Quality can be difficult to define, but to paraphrase a U.S. Supreme Court justice's ruling on a far more tawdry subject;most people know it when they see it. This rather loose definition of quality certainly applies to the typical American audiology practice, where very few aspects of the patient's interaction with the clinic are monitored. This inability or unwillingness on the part of the practice manager to measure various aspects of each patient's interaction within the clinic presents a significant problem for the profession of audiology, and the hearing aid dispensing industry as a whole. As this article will suggest, however, taking the time to measure some of the essential dimensions of the patient's interaction with your clinic is the key to improving patient satisfaction and further business growth.
According to a recent survey by Unitron of 300 practice managers in the United States (Unitron, 2008), the typical hearing aid dispensing practice can be described in the following way:
- Has been in operation for more than 15 years (median average)
- 95% are full-time businesses.
- Possess an average of 500-1,000 patients
- Is primarily a one-audiologist/hearing instrument specialist shop with one supportive administrative staff
- Uses a salary plus commission model for licensed hearing care professionals on staff (50% salary, 39% combination salary/commission, 10% full commission)
- Sees 33 patients and dispenses an average of 17 hearing aids per month
In practical terms, the two major drivers of patient satisfaction are service quality and product quality. Both dimensions must be measured, directly or indirectly, if overall patient satisfaction is to be markedly improved.
Regardless of the size and location of a hearing aid dispensing practice, all professionals recognize the importance of patient satisfaction. We know, through both clinical intuition and survey data analysis, that highly satisfied patients are an economic engine for the typical practice. Highly satisfied patients are far more likely to be repeat purchasers, and to refer other patients to the practice, than merely satisfied patients. Talking about the importance of patient satisfaction is easy;taking the time to implement procedures that actually improve patient satisfaction is difficult. Clearly, there is a disconnect between knowing how to create a highly satisfied patient and consistently doing it.
Peter Drucker, the highly influential business management pioneer, once said, "When you measure something you begin the process of improving it." When it comes to taking care of patients or running a practice, nothing could be more true. Taking the time to measure various aspects of your practice has a profound and lasting effect on its productivity. Successful business managers are well versed in the concept of measuring important things, as they routinely quantify several key financial indicators.
The majority of, but certainly not all, audiology practice managers are familiar with the fundamental metrics of their business. Figure 1 shows the percentage of Unitron survey respondents that routinely track several key financial variables. The majority of respondents said they track the following variables on a monthly basis: gross revenue (80%), cost of goods (78%), return rate (62%), average selling price (61%), tested, not sold (53%), and close rate (52%). Although there is certainly room for improvement on what financial variables are measured, the savvy manager understands the importance of tracking these numbers in order to gauge the progress of the business, and the need to quickly try to fix any decline in performance over the course of the year.
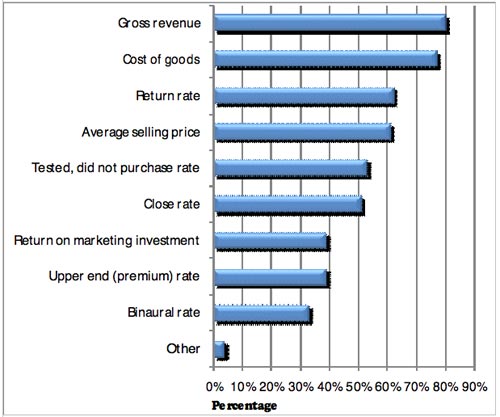
Figure 1. The percentage of survey respondents tracking several key financial variables on a monthly basis (Unitron, 2008).
While managing financial capital is a necessary activity, it is not sufficient for creating high levels of patient satisfaction. Additionally, a keen examination of consumer buying trends clearly indicates that managers need to reach beyond traditional financial metrics and begin to systematically assess the quality of patients' interactions with their practices. A primary focus of this article is to define several dimensions of quality, as well as to offer several pragmatic approaches for measuring them in a busy practice. The astute practice manager must look beyond simply measuring key financial indicators by combining several direct and indirect measures of the patient's interaction with your practice. In this way the manager can continue to raise the standards on how care is delivered to patients and, consequently, the practice will become more profitable.
Part of the Quality Equation: Outcome Measures
Audiologists, who are generally extraordinary caregivers, have at their disposal a plethora of well designed clinical measures of hearing aid outcome. Audiologists who only rely on one or two routine measures of hearing aid outcome may be overlooking several critical components of both service and product quality. Unfortunately, the majority of hearing care professionals do not routinely measure hearing aid outcome. According to Kirkwood (2005) less than 35% of audiologists and hearing instrument specialists routinely measure outcome.
Over the past decade there have been several excellent studies examining the various dimensions of hearing aid outcome. In practical terms, all of these studies can be condensed into two primary schools of thought.
Dr. Larry Humes and colleagues at Indiana University have published over twenty articles on various dimensions of hearing aid outcome (see Humes, 2004 for a review of findings). According to Humes (2004), there are three separate and unique dimensions of hearing aid outcome that account for a significant amount of their overall variability. These three dimensions are hearing aid usage, unaided vs. aided speech recognition performance, and benefit/satisfaction. Both laboratory and self-report measures of outcome can be used to measure these three dimensions.
Another bastion of outcome measures research is the University of Memphis, where Dr. Robyn Cox and colleagues have published several articles related to all aspects of hearing aid outcome. In essence, Cox's work in the area of self-reported outcome, which serves as the gold standard in an evidence-based practice paradigm, can be boiled down to using self-report questionnaires that have both device and wearer components, so that issues related to variables including personality, expectations, and attitude can be accounted for during the measurement process.
The collective work of Cox and Humes suggests that hearing aid outcome is most effectively measured by using a combination of laboratory and self-report tools that systematically capture the separate dimensions of outcome. For the purposes of measuring benefit and satisfaction with hearing aids, this may serve as a good starting point. However, we will take a much broader look at other dimensions of outcome, as they relate to the patient's entire journey through your practice.
Taking a Much Broader View of Outcome
The decision to take a much broader view of hearing outcome is based on research done outside the profession of audiology. Today all customers, due mainly to the Internet and mass marketing campaigns, have an abundance of choices. The availability of hearing instruments through multiple buying channels, most of which offer several price points, gives customers unprecedented power. Given their power, consumers can change the dynamics of the market by taking their business elsewhere, or by simply choosing not to do business with anyone who leaves a lasting negative impression. For the practice manager focusing on quality, in addition to the number of units sold and other traditional financial metrics, can have a profound impact on the long-term success of the business. According to Fornell (2008), in a competitive market the business that has the reputation as the leader in quality will soon own the highest market share and be able to command the highest average selling price. From a business standpoint, it is in the best interest of every audiologist and practice manager to have an obsession with quality and how to measure it.
Unlike key financial indicators, which can be quantitatively measured, quality measures are more challenging to accurately measure. There are several reasons for this. First, patients have their own interpretation of quality. Due to individual variations, one or two simple measures are not likely to capture it. Second, quality is difficult to quantify. Ten point Lickert scales, for example, can be used to measure the quality of the patient's experience in the clinic. However, Lickert scales and other similar tools have some degree of subjectivity and, also, do not fully capture all the dimensions of the patient's experience within the clinic. Finally, because quality is a somewhat vague and abstract concept, we need to look at multiple dimensions in order to more precisely measure it.
There are two different ways to measure quality within the audiology practice. Directly measuring quality is conducted by employing either subjective or objective metrics. The other approach is to use an indirect, or proxy, measure. This would include any type of checklist or scale that represents important behaviors or procedures that must be conducted by the hearing professional or support staff in order to achieve more favorable results. An example of a proxy quality measure would be a hearing aid evaluation protocol checklist. Once the hearing professional has been given guidance on the execution of a clinical protocol, the manager can refer to the checklist in order to verify that certain procedures were conducted with each patient. Figure 2 outlines direct and proxy measurements. A combination of direct and proxy measures are used in order to get a comprehensive picture of quality.
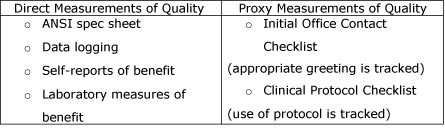
Figure 2. Various direct and proxy (indirect) measures of quality in a hearing aid dispensing practice.
Seven Dimensions of Quality and How to Measure Them
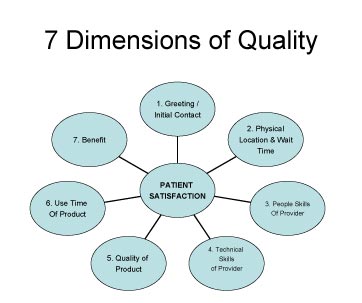
The purpose of this article is to give the busy clinician some helpful and easy-to-use tools that will measure quality in a holistic manner. Using a pragmatic approach, seven dimensions of quality will be reviewed here. These seven dimensions represent the various phases of the patient's journey from initial contact with the office until initial use of hearing aids. By taking the time to measure these quality dimensions, the hearing professional can manage the entire process and begin to ensure that each patient is highly satisfied with all aspects of his or her experience.
Click Here to View Larger Version of Figure 3
Figure 3. The seven dimensions of quality have a direct impact on patient satisfaction.
- Wait Time and Initial Greeting of the Patient in the Clinic
Woody Allen once said that 80% of success is simply showing up. In any customer service based business this certainly holds true. Little things, like the receptionist walking over to the patient and shaking her hand when she arrives in your clinic, can make a big difference to the overall success of the practice. Taking the time to fine tune the details of your initial greeting of patients is likely to improve business results. A warm handshake and smile go a long way toward putting patients at ease. This results in the patient being more willing to do business with your clinic. Managers can train their front office staff to warmly greet all patients when they arrive. Since communication experts agree that standing up, squarely facing the patient, smiling and offering a handshake are components of an ideal greeting, the ability of the front office staff to perform these behaviors can be tracked by using a form like the one shown in Figure 4.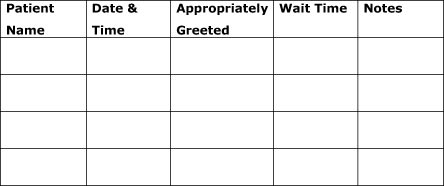
Figure 4. Sample tracking form used to measure the initial greeting and patient's first contact with the practice. - Appearance of Physical Location
The reception area or waiting room is one of the most easily overlooked aspects of a practice, but the most important first impression for patients. It may seem rather obvious that when patients enter a practice location they expect the facility to reflect their perception of a professional business. However, given the relatively high number of disheveled offices around the country, many managers and owners do not routinely inspect the physical appearance of their practices.
Beyond the reception area, the entire physical location of the practice needs to be routinely inspected. A simple approach to measuring and maintaining the quality of any physical location is to utilize a checklist that the office manager or front office professional marks daily with meticulous attention to detail. The physical location checklist is completed each morning by the office manager, and a written copy is shared with owner or managing director. All areas in need of upgrades or repair are recorded at the bottom of the form.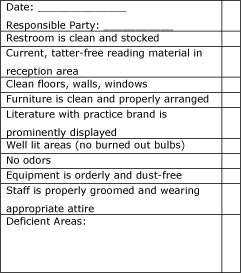
Figure 5. Physical location checklist. - Interpersonal Communication Skills of the Hearing Care Professional
The effectiveness of audiologists is largely determined by their ability to form strong relationships with patients. Any investment managers can make toward improving the relationship building skills of their employees is likely to pay off in improved service delivery. Good listening skills, the ability to ask open-ended questions, and clear and concise explanations of test results are a few of the "people skills" needed to build effective relationships with patients. This will make an important contribution to patient satisfaction.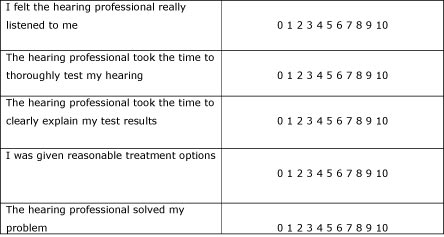
Figure 6. Five important components of relationship-building skills that can be measured on a comment card. 0 is highly dissatisfied and 10 is highly satisfied.
Interpersonal or relationship-building skills can be directly measured by patients. Using a comment card with five or six important components of interpersonal skills, like the one shown in figure 6, patients can directly measure the effectiveness of this dimension of quality. Once a representative data sample has been collected (15 to 20 responses per month for the typical practice), you can begin the process of improving behaviors that have the largest impact on patient satisfaction. - Technical Skills of the Service Provider
The ability of the hearing professional to conduct a comprehensive hearing evaluation, as well as program, fit & troubleshoot hearing devices can be indirectly measured by assessing the professional's adherence to a clinical protocol. There is no shortage of clinical hearing aid selections and fitting protocols. The most current clinical hearing aid selection and fitting protocol sanctioned by the American Academy of Audiology, incorporates evidence-based practice standards.
Unlike interpersonal skills, which patients can directly measure, the technical ability of hearing professionals needs to be gauged indirectly by tracking their adherence to a clinical protocol. In Figure 5 below, the essential standards for a pre-fitting hearing aid consultation appointment are outlined. Managers can track the execution of a protocol by requiring hearing professionals place a completed checklist into each patient chart notes at the end of the consultation.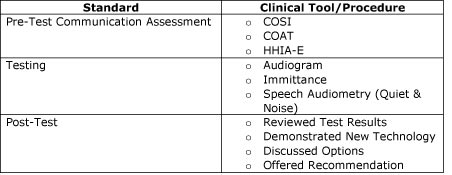
Figure 7. An example of a clinical protocol checklist. Once the hearing professional has been given guidance on how to conduct each procedure, she can begin to document that the protocol was followed by using the checklist. - Product Quality
2-cc coupler measures within the hearing aid test box are the standard method for ensuring that hearing aids are performing at a specific standard set by the manufacturer. They can also be used by the hearing professional before the fitting to ensure that the hearing aid is functioning properly. Prior to the fitting the hearing professional must take the hearing aids from the packaging material, perform a listening check on them and, finally, conduct a routine electroacoustic analysis of the devices, using the correct 2 cc coupler.
A 2 cc coupler analysis in your test box is compared to the specification sheet enclosed in the new order. If any of the ANSI tests shown on the spec sheet are not within +/- 2 dB of those recorded on the manufacturer's spec sheet, or if the listening check indicates a possible problem, the device must be repaired or exchanged immediately. Once the 2 cc coupler measure has been conducted in your office and the hearing aids are working within the manufacturer's specifications, this information is documented in the patient's chart.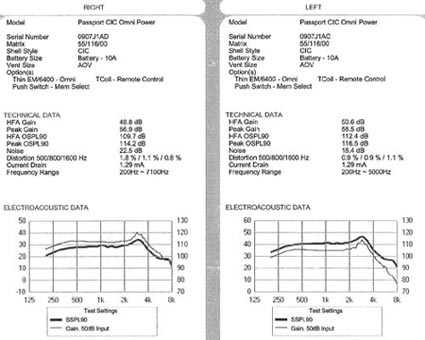
Click Here to View Larger Version of Figure 8
Figure 8. A sample specification sheet from the manufacturer. The same tests are performed in the clinic prior to the fitting to verify acceptable performance in the 2-cc coupler.
In addition to 2-cc coupler measures, the hearing professional can rely on a hearing aid fitting checklist as a proxy measure of product quality. After the fitting has been completed, the clinician completes the checklist, noting anything usual or problematic, before placing the checklist into the patient's chart. Figure 8 is an example of a hearing aid fitting checklist.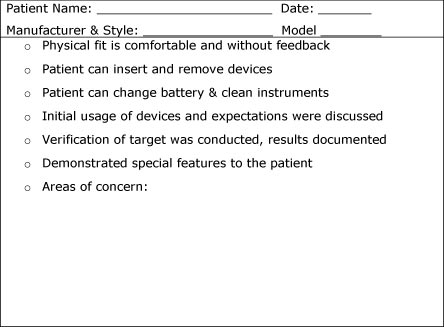
Figure 9. An example of a hearing aid checklist used to measure the quality of the initial fitting.
The final three dimensions of quality can be systematically evaluated using traditional measures of hearing aid outcome. Two separate studies conducted by Humes (2003, 2004) using an assortment of more than 20 outcome measures identified three separate and distinct aspects of hearing aid outcome: 1) aided and unaided speech recognition performance;2) self-reported hearing aid usage;and 3) subjective benefit and satisfaction. Given these findings, both subjective and objective measures of outcome should be used to assess quality in clinical practice. - Use Time of the Devices
There is a relationship between patient satisfaction and use time of hearing aids, as full time hearing aids users are more likely to report higher overall satisfaction scores compared to part time or non-users. In addition, lower rates of usage are reported for patients with negative attitude towards amplification (Wilson & Stephens, 2002), patients in denial (Brooks & Hallam, 1998) and those that consider hearing aid use to be stigmatizing (van den Brink, R.H., Wit, H.P., Kempen, G.I., & van Heuvelen, M.J., 1996).
Hearing aid use rate can be measured either subjectively or objectively. Subjective measures of use time would be considered to be diaries or questionnaires that the patient completes. Research conducted by Taubman, Palmer, Durrant, and Pratt (1999), however, suggests that subjective reports of usage are unreliable. Fortunately, objective measures of usage can be readily obtained using data logging, which is found in many modern hearing aids. One of the advantages of data logging is that it objectively tracks the total number of hours of hearing aid use. Part time and non-users can be managed differently than full time users. For example, a patient with a low use rate, which has been objectively verified with data logging, might have a problem with annoyance from noise as measured on the acceptable noise level (ANL) test. The low use time combined with the high unaided ANL score would be an indication that the patient needs a more aggressive noise reduction strategy. - Laboratory & Self Reports of Hearing Aid Benefit
Benefit is simply the difference between the unaided and aided condition. Hearing aid benefit can be measured in a number of different ways, including laboratory measures and self-reports or questionnaires. Considering the findings of Cox and Alexander (2007) and Humes (2004), a logical approach to measuring benefit would be to use some combination of laboratory and self-reports.
Laboratory measures of benefit complement probe microphone verification measures, as they can be used to objectively demonstrate to the patient that certain features within the hearing aid are functioning properly. For example, the QuickSIN can be presented at a low intensity level (45 dB HL) in the unaided and aided condition. The difference between these two scores would be the aided benefit on a speech recognition task. When the QuickSIN is conducted at a low intensity level, it provides the patient with meaningful information on how improved audibility usually translates into improved speech intelligibility in noise. To conduct this test, perform the following three steps.Step 1: The patient is placed 1 meter from a single speaker at 0 degrees azimuth. Using the QuickSIN, unaided scores are obtained and recorded.
Aided Loudness Discomfort Levels (LDLs) are a useful tool for identifying discomfort associated with high hearing aid outputs. This is especially true during the initial adjustment period;after the patient has been subjected to common loud environmental sounds while using their new devices. Additionally, binaural summation and channel summation are thought to affect measures of loudness discomfort with hearing aids. Therefore, aided LDLs may need to be evaluated in a systematic nature.
Step 2: The aided condition sentences are presented at a typical level of soft conversation (i.e., 50 dBHL) as the noise level is increasing using an adaptive procedure of the QuickSIN.
Step 3: Relate the results of this test to real world listening conditions that the patient experiences. Conducting speech in noise tests at low intensity levels is an effective way to demonstrate to patients the effect audibility has on intelligibility in noise.
In order to complete aided loudness discomfort level testing, the audiologist needs a CD player and a speaker (stereo system or boom box), an inexpensive sound level meter (SLM), and a CD with recordings of common noises. The procedure is conducted in the following manner:Step 1: Before conducting the test, the audiologist needs to calibrate the CD through the stereo system. This is done by placing the SLM approximately 1 m from the speaker and setting the volume of the stereo system so that the reading on the SLM reaches 85 dBA. The volume level on the boom box needs to be marked for future reference
Step 2: Place the patient 1 m from the speaker while wearing the hearing aids. Using the IHAFF loudness chart, ask the patient to rate the loudness of various passages that have been calibrated to reach 85dBA on the SLM. (The patient can be instructed using the IHAFF LDL guidelines).
Step 3: Patient listens to the passage and rates the loudness level on the IHAFF scale. Patients should rate the passage to be a #5 or #6 on the chart. If the patient rates them as #7, the output needs to be adjusted on the hearing aids.
Figure 10. A summary of helpful hearing aid outcome measures used to evaluate hearing aid benefit and satisfaction.
Self-reports or questionnaires compliment laboratory measures of benefit because they ask the patient to rate their success with amplification in everyday listening, using some type of a scale. There are dozens of self-reports that have been created and validated. Self-reports subjectively measure real world benefit and are an integral part of an evidence-based practice paradigm. Below, three of the most useful self-reports are reviewed. The author recommends that hearing professionals choose two of the three listed here and use them routinely to measure real world hearing aid benefit and satisfaction.
The Client Orient Scale of Improvement (COSI) was developed by the National Acoustic Laboratories (Dillon, James & Ginis, 1997). The COSI is an open-ended scale in which the patient targets up to five listening situations (from a list of 16) for improvement with amplification. The COSI was normed on 1770 adults with hearing loss in Australia. The goal of the COSI is for the patient to focus on the five specific listening situations and to report the degree of benefit obtained in those situations compared to that expected for the population. Many hearing aid manufacturers now include the COSI in their fitting software. The COSI can be downloaded for free from the NAL website.
Abbreviated Profile of Hearing Aid Benefit (APHAB)
In an attempt to develop a more clinic friendly measure of outcome, the APHAB was developed (Cox & Alexander, 1995). Like the Profile of Hearing Aid Benefit (PHAB), the goal of the APHAB is to quantify the disability caused by hearing loss, and the reduction of that disability achieved with hearing aids. The APHAB uses 24 items covering 4 subscales: ease of communication, reverberation, background noise, and aversiveness to sounds. The APHAB was normed on 128 elderly adults with mild to moderate hearing loss. The APHAB can be downloaded from the University of Memphis Hearing Aid Research Lab (HARL) website.
International Outcome Inventory for Hearing Aids (IOI-HA)
Consisting of seven questions on a five point rating scale, the goal of the IOI-HA is to assess benefit, satisfaction and quality of life changes associated with hearing aid use. The IOI-HA has been normed on 154 adults (Cox, Alexander, & Beyer, 2003). The IOI-HA was designed to be used with other self-report tools, like the APHAB. It is available in several languages, and can be downloaded from the University of Memphis HARL website.
Which Self-Report Outcome Measure Should Be Used?
Due to the abundance of self-reports available to the clinician, it is difficult to know which ones work the best. When making this decision, it is important to examine exactly what dimension of real world outcome you are trying to capture in the most time-efficient manner. Cox and Alexander (2007) in a large scale study with several variables examined the relationship between self-reports of outcome and personality. Analyses of the collection of outcome measures produced a set of three components that were interpreted as a Device component, a Success component, and an Acceptance component. Results suggest that personality is more closely linked to self-reports of hearing aid outcome than conventional laboratory measures, like the audiogram. How personality effects outcome needs to be taken into consideration when selecting a self-report questionnaire.
Summary
In today's modern audiology practice it seems there are two distinct approaches to management. One approach is composed of managers with a strong audiology orientation that have a tendency to focus on the technical aspects of hearing aids. When they actually take the time to quantify the results of their fitting, those with a product orientation typically focus on measures of hearing aid outcomes, if they measure anything at all.
On the other hand, there is another type of audiology practice manager who focuses almost exclusively on tracking key financial indicators, with little regard for hearing aid outcome measures or the use of a clinical fitting protocol. According to survey data, this group of business managers may focus on just a few metrics that quantify business operations and routinely track them. Beyond cost of goods, average selling price, and gross revenue, very few other metrics of a practice's economic are routinely tracked even by this business- oriented group.
Given the fact that patient satisfaction is directly related to both service and product quality, business managers need to look beyond exclusive use of traditional financial metrics or traditional measures of hearing aid outcome to gauge the success of their practice. Squarely focusing on the patient's interaction with the practice and taking the time to measure various aspects of this interaction allows the prudent practice manager to see the benefits of blending a commercial and clinical approach to improving patient satisfaction, business productivity, and efficiency. Measuring each of the seven dimensions of quality, using a combination of direct and proxy measures, enables the professional to identify performance gaps and begin the process of improving them. Managing today's modern audiology practice requires judicious application of quality metrics that compliment the traditional productivity measures. Audiologists, hearing instrument dispensers, and practice managers alike must start measuring quality in order to improve it.
References
Brooks, D., & Hallam, R. (1998). Attitudes to hearing difficulty and hearing aids and the outcome of audiological rehabilitation. British Journal of Audiology, 32(4), 217-226.
Cox, R. & Alexnder, G. (1995). The Abbreviated Profile of Hearing Aid Benefit (APHAB). Ear and Hearing, 16, 176-186.
Cox, R., Alexander, G., & Beyer, C. (2003). Norms for the international inventory for hearing aids. International Journal Audiology, 14(8), 403-413.
Cox, R. & Alexander, G. (2007). Personality, hearing problems, and amplification characteristics: contributions to self-report hearing aid outcomes. Ear and Hearing, 28(2), 141-162.
Dillon, H., James, A., & Ginis, J. (1997). The Client Oriented Scale of Improvement (COSI) and its relationship to several other measures of benefit and satisfaction provided by hearing aids. Journal of the American Academy of Audiology, 8(2), 27-43.
Fornell, C. (2007). The Satisfied Customer: Winners and Losers in the Battle for Buyer Preference. New York: Palgrave Macmillan.
Humes, L. (2004). As outcome measures proliferate, how do you choose which ones to use? The Hearing Journal, 57(4), 10-17.
Humes, L.E. (2003). Modeling and predicting hearing aid outcome. Trends in Amplification, 7(2), 41-75.
Taubman, l., Palmer, C., Durrant, J., & Pratt, S. (1999). Accuracy of hearing aid use time as reported by experienced hearing aid users. Ear and Hearing, 20(4), 299-305.
Unitron (2008). [Survey of hearing care practice managers]. Unpublished survey.
Van den Brink, R.H., Wit, H.P., Kempen, G.I., & van Heuvelen, M.J. (1996). Attitude and help-seeking for hearing impairment. British Journal of Audiology, 30(5), 313-324.
Wilson, C., & Stephens, D. (2003). Reasons for referral and attitudes toward hearing aids: do they affect outcome? Clinical Otolaryngology, 28(2), 81-84.