
Readiness Management is the collection of best practices that can assist in moving a patient who shows some level of interest in obtaining amplification to the point of trial use in a way that maximizes the chance for a positive outcome.
It is a well recognized reality in our field that only a minority of the patients who could benefit from amplification actually use hearing devices (Kochkin, 2000). Many patients enter the hearing care process, yet decide not to pursue amplification. Others obtain hearing devices but decide to either return them or simply stop using them. In order to reach more patients with our services, it is essential that professionals better understand the mindset of the potential hearing device user. We need to understand what prevents potential users from seeking out treatment, what creates hesitancy to follow through with fitting recommendations and what factors can derail new fittings. There are millions of individuals whose communication performance could be positively impacted through the provision of amplification. However, the decision to use amplification is a voluntary one on the part of the patient. It is incumbent upon our profession to best understand the situation from the patient's point of view so we can do all that we can to create more positive outcomes.
For a number of years, our field has operated under certain assumptions. For example, we believe that patients are reluctant to use amplification because of age-related stigma concerns and also concerns about costs and ease of use. However, oftentimes these assumptions have not been based on careful, large-scale studies but rather as an accumulation of clinical experience. More careful studies have challenged some of these assumptions. For example, Ramachandran, Stach & Becker (2011) recently have reported that uptake of amplification does not seem to be affected by reducing the cost. In recent years, more attention has been paid to systematic studies of the viewpoints, assumptions and opinions of those who could potentially make use of amplification.
In this paper, we will review recent data that has been collected from potential first time users of amplification, including the main results from a large scale international survey initiated by Oticon. In a companion paper (Oliver & Palmere, 2011), strategies for getting more potential users to enter the hearing care process are discussed. Here we will present an approach ("Readiness Management") designed to move the patient who shows some level of interest in obtaining amplification to a point where they are ready for the first fitting experience.
The Patient's Viewpoint
The following are transcripts taken from interviews with four different individuals who suspected they had some amount of hearing loss but had yet to enter the hearing care process.
Patient 1: Do you know anyone personally who has had a hearing loss?
My mother-in-law used to wear hearing aids, it was frustrating for her. She had trouble getting them in and wax in her ears was a big frustration for her. Because of that, I am hesitant to embark on them. I have seen the different sizes, and I would want them to be really tiny and not too loud, like a megaphone coming out of my ear - not too magnifying.
Patient 2: When did you first suspect that you had a hearing loss?
Within the last 6 months to a year. I am noticing not picking up on conversations. Recently I was with an old friend I hadn't seen for a long time. After five days being together she asked me if I had a hearing loss. When I don't understand what someone is saying I will ask them to repeat what they said. Doesn't affect my life at this point. My husband has said something also, but that doesn't matter!
Patient 3: What aspect of this whole process, either being evaluated or seeking treatment or something else, is the most concerning for you? Why?
Initial thing of going there and realizing that I do need a hearing aid — something I don't want to have. I don't like it . . .the thought of getting really old.
Patient 4: Do you know anyone personally who has had a hearing loss?
Good friend that I fish with, I think it is congenital or runs in the family. For a long time he has been wearing a hearing aid and when we go fishing he doesn't wear it so I have to get his attention another way. He is doing well with it and pleased. Jim at church wears one. They are getting along fine.
Have your friends or family expressed concerns to you about your hearing?
Just my wife - I think her concerns are valid.
What is striking about these four different sets of statements is that the concerns expressed by the patients vary significantly. For example, Patient 1 seems be focused on the difficulties that other people have expressed about hearing aids, whereas Patient 3 seems to be more focused on the age-related symbolism of hearing aids. Patient 2 seems to be minimizing the effects of the hearing loss, whereas Patient 4 seems to recognize that the hearing loss may be causing difficulties. These four examples represent a cross-section of the patient's who enter hearing care clinics and offices all around the world every day. By recognizing and analyzing this range of concerns expressed by patients, we believe that hearing care professionals can more effectively serve those who truly would benefit from the provision of hearing devices. Our goal is to provide suggestions on how patient counseling can be best tailored to the specific concerns expressed by patients when they enter the process.
Past Research on First-time Users
Concerns and Expectations
First-time hearing instrument users have many concerns when deciding to acquire their first hearing aid: practical issues, self image, technical concerns, dispenser service and counseling and other things. Many first-time users have gone through a long and hard recognition process to get to the point where they wish and are motivated to acquire a hearing instrument (Engelund, 2006). They have expectations and preconceptions of how it is to wear hearing instruments and what benefit they will receive from the amplification, but these preconceptions may be vague or inaccurate. Classically, it has been observed that first-time users have expectations that exceed actual obtained benefit (e.g., Schum, 1999; Wong, Hickson, & McPherson, 2004).
Some new hearing instrument users may not have formed a clear expectation of the benefit and potential difficulty associated with the provision of hearing aids (Wong et al., 2004), though they might have instinctive ideas of positive effects and problem areas when probed or confronted with the questions in pre-fitting ("expectation") questionnaires. The lack of expectations may be due to the fact that very few individuals have experiences with amplification of any kind before having acquired their first hearing aid. The expectations are thus built on the accounts of others (Bisgaard, 2008).
The anthropological study by Bisgaard (2008) described the coping associated with emergent hearing loss and, more specifically, the expectations and experiences of new hearing aid users. The study was conducted by interview, by telephone, in person and by email correspondences with the interviewer. The participants were 41 individuals randomly selected from both private clinics and hospital audiological departments in Denmark. Of the 41 participants, only 4 individuals deselected amplification (became non-users) after having tried it out. The participants had only vague expectations to acquiring a hearing aid. They wanted to "hear better", but did not have more specific expectations. Any prejudices were based on the accounts of others: colleagues, family, friends, etc. Some of the participants described that they had trouble defining how well they would hear with the provision of amplification, because their hearing had progressively worsened over the years and "normal hearing" had become a vague concept.
The expectations to the hearing instruments might not be met in the course of the first months, but after a year the perceived benefit may fall in line with expectations (Saunders & Jutai, 2004). Moreover, the expectation to amplification may change with use: at first the physical appearance and comfort of the aid may be most important while the sound quality and the resulting listening effort may become more important variables with experience (Oticon A/S, 2010). Nonetheless, recent work by Schum and Pogash (2011) and Smart, Kreisman, Robinson, Marczewski and Butler (2011) has indicated that typical first times users will report benefit right from the day of the fitting.
Performance Over Time
The auditory acclimatization effect is described as a change in auditory performance with time in response to a change in the acoustic information available to users of hearing aids or cochlear implants. This change in auditory performance cannot be accounted for purely by task-related training (Arlinger, Lyregaard, Billermark, & Öberg, 2000). Although the initial fitting of amplification will improve performance compared to going without hearing devices (e.g., Kreisman, Mazevski, Schum & Sockalingam, 2010), the full benefit may take up to six months to be realized (e.g., Gatehouse, 1992). On the other hand, some authors have noted that full acclimatization occurs during the first month, both in novice and experienced users (Kuk, Potts, Valente, Lee, & Picirrillo, 2003). The acclimatization to hearing aids can likewise affect unaided speech perception, the increased sound exposure and perhaps awareness of sound can influence speech perception (Reber & Kompis, 2005).
While general agreement is found on the benefit of hearing aid versus no hearing aid (Lindley, 2008; Arlinger et al., 2000), equivocal accounts are found on the preference of gain of new users. Some find that first-time users may prefer less than normal loudness and less gain in the beginning (Marriage, Moore, & Alcántara, 2004; Smeds, 2004). The lesser amount of gain (~2 dB) can provide the same speech in noise perception as the prescribed amount (Smeds, 2004; Keidser, O'Brien, Carter, McLelland, & Yeend, 2008). Soft sounds can be perceived as too loud for first-time users, before they grow accustomed to them (Laugesen, Vestergaard, & Nielsen, 2005). Others find no difference in the preference in gain at the initial fitting and no change in the preference in amount of preferred gain (Convery, Keidser, & Dillon, 2005). Finally, some find a preference for the prescribed gain (Arlinger et al., 2000).
Negative Experiences
One of the widely held beliefs in our field is that it takes time to adjust to the negative side effects of using amplification (e.g., Dillon, 2001). Further, it is believed that first-time users are more likely to experience side effects compared to experienced users. A study by Laugesen, Vestergaard, & Nielsen (2005) examined four known preconceptions of the differences between first-time users and experienced users. The method of obtaining data was by self-report by the users. 196 hearing aid users participated in the study. The four preconceptions were that new users are 1) more bothered with occlusion and the sound of their own voice, 2) perceiving soft sound as too loud, 3) disliking the high frequency amplification and 4) less aware of the complexities in every day sound environments and less aware of the compromises involved with hearing aids than experienced hearing aid users.
The authors found no evidence supporting suppositions 1, 3 and 4. Experienced users are equally bothered with the sound of their own voice but apparently they accept its inevitability and stop complaining about it when seeing the audiologist. The second preconception, that soft sound are too loud for new users is strongly verified/confirmed. Correlation was found with threshold and type of hearing loss.
However, advances in the control of side effects such as occlusion, acoustic feedback and discomfort should cause us to re-examine the assumption that side effects are inevitable. Schum & Pogash (2011) and Smart et al. (2011) examined the subjective evaluation of side effects for first-time users at the day of the fitting and at 5 other points during the first 30 days of device use. All patients were using advanced technology, mini-RITE devices. Many of the fittings were open and most patients were fit using adaptation management. Both studies found a low occurrence of side effects even from the day of the fitting.
The Patient Journey
Since most patients develop hearing loss over a number of years, it is not clear precisely when they identify themselves as being hearing impaired. Extensive studies have been conducted on the process from becoming aware of the emergent hearing loss to the decision to acquire a hearing instrument.
Engelund (2006) defined a four-stage recognition process that individuals with hearing loss go through: attracting attention, becoming suspicious, sensing tribulation and jeopardizing fundamental self. An emergent hearing loss may become apparent in situations where hearing ability is seen as "unpredictable" (Engelund, 2006). Unpredictable hearing can be related to problems with audibility, localization, detection, and/or intelligibility. Problems with different aspects of hearing can lead to unsuccessful or inappropriate communication where misunderstandings or non-understandings occur more or less frequently.
Besides the more "tangible" hearing-related situations, the problems with hearing are manifested in a great deal of disappointments and confusion in the relations with others. Engelund divided these forms of troublesome and unsuccessful communication into two categories; relational tribulations and personal tribulations. The relational tribulations concern how individuals experience the impact of their hearing loss on other people and their interaction. Thus, relational tribulations affect an individual's social identity - the consequence of how individuals see themselves through others' reactions to them. The personal tribulations concern the impact of the hearing loss on an individual's self-concept and self-esteem. The consequences of the related problems and their manifestation are the change in self-identity. Having one's self-identity challenged is one of the major triggers in the recognizing process; when being faced with or reflecting upon the problematic changes in interpersonal relationships that are occurring, the hearing impaired individual will understand that something has to be done. The problems are no longer solvable without professional intervention. The hearing loss will worsen and personal hearing tactics will fail. The hearing impaired individual is faced with the need to confront the hearing impairment and, hopefully, is motivated to change the situation (Engelund, 2006).
Predicting Patient Behavior and Experience
Since only a minority of individuals with hearing loss will obtain amplification and not all of those fittings are successful, there is a deep interest in understanding the factors that may predict who will or will not seek out treatment and whether or not that treatment will be successful. For example, Garstecki and Erler (1998) found that the single strongest predictor of whether or not an older patient will follow through on the recommendation to obtain amplification was locus of control. Patients who had a stronger sense that they controlled their own destiny were more likely to seek out treatment for their hearing loss.
Knudsen, Oberg, Nielsen, Naylor & Kramer (2010) performed an extensive search of the literature covering studies that examined which variables predict help seeking, hearing aid uptake, use, and satisfaction. The authors identified 39 empirical studies published in the period between 1980 and 2009. A total of 31 factors have been examined in these studies, including source of motivation, expectation, attitude, measured hearing sensitivity, age, gender, cost, etc. The only factor that was consistently predictive of whether or not a patient will seek out treatment, obtain amplification, use the devices and experience benefit was self-reported hearing difficulty. Clearly, a patient must feel the effect of the hearing loss in daily life in order to be motivated to enter the hearing care environment and see the process through.
Oticon Patient Experience Survey
In 2010, Oticon initiated a large-scale, international survey of both potential users and existing users of amplification. Responses were obtained from 1450 individuals, 750 individuals who suspect they have hearing loss but have yet to obtain amplification and 700 individuals who are current hearing aid users.
The web-based survey was conducted in the United States, Germany, France, Canada and Italy. The data from the non-users provides a wealth of insight into the mindset of those contemplating what to do about their hearing difficulties. A variety of domains were examined, including expectations, concerns and potential motivational drivers. The results reveal much about how these individuals are reacting to the emergence of hearing difficulties, why they have yet to act, but also what could potentially cause them to take the next step.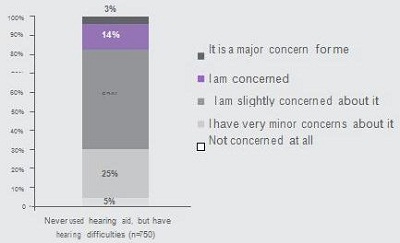
Figure 1. Response of 750 non-users to the question "How concerned are you that this (hearing difficulties) is a problem?" from Oticon A/S (2010).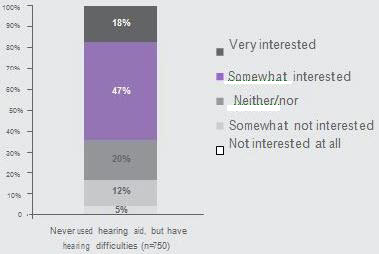
Figure 2. Response of 750 non-users to the question "How interested are you in a solution to your hearing difficulties?" from Oticon A/S (2010).
Figures 1 and 2 provide an intriguing look at the mindset of the non-users. Recall that these patients responded to the survey because they recognized that they were experiencing some changes in their hearing. In Figure 1, the results to the question "How concerned are you that this (hearing loss) is a problem?" Notice that only 17% of the respondents indicated that hearing loss is either "a concern" or "a major concern". However, now look (Figure 2) at the responses to the question "How interested are you in a solution to your hearing difficulties?" Now, nearly two-thirds of the respondents are either "interested" of "very interested". So, although the large majority does not respond as if the hearing loss is a concern, they still want information about treatment options.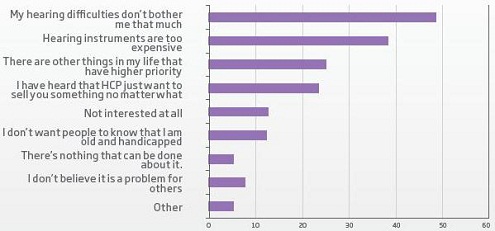
Figure 3. Response of 570 non-users to the question "Have you ever considered contacting a hearing care professional but refrained from doing so because:" from Oticon A/S (2010).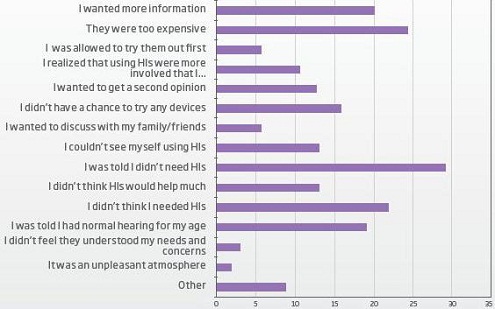
Figure 4. Response of 134 non-users to the question "Why didn't you buy hearing instruments at your first consultation?" from Oticon A/S (2010).
When asked why they have not talked to a hearing care professional (Figure 3), the most common response is that the "hearing difficulties don't bother me that much", followed by concerns about cost and stigma. For a subset of patients who did talk to a hearing care professional but did not obtain amplification, when asked why (Figure 4), a similar range of reasons emerge: not a big enough problem, cost, time & trouble, stigma, etc.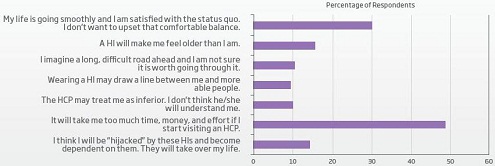
Figure 5. Response of 749 non-users to the question "Which 2 statements best describe your worries or concerns ahead of visiting a hearing care professional?" from Oticon A/S (2010).
This wide range of themes continues when looking at the responses to the question (Figure 5) "describe your worries or concerns ahead of visiting a hearing care professional". As was seen at the beginning of this paper in the interviews with individuals contemplating obtaining amplification, the palette of issues is broad. It is not just cost and it is not just stigma. Those factors are there, but others are present also. The patient may be concerned about the overall "hassle" of dealing with a new set of challenges, a new health care professional and another thing to worry about. Others may have been looking for someone to validate their desire to not do anything (even though this may not be exactly what the hearing care professional actually said). Others may not trust where this journey will lead them.
Reaction to the Aging Body
We are not the only professionals who deal with age-related changes in body function. The human body experiences age-related changes in nearly all aspects of form and function. Although we may view hearing loss in isolation, the patient may not. Hearing loss may be perceived as just another aspect of inevitable body decline. In fact, the loss of hearing may actually occur relatively late in the process when compared to many other age-related physical changes (vision difficulties, hair loss, arthritis, diabetes, strength& flexibility loss, loss of endurance, menopause, sexual dysfunction, etc.) The patient's reaction to the emergence of hearing loss may be tied to a broader, generalized reaction to the physiological effects of aging.
There is a rich literature that has been developed by other health care and behavioral scientific fields that speaks to the emotional reaction to the aging process (e.g., George, 2001; Leventhal, Rabin, Leventhal, Burns, 2001; Whitborne, 2002). Audiology is not the only field that witnesses reluctance of older patients to take positive steps towards dealing with age-related body changes. The lessons learned by these related fields provide us some with interesting viewpoints on interacting with these patients.
For example, normalization refers to the tendency for some older individuals to respond to body changes as simply part of the normal aging process and that compensation is not necessary. The person simply accepts the loss of function. Compensation is seen as optional and many individuals may simply decide to not take action. Remember, a lot of things about the human body change over the years. What should be brought to the attention of a health care professional versus what is just "normal" may not be clear to the person. Many older individuals will have the attitude that you simply cannot fix everything that changes in the body. Hearing may be considered one of those functions that should be expected to go over the years. Although it is desirable for the aging person to be realistic about body change, the key issue is: What does it take to be motivated to take the steps necessary to compensate?
Further, aging will challenge a person's sense of self worth. As the years progress and the physical effects of aging take hold, the roles that a person has always played may start to change. Lifestyle changes will be inevitable. Some tasks will become more difficult. Some favorite activities may have to be abandoned. Mental health professionals emphasize the importance of a healthy self-identity in the aging person, as strong mental health has been tied to physical well-being (Skaff, 2007). The decline in hearing abilities is another one of the challenges to a person's sense of self. Familial, occupational and social relationships will also go through changes. The risk of isolation increases as interactions with friends or family may become less frequent. Important roles in life may be eroded as the person leaves the workforce and may perhaps pull back from other important service positions. This erosion of self-confidence may act to de-motivate the person from taking positive steps to maintain effective social abilities, such as seeking out amplification. Amplification is a form of secondary control mechanism -- compensation strategies that can be adopted to make up for the loss of primary control or function. McConatha & Huba (1999) point out a strong link between the adoption of secondary control mechanisms and a sense of self confidence and self worth in older individuals. Both George (2001) and Leventhal et al. (2001) stress that self-efficacy (the belief that a person has the ability to successfully perform a task or meet a goal) is an important component to making a successful health care change in older patients. The hearing care professional plays a key role to engender the desire to make a change and the confidence that change is possible.
Hearing care professionals see the patient at a specific point in time. The natural tendency is to feel that, if a hearing loss is established via audiometric testing, it seems sensible that compensation (i.e. amplification) should be applied. However, the patient may see the situation differently. The hearing loss typically will have developed slowly over the course of several years. The patient has been compensating for the loss of function, perhaps even without being aware of the adjustments to behavior and lifestyle. Other life changes may have acted to reduce the size of the person's social circle and the frequency of challenging communicative interactions. Basically, the person is getting by. The patient may simply lack the inherent motivation to take on a major new life challenge (obtaining, accepting and adjusting to amplification). Further, since older individuals have faced a series of body changes over the years, what alterations in function represent a "health condition" versus simply normal changes may be unclear. The hearing care professional may define it as a "hearing loss" but the patient may simply define it as "my hearing". It may not be the same as when I was younger, but it is normal for my age.
Commitment to the Process
In a recent pair of studies described above (Schum & Pogash, 2011; Smart et al., 2011), the subjective and, in the case of the Smart et al. (2011) study, objective performance of first-time users was evaluated several times over the first month of use. One unique aspect of this pair of studies was that the patients were asked two questions concerning their commitment to the process of being a hearing instrument user: (1) How happy are you with your decision to get amplification? (2) Do you see yourself as a long-term, permanent user? The patients responded on a 1 to 5 scale, with 1 indicating Very Unhappy and Very Unlikely, respectively, and 5 indicating Very Happy and Very Likely, respectively.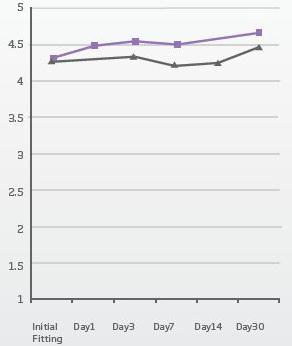
Figure 6. The responses of 24 first-time users to the questions "How happy are you with your decision to get amplification?" and "Do you see yourself as a long-term, permantent user?" at various times during the first month of hearing device use from Schum &Pogash (2011).
The results for those two questions are presented in Figure 6 for the patients from the Schum and Pogash (2011) study. The mean ratings for this group of patients started high even on the day of the fitting and remained high during the first month of device use. At six months post-fitting, all of the patients were still using the devices and were generally satisfied. The data from the Smart et al. (2011) study were quite similar. These results may catch some professionals by surprise, since it is often assumed that patients may withhold judgment until closer to the end of the (typical) 30-day trial. What these findings suggest is that, although there may be many barriers that keep patients from obtaining amplification, once the patient commits to obtain hearing devices, they have a positive mindset. This further puts focus on the activities that the professional can do to prepare that patient for the fitting.
Readiness Management
The awareness of hearing loss and the decision to enter the health care system is not immediate; it may evolve over several years. Patients raise their hand at different stages in the process - some are more ready to take the next step than others. We want to know what can we do to make sure as many of these patients as possible are prepared for a successful fitting experience. The question is: What can we all do to make sure the first-time user is in the right state of mind to maximize the chances of a successful fitting?
When a patient raises their hand and enters the hearing care environment, that person may view the process in different ways. For some patients, interactions with hearing care professionals may take on a transactional feeling. They may approach the process of potentially obtaining amplification from a cost versus benefit viewpoint. In a very logical way, they may line up the possible benefits of amplification with the expected costs which may include both financial and lifestyle implications. Other patients may view the process from a medical standpoint: they have a health condition that may need treatment, and they are seeking out the advice of a qualified professional. Finally, another group of patients may view the idea of getting amplification as a major life change decision. These patients may be dealing with the question of whether or not they are ready to become a hearing aid user. The idea of becoming a hearing aid user may be emotionally laden, representing a new, negative chapter in their life.
The hearing care professional needs to recognize that the thought of getting amplification may mean significantly different things to different patients. Again, the final decision rests with the patient and it is a voluntary choice. The role of the professional is to provide appropriate information and advice to the patient and the family members. This information and advice (i.e. counseling) should meet the patient on the patient's terms. Having a detailed discussion of features, options and costs with a patient who is struggling with age-related stigma issues may be counterproductive. On the other hand, a patient who wants to believe they're getting the appropriate technology for a fair price may desire to have a detailed discussion of hearing aid features and functions.
Based on the range of findings discussed above, we believe that there are four classic sets of behavior that potential first time users will demonstrate. Further, these classifications of behavior are not mutually exclusive: some patients will show behaviors from different categories. However, we believe that there is value in categorizing the dominant behaviors shown by a patient when they enter the hearing care process. The better the professional is at matching the counseling approach to the behavior patterns shown by the patient, the greater is the likelihood of a successful process.
Hearing care professionals recognize that not all fittings with first-time users are successful. We want to examine more closely the interactions between the hearing care professional and the first-time user to try to increase the success rate of fittings - everyone wants more satisfied, long-term successful users. Readiness Management is the collection of best practices that can assist moving a patient who shows some level of interest in obtaining amplification to the point of trial use in a way that maximizes the chance for a positive outcome.
Most Prevalent Behavior Patterns
Our work and the work of many others on the nature of the concerns of first-time users has lead us to believe that there are, in general, four major patterns or drivers of behavior. We broadly divide the patients into the Willing and Reluctant categories. Not all first-time users are reluctant, some are actually willing. But just because a patient is willing to be fit, that does not mean that person is totally ready for amplification. Additionally, just because a person is reluctant, that does not mean they are unwilling: they have taken the first step. For those who are reluctant, they may be reluctant for very different reasons. We believe that there are three major reasons why a patient may be reluctant.
We do not see this as suggesting that there are four distinct types of patients. Rather, we see four dominant patterns of behavior. Any patient may show combinations of drivers. Further, throughout the process of recognizing and acting upon the hearing loss, any patient may move from showing one type of behavior to another.
Let's take a closer look at these dominant behavior patterns.
Willing.
The patient who is demonstrating willing behavior recognizes the hearing loss and is ready to move forward. They tend to be emotionally comfortable with the notion of obtaining hearing devices. They are approaching the decision-making process in a rational manner. They approach the process with a "let's get this done" attitude. They know they have a hearing loss and that amplification should address the situation. They may have done extensive research ahead of time, even down to brand and pricing information. They may see this as a business transaction or they may see the process as a condition-treatment situation.
The question is whether or not the patient is acknowledging the difficulties created by the hearing loss. Do they feel the pain enough? The reason why this is important is that if the patient is only acting on intellectual, rational grounds and if the hearing instruments do not provide full expected benefit, they may logically assume that amplification was not the right option. Of course, it is a positive sign that the patient is willing to be fit with amplification. However, if the process moves too quickly and the patient has not taken the time to explore the true nature of the effect of the loss, the process can end in returned devices.
Review the interview with Patient 4 from the beginning of this paper. In general, this patient appears willing to be fit with amplification. He has reported two cases that he is aware of with positive results and he is acknowledging that his wife's concerns about his hearing are likely valid. Further questioning with the patient should likely focus on the specific situations with which he struggles. It is not enough that his wife has noticed problems. His decision to pursue amplification cannot just be because his wife sees the need. He must feel and, importantly, express the need himself.
Reluctant - Normalizing.
The patient showing normalization behavior may view hearing loss as an inevitable part of that aging process - something that you just have to put up with. They recognize the hearing loss, but not the need to do something about it. They may tend to be passive, perhaps with an external locus of control. They may be ambivalent about their hearing loss because of the low motivation to make a change. They know the loss is there, but they also know that amplification is optional and they do not see it as an option for them. Perhaps the erosion of self-confidence that can occur with some older individuals has led them to think that they may not perform well with amplification or will run into adjustment problems. They are waiting for a professional to tell them that they have to make a change. They may interpret a statement from a physician or hearing care professional that obtaining hearing aids is a good but not necessary step as permission to not take action.
The patient showing normalizing behavior needs to develop the motivation to make things better. Perhaps they are not fully recognizing the impact of the hearing loss, especially on loved ones. They may not associate their shrinking social circle as a result of communication difficulties. Perhaps they simply do not see how much better things could be.
The interview with Patient 2 at the beginning of the paper demonstrates some classic normalizing behavior. She acknowledges that she is missing things and that other people pick up on it. However, she dismisses her husband's concerns and she also indicates that she can continue to get by. Perhaps there is more going on with her. Maybe she minimizes the effects of the loss because she truly does not want to take action, but at least on the surface, she makes it clear that she does not see the hearing loss as a large issue.
Reluctant - Wary.
Patients who are showing wary behavior are concerned about the practical realities of obtaining and adjusting to amplification. They may be concerned about the expense of the devices, the adjustment process, the side effects or the potential lack of benefit. They may have heard from others over the years about problems with amplification. They may be concerned that they will spend a lot of money and may not get the value they expect. They may feel that they are getting by, so they may not want to put up with the downsides of the fitting process. For them, it is a clear cost— benefit calculation and they are already suspicious of the negatives. They may well recognize the presence of hearing loss and the resultant communication struggles, but they also expect problems.
For patients who show wariness, their concerns may be valid, or they may be masking something else. It is true that there are truly wary people: individuals who want to know the full picture before they can commit to a change. This will be especially apparent for those who see the obtaining of amplification as a transaction. On the other hand, if a patient is having difficulty accepting the fact that they have a hearing loss or if they are minimizing the effects because they lack the confidence to make such a big decision or take on a new challenge, then they may throw up a lot of practical objections. They may or may not truly be concerned about the practicalities, but it is a way to avoid discussing perhaps a deeper issue.
The interview with Patient 1 demonstrates classic language from a patient showing wary behavior. She brings up a series of concerns that she has either heard of or seen firsthand. Perhaps she is bringing these objections because she is trying to avoid talking about other issues, such as her reluctance to accept the idea of using hearing aids. On the other hand she may feel that the downside of using amplification may be simply too high. Either way, the hearing care professional needs to discuss these stated concerns first and foremost and avoid being dismissive of such practical objections.
Reluctant - Conflicted.
The patient showing conflicted behavior represents the classic view of the reluctant patient: they are focused on struggling with accepting the aging process and feel that obtaining hearing aids may be a negative watershed point in time. They probably are well aware of the communication problems that they are having and truly wish that things could be better.
However, they cannot get by the block of what hearing instruments mean. The conflict comes from the competing desires to perform better in communication environments but to avoid getting amplification. They know they should... they just can't.
As a starting point, new users often consider it shameful to be dependent on a technological device, the purpose of which is to overcome a physical deficit" (Bisgaard, 2008). There is an inherent contradiction when the user wants the advantages of the technology, but not the image that comes with technology itself (Bisgaard, 2008); the user does not want to display what they consider a physical or even cognitive deficit.
Patient 3 lays her cards right out on the table: she does not feel she is ready to accept amplification. Oftentimes, the patient showing difficulty accepting the notion of using hearing devices is not quite as frank as this patient. They may talk around the issue more. Clearly, the stigma of being seen as a hearing aid wearer weighs heavily on the mind of many people who have come to realize that they probably are experiencing age-related hearing difficulties.
It is important to point out two important aspects of patients' agendas. First, many patients will have hidden or otherwise unstated concerns. For example, a patient may spend a lot of time talking about the practical problems of using amplification when, in actuality, the real concern is related to a perceived, age-related stigma.
The professional has the responsibility to respect the stated concerns of the patient and respond appropriately. However, that professional also has the responsibility to be aware that the real objections may lay deeper and that some probing may be needed to bring those issues to the surface. Secondly, any given patient may show a mix of issues. Perhaps the patient truly feels that the hearing loss is not that significant and that the cost (in terms of time, effort and money) is great. Another patient may express a willingness to move forward, but there are lingering, stigma-related concerns that are still not fully resolved. The counseling strategy developed for each patient must take into account the true complex of issues faced by each individual patient.
Making a Patient "Ready"
The first step in establishing an intervention plan is to determine the outcome goals. What makes a person ready to be fit with amplification? We believe that the following factors are important:
- Trust: the patient must feel trust in three key areas.
- Trust in the professional that is providing the care
- Trust in the products that are recommended as part of the care package
- Trust in themselves that they are making the right decision
- The patient must emotionally feel the effects of the hearing loss. There needs to be a sense of urgency that the hearing loss is affecting daily life, and that situation must change.
- The patient must take ownership of the solution
- The patient needs to have realistic expectations of the process
The goal is to create a positive environment for success so that the patient feels that they are doing the right thing and are working with the right person. They must recognize that the hearing loss is complicating their life and the lives of their loved ones. They have to recognize that they are the only person who can make the decision to move forward in the process. Finally, they have to recognize the inherent limitations of hearing loss and understand what their life will be once amplification has been obtained. Although different patients will enter the process with a different agenda and mindset, it is reasonable to expect most patients to move to a point where these four criteria are met and the fitting process can start. It may take only a few minutes of discussion with the patient and family members to recognize that the patient truly is ready to start the fitting process. For other patients, however, the discussion may be longer and the path that the discussion takes is very much determined by the primary concerns expressed by the patient or loved ones.
Readiness Strategies
Why spend the time to examine the patient's mindset? The optimal counseling approach will vary depending on the major concerns of the patient. The better the professional can understand the patient's agenda, the better are the chances of moving the patient to the best place for success: a place that allows good technology and good fitting practices to help the patient to the greatest extent possible.
First, the professional should determine how the patient views the process. Is this a transaction? Is this a health care decision? Is it a life change decision? That does not mean that the professional has to have three different and distinct counseling approaches. However, it does mean that the professional may need to adapt the intervention approach to take into consideration the assumptions of the patient. A patient who sees the decision to obtain amplification as a major life-change event may not respond well to a professional who is talking about a lot of technical features. A patient that has a transactional mindset may not respond well to a lot of discussion of the emotional impact of the hearing loss . . . at least not initially. The professional needs to recognize where the patient is coming from and start the discussion in a similar universe. Perhaps there will be value in reframing the effect of the hearing loss in another way in order to make the patient ready, but that can only take place if the professional at least starts where the patient is.
Next, the patient's initial descriptions of why they are seeking out care should be evaluated to look for any dominant behavior patterns. Does the patient seem willing or reluctant? If the patient seems willing to move forward, then the process becomes focused on what is needed to make sure that the patient's initial experiences are positive.
If the patient seems to be reluctant, what seems to be the nature of the reluctance? Cost? Minimization of the effects of the hearing loss? Concerns about practical problems using amplification? Concerned about what it "means" to be a hearing device user? Suspicion that they are going to be taken advantage of? Determining the specific nature of the patient's reluctance will help to focus the discussion on the most relevant issues.
Once the professional has identified the types of major behaviors being demonstrated by the patient in the initial interview, it is time to develop a strategy for intervention. Clearly, different discussions are needed depending on the core issues exhibited by the patient. One counseling or sales tactic approach cannot possibly make sense for all four major types of behavior. Further, it is likely never as simple as picking one of the four profiles and categorizing the patient cleanly. Nearly all patients show some subtle variations on a behavior pattern or a mix of types of issues. The hearing care professional needs to quickly decide how to frame the ensuing discussion with the patient and be ready to change approaches as potentially deeper concerns are expressed by the patient.
Once an overall strategy is identified, then the question turns to whether or not additional tools may help move the patient forward. In many cases, the professional may feel that simple discussions with the patient and family will be sufficient to bring the person to a point where they are ready for a fitting. In other cases, additional counseling tools may make sense. Each professional will have a different viewpoint and comfort level with different tools. A tool should never be seen as a substitute to effective counseling, and it should never get between the patient and professional. Tools should be used if they fit naturally into the counseling style of the professional and are appropriate for the concerns expressed by the patient.
A variety of tools exist to support the chosen strategy. We broadly divide the purpose of tools into those that can help motivate the patient to take action and those that can help confirm that the patient made the right decision. Any given tool may be able to meet both purposes. For example, the Ida Institute (2009) has developed a series of tools to help to evaluate and potentially increase the motivation level of the patient. The Line can be used to discuss with the patient their current level of motivation and spur a discussion of what it would take to enhance that motivation to change. The Box can help in laying out both the pros and cons of continuing without amplification versus moving forward. The COSI (Dillon, James & Ginis, 1997) has been available for nearly 15 years and, when used as a counseling tool, can assist in focusing the process on the most important needs of the patient. The Patient Expectation Guide (Schum, 2009) can help to allay the concerns of the cautious patient and give them the confidence that they can trust the professional and the products that are recommended.
Genie software tools such as eCAPS and the Activity Analyzer can assist in informing the patient of the role of advanced technology. For patients who have moved to the point of at least trying amplification on a demonstration or at-home trial basis, these tools can confirm to the patient the value of the sophisticated processing of advanced products. The COSI, used after some period of trial use, can help to demonstrate to the patient that the devices addressed the most important concerns expressed by the patient.
Appendix A provides an overview of several of the most relevant tools for the counseling of first-time users. Specific use scenarios are proposed. With the understanding that patient counseling is never a neat, systemized process, let's examine the key components of a counseling strategy for each of the four major behavior patterns.
Willing.
Although having the patient express a willingness to be fit with amplification is a good sign, there are some potential issues that may emerge. Of course, these patients do not need intervention to be willing to act. However, it is important to confirm that they are acting for the right reasons and with the right expectations in mind.
The patient showing willing behavior needs to express an emotional investment in the fitting process, not just an intellectual one. It is possible that they are in the early stages of information gathering and may see a trial fitting as just an experiment. With the widespread availability of at-home trials and generous return privileges, saying "yes" to a fitting may not represent a full commitment to permanent use.
The COSI is a potentially useful tool to use with the patient who seems willing. However, care should be taken to make sure that the COSI is not filled out at a surface level. It is one thing to be able to identify several situations where communication breakdowns occur; however, it is another to express the frustrations that these situations engender. Time should be taken to discuss difficult situations to the point where the patient truly expresses the impact of the loss on themselves and their loved ones. In follow-up, especially for a patient who entered the trial fitting early in the acceptance/realization process, returning to COSI goals is a good way to remind the patient that the devices are addressing situations that have been particularly troubling.
One tool that can help to confirm that these patients are operating under realistic expectations is the Patient Expectation Guide. It is entirely possible that the patient may expect the devices to totally restore all hearing abilities. If the patient enters the process with those expectations and they are not met, then the patient may quickly decide that the devices are not providing benefit. Again, they have the tendency to operate in a purely logical fashion. With patients showing willing behavior, as with all patients, the key is to focus on the benefits that the devices do provide. Perhaps the solution will not be complete, but it will represent, for most patients, a significant improvement over going without amplification.
Normalizing.
A patient may show normalizing behavior for a variety of reasons. For example, perhaps the patient does not have the confidence that they can be successful, perhaps it seems like there is no reason to bother if they can continue to get by or perhaps they do not see the impact the hearing loss is actually having on their life. The key to success with a patient showing normalizing behavior is to help the patient see that amplification is something that can make their life better and that they deserve it.
The Box can be an excellent tool to dig deeper into how the patient really sees the impact of the hearing loss. The patient showing normalizing behavior will not likely be able to express much about the cost of not taking action. They tend to feel that they can continue to get by. The professional can help them better understand the sort of situations where communication can likely be easier. Enlisting the family members may be a good way to help the patient see that the hearing loss is truly having an impact on daily life. There may be some patients who truly do not recognize that reality or feel it is just the way things have to be. The hearing care professional can help to engender an earnest dialog between the patient and family.
They may also not have a clear idea of the specific benefits of taking action. They may know in general that hearing aids help with hearing loss, but they may not have identified the specific ways or situations in which this assistance will manifest itself. The COSI may be difficult for these people since they may not really see that they are having problems. However, if you can use the COSI to find a few key situations in the patient's life, then you may well be able to paint a picture as to how things could be better.
More to the point, a demonstration use of products can directly reveal to the patient what they have been missing. If at all possible, the patient should be given the opportunity to try devices out of the office, in their own environments for a few days. When the patient returns from the demo time, the family members can serve to re-enforce the positive experiences that amplification made during that time. In many cases, the biggest impact of the demonstration use of devices is when the patient takes them off and has to return them. Then it may be clear what difference they were making.
Although the patient may feel that they are getting by, it is entirely possible that the patient has been subtly withdrawing from difficult communication situations over the years. They may be getting by because they have limited the number of times that they are in challenging situations. They may not even be consciously aware of this change in behavior. To that end, it may be useful to have the patient not just focus on how things are now but to also consider how things used to be and how good they could potentially be. They may indeed be getting along fine, but they may also be limiting themselves. Probe to look for any significant changes in social behavior over the past several years and also have the patient describe, if at all possible, things that they would like to be able to do.
Don't underestimate the possibility that the patient may be lacking the confidence that they can be good at using amplification. If the patient has had trouble with either medical technology (e.g. blood glucose monitors) or consumer technology (e.g. DVD players), then they may feel apprehensive about approaching any new technology. Do not dismiss these concerns too quickly ("oh, you'll get used to these right away"). Include in the demo process the sort of practical handling of the devices that are part of daily use. The patient may have some unstated practical concerns (e.g., they may know someone who has struggled with feedback issues or someone who has lost a device), so you may want to probe for this possibility. Some patients may be price sensitive. They are not against the idea of using amplification; they just are concerned about the costs, so they minimize their difficulties. It will be important to probe for this possibility and make sure that the patient understands that there is excellent technology available at a range of price levels.
Finally, be aware that the patient may be minimizing the effect of the hearing loss because they truly do not want to be using amplification (for example, due to age-related stigma concerns), yet they do not want to state that fact outwardly. Remember, for most patients, hearing loss is not the first age-related change in body function. It may not be an easy thing for the patient to talk about, so they tend to dismiss any concerns about their hearing performance. If, through deeper questioning, it becomes clear that the patient may be having this sort of reaction, then you may want to consider strategies appropriate for the Conflicted category.
Wary.
Clearly, for the patient showing wary behavior, the hearing care professional needs to build trust. The patient must trust in the professional, trust in the product and trust that they are making the right decision. The lack of trust entering the process may be based on a variety of factors. Perhaps the patient has heard of the bad experiences of others - hearing aids that did not work well, broke down frequently, created feedback or simply did not provide benefit. Perhaps the patient is generally suspicious of any situation where a large purchase is involved. Perhaps they have made some large-scale purchase-decision mistakes in the past. There is no doubt that the dispensing of amplification takes on a "sales" feel in many settings. That may heighten wariness on the part of the patient and needs to be handled appropriately. It is also possible that the patient's wariness may not be related to the commercial element of the process at all but rather reflects a personality that just needs to have all the facts clear before a decision can be made.
Hearing device demos can work well for this group as long as the process is handled carefully. If the patient's wariness is based on a mistrust of someone trying to sell them something expensive, then suggesting a demo too soon can feel like a "hard sell". If this is the case, then time should be taken for the professional to make the case for the importance of amplification. On the other hand, if the wariness is based on a concern over all the practicalities of new devices or a concern that there will be a lot of practical problems, then getting to the demo early in the process can dispel a lot of these concerns. Obviously, the professional needs to quickly develop a sense of where the patient's concerns lie and respond accordingly.
The Patient Expectation Guide is a good tool to use for the patient whose wariness seems to be related to the sales nature of the process. If the professional can clearly explain the absolute expectations and also what the potential benefits can be, the patient may respond well to the frankness of the explanation. Again, trust in the professional is essential in the process. The Patient Expectation Guide is also helpful to ensure that the patient's expectations are appropriate. It is important for the patient who has concerns that this may not be the right thing to do that the initial experiences with amplification are in line with expectations. Expectations can be both positive and negative so the Patient Expectation Guide can serve to remind a patient of both the guarantees that are in place and also what the potential for success can be.
The Line is probably not a good tool to use with this population because it may have a "sales" feel to it. The fact that the patient came to have their hearing evaluated and is willing to discuss amplification is a sign that they are considering their options. Attempting to establish their level of motivation can potentially be misinterpreted by the patient as an assessment of their "sales potential".
The Box can be a useful tool with this population. By nature, these patients will be focused on the potential problems if they decide to pursue amplification. The quadrants that cover the negatives of not making a change and the potential positives of making a change can potentially balance out their concerns. Of course, there may be some specific patient concerns that are absolute: if they are not resolved, the patient will not move forward. However, often the concerns are not so black or white. Of course, there are costs to getting amplification: monetary, effort and lifestyle. If the patient is only seeing these, then of course the likelihood of getting devices is decreased. However, if these costs can be outweighed by the benefits of moving forward, then the fitting is more likely. The bottom line with patients from this category is that they have some real concerns about the process. Whatever their reason for concern, it is a good policy to make sure that these issues are uncovered, discussed and resolved right from the start. If the patient perceives that the professional is willing to be as forthcoming as possible, that can go a long way in building the trust that is essential.
One final point: It is entirely possible that the practical concerns that the patient expresses are simply a mask for some deeper, unspoken concerns. If the patient has some stigma-related concerns about the idea of becoming a hearing aid user, they may be expressed instead as practical objections. The hearing care professional must first and foremost deal with the issues that the patient expresses. However, care should be taken to be aware of the possibility that, below the surface, other types of concerns exist. As the practical objections are discussed and resolved, other issues may then emerge.
Conflicted.
Patients who show evidence of being conflicted over the idea of using amplification are the classic reluctant first time users. The key with patients in this group is to turn the discussion from what the hearing devices say about the user to what they can do for the user. However, changing the direction of the conversation can only take place once the patient has come to terms, at least on some level, with the notion of being a device user. There are several effective techniques available to help with acceptance.
This situation is perfect for use of The Line. This tool can help guide the discussion with the patient from a place where the conversation is centered on the fear of looking old to a place where the focus is on the potential life goals that are more likely attained with the use of amplification. In this context, of course, The Line is not just a diagnostic tool. Rather, it is a springboard to a discussion about the nature of the conflict that the patient is having. As mentioned earlier, not all patients with conflicted feelings will be as forthcoming as Patient 3 from the beginning of the paper: " I don't like it . . . the thought of getting really old."
However, that issue may lie right below the surface for a lot of patients and it may come out very quickly with just a little bit of probing. If there is a mismatch between the patient's stated level of willingness and the desires that they express, they may be looking for a professional with whom they can have this discussion.
The Box is also a valuable tool for these patients. The cost of change - the danger of appearing old, handicapped and incapable - can be balanced against the potential benefits of making a change. In the spirit of Motivational Interviewing (Miller & Rollnick, 2002), getting the patient to talk about the way their life could be can help to create forward movement. Importantly, the patient may not be willing to discuss the costs of not taking action. Again, the family can play an important role at this point in time. Perhaps the patient's stigma-related concerns may be such that they are not seeing the cost that their lack of action is having on those around them.
Shifting the focus to functional outcome is a key, but cannot be rushed. The patient does need the time to fully voice the nature of their concerns. It may not be necessary to get the patient to fully and absolutely accept the idea that they will become a hearing device user for life. Moving the discussion to the point where the patient is willing to consider trial use may be a useful intermediate stage. That is the point where a device demonstration can be useful. The appearance of the devices, both in the hand and on the ear, should be emphasized. An important positive sign is when the patient says “I could wear that.” Again, perhaps the commitment is not complete but it may be enough to move the process to the point of trial use. At that point, the discussion can then turn to the functional benefit being provided by the technology.
Are Some Patients Truly Not Ready?
There are some patients who truly should not be fit with amplification after the first interaction with the hearing care professional. As indicated above, some patients opt to gather information from professionals before deciding to act on healthcare issues. Some patients do not feel comfortable with making a major decision that will affect either lifestyle or finances without taking the time to examine all the options. Traditionally, a person who visits a hearing care professional but decides not to purchase amplification at the time might be viewed as a missed opportunity. That viewpoint is not consistent with what we understand about the way individuals interact with the healthcare system. For a voluntary decision, such as using amplification, many patients take upon themselves the responsibility to evaluate all options. The traditional notion that “the doctor will tell me what to do” is less and less apparent these days.
The hearing care professional should view a patient who does not decide to act during the first encounter not as a missed opportunity but rather as a future opportunity. The patient must act from a mindset of confidence and trust. The best thing that the hearing care professional can do is to validate the patient’s decision to continue to seek information before acting. Perhaps the patient feels the need to get a second opinion. Perhaps the patient feels that their hearing difficulties are not bad enough yet to require the purchase of amplification. The ultimate goal is to ensure that the patient does act at some point in time, preferably seeking out the services of a qualified professional. The hearing care professional can increase the likelihood that the patient will return to their office if they show respect for the patient’s decision to continue to consider options.
For the patient who is not sure that the hearing difficulties are severe enough yet to warrant intervention, one strategy that the hearing care professional can employ is to help the patient understand when will be the right time to act. As indicated above, patients often decide to act when they have experienced enough specific occurrences of communication breakdown that the frustration level reaches some threshold or tipping point. The hearing care professional can alert the patient to be on the watch for these instances of frustration (“moments of tribulation”, in the words of Engelund). Similarly, the patient may fall into a habit of avoiding certain situations because of hearing difficulties, even though this behavior may not be immediately apparent to the patient. The hearing care professional can alert the patient to the reality that avoidance behavior is a classic sign of hearing difficulties. If there are situations that the patient finds themselves not participating in that used to make up an important part of their life, then perhaps it is the hearing loss that is driving this change in socialization behavior. Finally, the family members can be enlisted to remind the patient of when the hearing loss is causing difficulties. Again, the patient may intellectually recognize the presence of hearing loss but may not feel enough motivation to take the next step. The family members can play an important role in reminding the patient when the hearing loss is creating stress or other difficulties.
Final Thoughts
The goal of everyone involved in the process is the same: to improve the communication abilities of the patient with hearing loss. The patient, the family members and the professional are all interested in overcoming the effects of hearing loss. The patient must be ready to accept the beneficial role of amplification. The family members need to understand the way amplification works and what they can do to help their loved one achieve the best possible performance. The professional wants to be able to bring effective service to the patient with documented hearing difficulties.
We know that accepting hearing devices is a lifelong decision by the patient, and that decision does not come easily. The professional needs to be careful not to minimize the concerns of the patient may have, whether they are based in fact or not. The decision to use hearing aids is a voluntary decision on the part of the patient and the professional needs to be sensitive to that reality.
The concept of Readiness Management is no guarantee for successful fittings. However, based on our review of an extensive literature on the mindset of the potential user, we believe there is a need to approach the counseling process in a different manner depending on the primary concerns expressed by the patient and family members. The patient has indicated some level of interest in seeking out a solution to the hearing difficulties. The concerns are justified and their questions legitimate. The better able the professional is at meeting the patient on their terms, the greater the likelihood that the entire process will turn out positively.
Importantly, fine tuning the counseling approach to match the classic behavior patterns that we have identified helps to confirm the important role of the professional and the process. With the popularity these days of nontraditional avenues to obtaining amplification, the role of the caring, qualified hearing care professional has been challenged. The recognition that the patient’s commitment to the process is typically not complete when they first start to consider the idea of using amplification underlines how important it is to have a professional to help guide the patient and the family through the process. Hearing technology in combination with qualified professional care can bring great benefit to patients suffering from hearing loss. Technology alone is not the answer. Guiding the patient through the process is essential to maximize the opportunity for the greatest level of communication function on the part of our patients.
Click Here to View APPENDIX A and APPENDIX B (PDF)
Acknowledgements
The authors would like to thank the following hearing care professionals who provided feedback on the Readiness Management concepts discussed in this paper: Nimet Adam, Linda Fudge, Sergio Guerreriro, Melody Hartman, Chiraporn Helton, Will Helton, Bill Heob, Alisa Kaufman, Valerie Kirney, Donna Mallory, Kurt Pfaff, Cheryl Runge, Leslie Soiles, Phyllis Stern-Weisman, Curt Thomas, Thea Wickey & Dawn Young.
References
Arlinger, S., Lyregaard, P.-E., Billermark, E., & Öberg, M. (2000). Fitting hearing aids to first-time users. Scandinavian Audiology, 29, 150-158.
Bisgaard, S. (2008). Coping with emergent hearing loss. Expectations and experiences of adult new hearing aid users. An anthropological study in Denmark. Ph.D. dissertation. Faculty of Linguistics and Cultural Studies, Johann Wolfgang Goethe Univerity, Frankfurt am Main.
Convery, E., Keidser, G., & Dillon, H. (2005). A Review and analysis. Does amplification experience have an effect on preferred gain over time. The Australian and New Zealand Journal of Audiology , 27(1), 18-32.
Dillon, H. (2001). Hearing Aids. New York: Thieme.
Dillon, H., James, A. & Ginis, J. (1997). Client Oriented Scale of Improvement (COSI) and its relationship to several other measures of benefit and satisfaction provided by hearing aids. Journal of the American Academy of Audiology, 8, 27-43.
Engelund, G. (2006). Time for hearing- recognizing process for the individual. Unpublished Ph.D. Thesis, Dept. of Nordic Studies and Linguistic Audiologopedics, University of Copenhagen, Copenhagen, Denmark.
Garstecki, D. & Erler, S. (1998). Hearing loss, control and demographic factors influencing hearing aid use in older adults. Journal of Speech, Language and Hearing Research, 41, 527-537.
Gatehouse, S. (1992). The time course and magnitude of perceptual acclimatization to frequency responses: Evidence from monaural fitting of hearing aids. Journal of the Acoustical Society of America, 92 (3), 1258-1268.
George, L. (2001). The social psychology of health. In R. Binstock & L. George (Eds.), Handbook of aging and the social sciences (pp. 217-237). New York: Academic Press.
Ida Institute. (2009). Motivation tools the line, box and circle. White paper. Naerum, Denmark. Available from author.
Keidser, G., O’Brien, A., Carter, L., McLelland, M., & Yeend, I. (2008). Variation in preferred gain with experience for hearing-aid users. International Journal of Audiology, 47(10), 621-635.
Knudsen, L., Öberg, M., Nielsen, C., Naylor, G. & Kramer, S. (2010). Factors influencing help seeking, hearing aid uptake, hearing aid use and satisfaction with hearing aids: A review of the literature Trends in Amplification , 14(3) 127–154.
Kochkin, S. (2000). MarkeTrak V: “Why my hearing aids are in the drawer”: The consumer’s perspective. Hearing Journal, 53, 34-42.
Kreisman, B., Mazevski, A., Schum, D. & Sockalingam, R. (2010). Improvements in speech understanding with wireless binaural broadband digital in adults with sensorineural hearing loss. Trends in Amplification, 14(1), 3-11.
Kuk, F. K., Potts, L., Valente, M., Lee, L., & Picirrillo, J. (2003). Evidence of acclimatization in persons with severe-to-profound hearing loss. Journal of the American Academy of Audiology, 14 (2),84-99.
Laugesen, S., Vestergaard, H., & Nielsen, C. (2005). Common conceptions about first-time versus experienced hearing aid users: Facts or Fiction? In A. Rasmussen, T. Poulsen, T. Andersen, & C. B. Larsen (Eds.), Hearing Aid Fitting (pp.261-287). 21st Danavox Symposium.
Leventhal, H., Rabin, C., Leventhal, E. & Burns, E. (2001). Health risk behaviors and aging. In J. Birren & K. Schaie (Eds.), Handbook of the psychology of aging (pp. 186-214). New York: Academic Press.
Lindley, G. (2008). Satisfying first-time users: A clinical study. Hearing Review. Retrieved from: https://www.hearingreview.com/issues/articles/2008-05_04.asp
Marriage, J., Moore, B. C., & Alcántara, J. I. (2004). Comparison of three procedures for initial fitting of compression hearing aids. III. Inexperienced versus experienced users. International Journal of Audiology (43)4, 198-210.
McConatha, J. & Huba, H. (1999). Primary, secondary, and emotional control across adulthood. Current Psychology, 18(2): 164-170.
Miller, W. & Rollnick, S. (2002). Motivational inter viewing: Preparing people for change (2nd ed). New York: The Guilford Press.
Oliver, S. & Palmere, N. (2011). Attracting first time users. Oticon White Paper. Available from Oticon.
Ramachandran, V., Stach, B., & Becker, E. (2011). Reducing hearing aid cost does not influence device acquisition for milder hearing loss, but eliminating it does. Hearing Journal, 65(5), 10-18.
Reber, M. B., & Kompis, M. (2005). Acclimatization in first-time hearing aid users using three different fitting protocols. Auris Nasus Larynx, 32, 345-351.
Saunders, G. H., & Jutai, J. (2004). Hearing specific and generic measures of the psychosocial impact of hearing aids. Journal of the American Academy of Audiology, 15 (3), 238-248.
Schum, D. (2009, April 13). Managing patient expectations. AudiologyOnline, Article 2225. Retrieved January 20, 2012 from the Articles Archive on www.audiologyonline.com
Schum, D. (1999). Perceived hearing aid benefit in relation to perceived needs. Journal of the American Academy of Audiology, 10, 40-45.
Schum, D. & Pogash, R. (2011, March). New insights into first-time users. Paper presented at the Annual meeting of the American Auditory Society, Scottsdale, AZ.
Skaff, M. (2007). Sense of control & health. In C. Aldwin, C. Park & A. Spiro (Eds.), Handbook of health psychology and aging (pp. 186-209). New York: Guilford Press.
Smart, J., Kreisman, B., Robinson, C., Marczewski, C. & Butler, C. (2011, April). Evaluating hearing aid benefit during the first four weeks. Paper presented at the Annual Convention of the American Academy of Audiology, Chicago, IL.
Smeds, K. (2004). Is normal or less than normal overall loudness preferred by first-time hearing aid users? Ear & Hearing, 25, 159-172.
Whitbourne, S. (2002). The aging individual. New York: Springer Publishing.
Wong, L., Hickson, L., & McPherson, B. (2004). Hearing aid expectations among Chinese first-time users: Relationships to post-fitting satisfaction. The Australian and New Zealand Journal of Audiology , 26, 53-69.

