
Minot State University
Minot, North Dakota
Bonnie McMillan Baxter, MS
Lakeland Regional Health Authority
Fort Saskatchewan, Alberta, Canada
David R. McCormack, PhD
Minot State University
Minot, North Dakota
Cheryl B. Gerard, PhD
Minot State University
Minot, North Dakota
INTRODUCTION:
Over the past several years, the literature has demonstrated children with significant prenatal alcohol exposure may experience marked deficits (Church and Gerkin, 1988; Jones, Smith, Streissguth Barr, Sampson and Bookstein,1994; Lemoine, Harousseau, Borteyru and Menuet, 1968). In 1973, Jones and Smith recognized a cluster of characteristics exhibited by children of alcoholic mothers, which they subsequently termed Fetal Alcohol Syndrome (FAS). Since that time, numerous investigators have contributed to a list of characteristics commonly found in children with FAS. Some of those characteristics are a discrepancy between verbal performance and effective communication, difficulty with conversational skills (''shallow speech''), impaired social skills, inattention, and general learning difficulties (Abkarian, 1992; Institute of Medicine [IOM], 1996; Nanson and Hiscock, 1990; Streissguth, Aase, Clarren, Randels, LaDue and Smith, 1991; Wekselman, Speiring, Hetteberg, Kenner and Flandermeyer, 1995).
Dysfunction within the central nervous system (CNS) is among the sequelae of FAS (Clarren, 1982). Decreased cranial and cerebellar size at birth, partial or complete agenesis of the corpus collosum, cerebellar hypoplasia and various hard or soft neurologic signs have been identified in children with FAS (Connor and Streissguth, 1996; IOM, 1996; Riley, et al., 1995). Additionally, Rossig, Wasser and Oppermann (1994) identified dysfunctions attributed to the brainstem in some individuals with fetal alcohol exposure. Other studies suggested exposure to alcohol throughout pregnancy appears to relate to: (1) deficits in encoding and sequencing information presented visually and through audition (Coles, et al., 1991); (2) possible deficit in rate of central information processing (Jacobson, Jacobson and Skol, 1994; Jacobson, Jacobson, Skol, Martier and Ager, 1993); and (3) slowed rate of information processing and difficulty retaining information, focusing, maintaining attention, and organizing information (Streissguth, Barr, Sampson and Bookstein, 1994).
The ASHA Task Force on CAP (Central Auditory Processing) Consensus Development (1996) defined CAPD (Central Auditory Processing Disorders) as a deficit seen in one or more of the following behaviors: ''sound localization and lateralization; auditory discrimination; temporal aspects of audition including temporal resolution, temporal masking, temporal integration, and temporal ordering; auditory performance decrements with competing acoustic signals; and auditory performance decrements with degraded acoustic signals'' (p.41). Keith (1995) described an auditory processing disorder as the ''inability or impaired ability to attend to, discriminate, remember, recognize, or comprehend information presented auditorily'' (p.101). Many investigators have linked CAPD to deficits in speech and language skills (Bellis & Beck, 2000; Chermak & Musiek, 1997; Keith, 1995; Koay, 1992; Lasky & Katz, 1983; Masters, Stecker, and Katz, 1998). Bellis and Beck (2000) also specified children with CAPD may demonstrate difficulty with reading and spelling skills, following complex directions, and may exhibit better nonverbal performance than verbal cognitive performance.
Given this background (above) information, it is not that surprising descriptions of listening and conversational skills of children with FAS are remarkably similar to descriptions of listening and conversational skills of children with CAPDs. Abkarian (1992) asserted that individuals with FAS often appeared to demonstrate more difficulty with comprehension and listening skills than with expressive language skills. Streissguth, et al., (1991; 1996) stated individuals with FAS generally have IQ scores in the low average range. Taking into account Keith's (1995) prerequisites of normal hearing and normal intelligence for a diagnosis of CAPD, it is possible the communication weakness in some individuals with FAS may be associated with CAPD.
The present study compared the performance of children diagnosed with FAS to age matched children without FAS, across five selected measures of central auditory processing.
SUBJECTS:
Sixteen children aged six to eleven years participated in this study. Eight of the children were diagnosed with FAS by the medical geneticist at the University of North Dakota School of Medicine. All of the children lived in either foster or adoptive homes at the time of testing. Children selected as controls were chosen from the same community or a similar urban center as the children with FAS and were matched within seven months of age. A hearing screening and tympanometry were completed to rule out hearing loss and/or middle ear pathology. The Comprehensive Test of Nonverbal Intelligence (TONI-2; Brown, Sherbenou, & Johnson, 1990) was administered to each child to ensure nonverbal intelligence was within normal limits.
PROCEDURES:
A graduate student in Communication Disorders tested each child under the supervision of a certified and licensed Audiologist/Speech-Language Pathologist. Each child was administered the SCAN: A Screening Test for Central Auditory Processing Disorders (SCAN; Keith, 1986), the child version of the Pitch Pattern Sequence (PPS; Auditec recording) and the Duration Pattern Sequence (DPS; Auditec recording). The tests were administered in random order to the children with FAS. The children in the control group were given the tests in the same sequence as their age-matched peers in the group with FAS.
RESULTS:
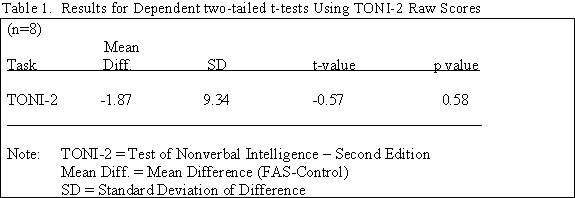
Dependent t-tests were used to compare the TONI-2 scores of the children with FAS to their age matched peers without FAS. The results from the dependent two tailed t-tests demonstrated the matched pairs did not show a great amount of variability. This suggested the subjects performed reasonably similar on this measure of nonverbal intelligence (see Table 1).
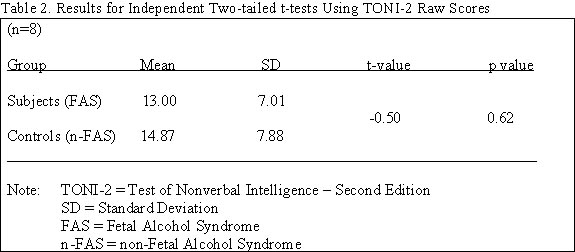
Independent t-tests were used to compare the overall mean scores of the two groups on the TONI-2. The two groups had similar variability on the TONI-2 scores, again suggesting subjects and controls were reasonably well matched on scores of nonverbal intelligence (see Table 2).
The CAPD data were analyzed in two ways. Dependent one-tailed t-tests were utilized to determine whether the scores of the children with FAS were significantly less than the scores of the their age-matched peers on selected CAP tasks. Secondly, the overall mean raw scores of the two groups of children were also compared with independent one-tailed t-tests. A probability level of (=.05 was chosen to indicate a statistically significant difference.
Table 3 shows the results for the dependent one-tailed t-tests performed on the CAP tasks. The individuals with FAS scored significantly lower (p

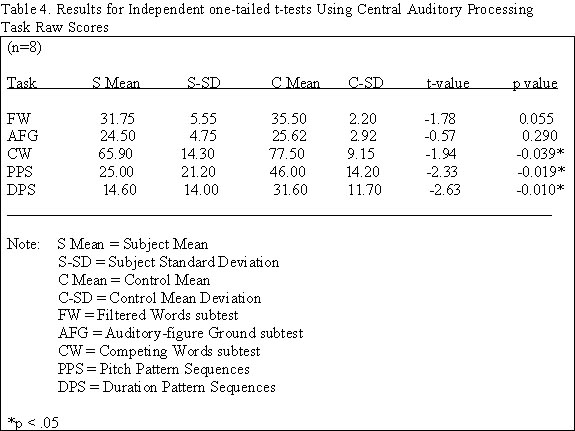
Table 4 shows the results of the independent t-tests. As a group, the children with FAS performed significantly lower than the children without FAS on the CW subtest, the PPS and the DPS. Significant difference was not demonstrated between groups on the FW and AFG subtests of the SCAN. In general, scores of the children with FAS showed more variability than the scores of the children without FAS.
SUMMARY:
In summary, statistical analysis revealed children with FAS scored significantly lower than children without FAS when raw scores of matched pairs were compared on dependent t-tests on all of the CAP tasks administered, with the exception of the AFG subtests of the SCAN. Likewise, when overall group means were compared with independent t-tests, the group of children with FAS scored significantly lower than the group without FAS on all the CAP tasks, with the exception of the AFG and the FW subtests of the SCAN.
DISCUSSION:
Significant between group differences were consistently identified in three of the five tasks (CW, PPS, DPS). The performance on the AFG task was not significantly different between groups. Between group differences on the FW task were observed when the performance of matched pairs was analyzed but not when the groups were compared as a whole.
These results invite interesting speculations. It has been suggested the tests used in this study may be associated with specific CANS lesions. Several studies have linked poor performance on CW, PPS and DPS tasks with underdevelopment or slower maturation of the auditory system, deficiencies in either hemisphere, damage to the corpus callosum, and damage to the temporal lobe (Keith, 1986; Bellis, 1996; Chermak and Musiek, 1997; Keith, 2000). Damage to these areas has also been associated with FAS. Rintelmann (1985) summarized numerous studies examining the effects of site of lesion associated with filtered word tasks. Performance on FW tasks was not significantly diminished in patients with damage to the interhemispheric auditory pathways of the corpus callosum.
Suspected neurological damage of the children with FAS in this study did not consistently interfere with FW and AFG tasks, but apparently diminished performance on CW, PPS and DPS tasks. The CW, PPS and DPS tasks included the additional demands for memory, cognition and language, as well as the coordination of these processes. Possibly, damage from FAS diminishes these processes, their coordination, or the combination of the processes and their coordination in tandem.
Regardless of neurological explanations, deficits in CW, PPS, and DPS skills have significant effects on receptive and expressive language skills, social interaction, and academic success. Children with deficits in pitch pattern and duration pattern tasks will obviously have difficulty understanding intonation and inflection. This will subsequently create difficulty understanding jokes, sarcasm, indirect directives and other common language forms, as well as difficulty with reading, spelling and writing skills. It is very difficult to read and spell efficiently when one cannot recognize stress and inflection of syllables, phrases and/or sentences.
It is noteworthy that children with FAS were able to withstand degradation of the acoustic stimuli on the FW and AFG tasks. Since there were no differences identified between groups in performance on these tasks, it is evident that enough integrity was maintained in the acoustic signal as it passed through the central auditory nervous system (CANS) and a significant disruption did not occur.
The performance of children with FAS on the five tasks of this study supports the idea of ''scattered'' auditory skills. Children with FAS are often able to perform well in some auditory environments such as understanding muffled speech or speech in noise. However, they may have more difficulty with other auditory tasks such as integrating auditory information into language. This is manifest in assimilating the components of pitch and duration as well as understanding language in the presence of competing speech. This discrepancy may give teachers, parents and interventionists the false impression ''listening skills'' may be ''selective,'' or possibly intermittent.
SUGGESTIONS FOR EDUCATIONAL MANAGEMENT:
This study suggests children with FAS demonstrate many behaviors consistent with CAPD. Therefore, central auditory processing skills must be evaluated in children with FAS in order to assess and provide effective and appropriate intervention. Management strategies may need to focus on skills related to competing words, pitch and duration patterns. A few examples of intervention areas related to deficits in CW, PPS and DPS are interhemispheric transfer tasks, use of strategies to improve organization of speech, language and general information, and direct training with the prosodic features of speech and language. Additionally, direct training on discrimination of duration and pitch differences of speech sounds, words, phrases and sentences may be necessary. Gillet (1993), Bellis (1996), Chermak and Musiek (1997), and Masters, Stecker and Katz (1998) provided many suggestions for remediation of deficient central auditory processing skills.
Additional research regarding CAP skills in children with FAS is necessary before permanent conclusions are drawn. Further investigation of left and right ear differences in children with FAS may provide information regarding hemispheric strengths and deficits. Investigation of children and adults affected by prenatal alcohol exposure with classifications other than FAS would be helpful in broadening the application of the present results. Additional studies, focusing on the educational and intervention process with these individuals, will be beneficial.
REFERENCES
Abkarian, G. G. (1992). Communication effects of prenatal alcohol exposure. Journal of Communication Disorders, 25, 221-240.
ASHA Task Force on Central Auditory Processing Consensus Development. (1996). Central auditory processing: current status of research and implications for clinical practice. American Journal of Audiology, 5 (2), 41-54.
Bellis, T.J., & Beck, B.R. (2000). Central auditory processing in clinical practice. Audiology Online. D.L Beck (Ed.) at http//audiologyonline.com
Bellis, T.J. (1996). Assessment and management of central auditory processing disorders in the educational setting: from science to practice. San Diego: Singular Publishing Group.
Brown, L., Sherbenou, R.J., & Johnsen, S.K. (1990). Test of nonverbal intelligence (end ed.). Austin, Tx: Pro-ed.
Chermak, G.D. & Musiek, F.E. (1997). Central auditory processing disorders: new perspectives. San Diego: Singular Publishing Group.
Church, M.W., & Gerkin, K.P. (1988). Hearing disorders in children with fetal alcohol syndrome: findings from case reports. Pediatrics, 82, (2), 147-152.
Clarren, S.K. (1982). The diagnosis and treatment of fetal alcohol syndrome. Comprehensive Therapy, 8 (10), 41-46.
Coles, C.D., Brown, R.T., Smith, I.E., Platzman, K.A., Erickson, S., & Falek, A. (1991). Effects of prenatal alcohol exposure at school age. I. Physical and cognitive development. Neurotoxicology and Teratology, 13, 357-367.
Conner, P.D., & Streissguth, A.P. (1996). Effects of prenatal exposure to alcohol across the life span. Alcohol Health & Research World, 20 (3), 170-174.
Duration Pattern Sequences (PPS) [cassette]. St. Louis: Auditec of St. Louis.
Institute of Medicine, Stratton, K.R., Howe, C.J., & Battaglia, F.C. (Eds.). (1996). Fetal alcohol syndrome: diagnosis, epidemiology, prevention, and treatment. Washington, DC: National Academy Press.
Jacobson, S.W., Jacobson, J.L., & Sokol, R.J. (1994). Effects of fetal alcohol exposure on infant reaction time. Alcoholism: Clinical and Experimental Research, 18 (5), 1125-1132.
Jacobson, S.W., Jacobson, J.L., Sokol, R.J., Martier, S.S., & Ager, J.W. (1993). Prenatal alcohol exposure and infant information processing ability. Child Development, 64 1706-1721.
Jones, K.L., & Smith, D.W. (1973). Recognition of the fetal alcohol syndrome in early infancy. Lancet, 2 999-1001.
Keith, R.W. (1995). Tests of central auditory processing. In R. J. Roeser & M.P. Downs (Eds.), Auditory disorders in school children (3rd ed.) (pp. 101-113). New York: Thieme.
Keith, R.W. (1986). SCAN: A Screening Test for Auditory Processing Disorders. San Antonio: Harcourt Brace Jovanovich.
Keith, R.W. (2000). SCAN: A Screening Test for Auditory Processing Disorders in children-Revised. San Antonio: Harcourt Brace Jovanovich.
Koay, M.E.T. (1992). Speech and speech disorders: implication for central auditory processing. In J. Katz, N. A. Stecker, & d. Henderson (Eds.), Central auditory processing: a transdisciplinary view (pp. 169-176). St. Louis: Mosby-Year Book.
Lasky, E.Z., & Katz, J. (1983). Central auditory processing disorders. Baltimore: University Park Press.
Lemoine, P., Harousseau, H., Borteyru, J.-P., & Menuet, J.C. (1968). Children of Alcoholic Parents: Abnormalities observes in 127 cases. Selected Translations of International Alcoholism Research (STIAR). Rockville, MD: National Institute on alcohol Abuse and Alcoholism. [Translation from the French of: Les enfants de parents alcooliques: Anomalies obervees, a propos de 127 cas. Ouest Medical )Paris), 21: 476-482].
Masters, M.G., Stecker, N.A., & Katz, J. (1998). Central auditory processing disorders:mostly management. Boston: Allyn & Bacon.
Nanson, J.L., & Hiscock, M. (1990). Attention deficits in children exposed to alcohol prenatally. Alcoholism: Clinical and Experimental Research, 14 (5), 656-661.
Pitch Pattern Sequences (PPS) [cassette]. St. Louis: Auditec of St. Louis.
Riley, E.P., Mattson, S.N., Sowell, E.R., Jernigan, T.L., Sobel, D.F., & Jones, K.L. (1995). Abnormalities of the corpus callosum in children prenatally exposed to alcohol. Alcoholism: Clinical and Experimental Research, 19 (5), 1198-1202.
Rintelmann, W.F. (1985). Monaural speech tests in the detection of central auditory disorders. In M.L. Pinheiro, & F.E. Musiek (Eds.), Assessment of central auditory dysfunction: foundations and clinical correlates (pp. 173-200). Baltimore: Williams & Wilkens.
Rossig, C., Wasser, S., & Oppermann, P. (1994). Audiologic manifestations in fetal alcohol syndrome assessed by brainstem auditory-evoked potentials. Neuropediatrics, 25, 245-249.
Streissguth, A. P., Aase, J.M., Clarren, S.K., Randels, S.P., LaDue, R.A., & Smith, D.F. (1991). Fetal alcohol syndrome in adolescents and adults. JAMA, 265 (15), 1961-1967.
Streissguth, A. P., Barr, H.M., Kogan, J., & Bookstein, F.L. (1996). Understanding the occurrence of secondary disabilities in clients with Fetal Alcohol Syndrome (FAS) and Fetal Alcohol Effects (FAE). Seattle: University of Washington Publication Services.
Streissguth, A. P., Barr, H.M., Sampson, P.D., & Bookstein, F.L. (1994). Prenatal alcohol and offspring development: the first fourteen years. Drug and Alcohol Dependence, 36, 89-99.
Wekselman, K., Spiering, K., Hetteberg, C., Kenner, C., & Flandermeyer, A. (1995). Fetal alcohol syndrome from infancy through childhood: a review of the literature. Journal of Pediatric Nursing, 10 (5) 296-303.
