Traditionally, optimizing hearing aid sound quality has been accomplished through a process of patient interview and device adjustment. While ultimately effective, this process is inefficient, sometimes requiring multiple visits to arrive at subjectively acceptable settings. In some cases, the patient elects to return the hearing aid for credit before optimal sound quality is achieved. This paper introduces SoundPoint, a new patient-assisted fine tuning process that complements the traditional fitting process by placing control of sound quality in the hands of the patient. The SoundPoint system offers an alternative to the method of 'interview and adjust' by presenting the patient with ability to navigate through a perceptual world of possible hearing aid adjustments. Via use of a touchpad (as shown in Figure 1) or through the intuitive movement of a mouse, adjustments are made to the patient's hearing aids in a smooth and seamless manner, allowing patients to find their preferred subjective sound quality without the need to articulate the acoustic complexity of their own auditory perceptions.

Figure 1. A patient fine tunes hearing aids to preferred listening settings using the SoundPoint iPad remote interface.
Prescriptive methods based on audiometric data may prescribe gains that differ significantly from a patient's preferred settings (Liejon, Eriksson-Mangold & Bech-Karlsen, 1984). These differences are likely due to the fact that the algorithms cannot incorporate individual variability in loudness growth, most comfortable listening level (MCL) or upper level of comfort (UCL) due to the process of averaging test data from a large sample of listeners to arrive at a prescriptive target (Kiessling, 2001). For example, Dillon and colleagues (2006) found that an individual's comfortable listening level may deviate from NAL-NL1 prescribed targets by as much as 18 dB. The general healthcare literature suggests that outcomes are improved when patients are involved in the decision making process (Roberts, 1999; Frosch & Kaplan, 1991). Similarly, the hearing aid literature reminds us that success with a hearing aid fitting will improve when the fitting is customized according to feedback from the patient regarding his or her individual preference (Dillon et al., 2006). These findings affirm the potential benefit of customizing a hearing aid fitting to achieve acceptable sound quality after appropriate audibility for speech level inputs is verified. In essence, optimization of sound quality according to the preferences of the individual marks the difference between fitting the hearing loss with hearing aids, versus fitting the individual with hearing aids.
SoundPoint - Origins
SoundPoint is a computer-based signal processing tool developed by researchers at Starkey Laboratories. Designed to provide a fast, simple means of adjusting complex signal processing algorithms, the system works as a listener-assisted hearing aid fine-tuning interface. It allows the user to tailor almost infinite combinations of up to 64 parameters in real-time, ultimately resulting in the selection of preferred hearing aid settings.
The adjustments made with SoundPoint go far beyond a simple gain control, thus the interface must be more than a simple graphic equalizer. For this reason, early work on the development of SoundPoint focused on the organization of the adjustments available to the patient in a pattern that allowed smooth and intuitive changes to sound quality. It was quickly realized that in order for listeners to be able to use the interface successfully; it was essential that the control space have perceptual consistency, a requirement that consists of two major components. First, movement in a particular direction should result in a consistent change in a particular sound quality. Second, a small range of movement in the control space should result in a small change to the sound of the hearing aids, while a large movement should result in a change of greater perceptual magnitude.
The result of this work is that as patients navigate through the control space, various adjustments are blended and applied to the hearing aids. With an appropriate organization of the interface, listeners are able to consistently navigate to perceptually similar preferred settings from trial to trial, suggesting that desirable sound quality can be reliably achieved within the SoundPoint environment. Paired comparison testing was conductedd to determine if the organization of the layout had an effect on listeners' preferred hearing aid settings. In fact, listeners preferred hearing aid settings achieved with an optimized organizational layout over randomly sorted layouts and self generated layouts. These early phases of development provided the proof of concept for SoundPoint as a listener-assisted fitting tool as well as important implementation information regarding the interaction between the organizational layout of the control space and the navigation task completed by the listeners. For an in-depth review of the SoundPoint development process, please see Abrams, Edwards, Valentine and Fitz (2011).
The result of these research efforts is that the relationship of the SoundPoint system to the hearing aids appears deceptively simple and highly intuitive. The listener manipulates fitting parameters as the mouse pointer is moved around the screen. The relationship between the position of the pointer and the various changes to fitting parameters is recalculated continuously in real time, resulting in a smooth blending of, and transition across, various sound qualities. The listener perceives only a smooth change in sound qualities such as loudness, brightness, richness, fullness and speech intelligibility as the SoundPoint environment is explored.
Validation of SoundPoint as a Solution for Preferred Sound Quality
SoundPoint has been validated through laboratory and field trial evaluations. These studies, described later in this article (see Experimental Validation), were designed to provide data on 1) objective benefit, 2) subjective benefit and sound quality, and 3) preference among fittings conducted with the SoundPoint system, traditional fittings fine-tuned by the professional, or audiogram-based prescriptive methods.
Three important goals were set forward in the development of the SoundPoint tool. The first was that clinically acceptable audibility would be preserved while also achieving the second goal, providing a large range of perceptual differences within the SoundPoint fitting environment. Third, the system must provide an intuitive and satisfying experience, in which the goal and process would be immediately apparent and achievable for all users. The first goal was achieved by constraining the range and type of adjustability within the system. The second is one of the most important concepts of the SoundPoint system. Rather than functioning as the hearing aid equivalent of a graphic equalizer, the system represents audible changes along a perceptual continuum. That is, since it is possible to arrive at the same perceptual experience via several different combinations of gain and compression parameters, settings that produce similar sound qualities are found close together in a particular area of the SoundPoint environment, while those that produce very different perceptual experiences are located relatively far apart. These qualities provide an intuitive user experience, where changes to sound quality occur in a logical and transparent manner. This third goal was achieved via careful design, refinement and clinical validation of the SoundPoint system.
Clinical Use of SoundPoint
The SoundPoint fitting process consists of 4 steps: Calibration, Derivation of Presets, Instruction and Navigation. These steps are described below.
Calibration:
1. When the clinician launches the SoundPoint fitting process, the hearing aids are connected automatically via wireless or wired link, and a calibration screen is presented. The screen instructs the clinician to position the patient facing the right loudspeaker, and to initiate the calibration process. A speech-shaped calibration stimulus is presented from the right channel loudspeaker in the fitting room. The level of the stimulus is measured at the patient's ears through the microphones of the hearing aids, and is adjusted by the clinician so that it is presented at 60dBA (Figure 2).
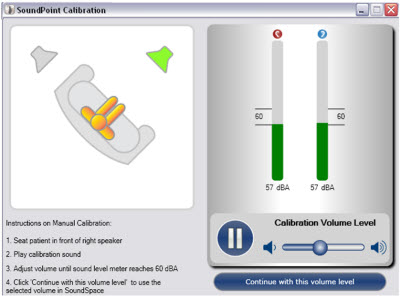
Figure 2. Calibration process within SoundPoint fitting software.
2. System Preparation: The SoundPoint fine tuning environment is launched, and an appropriate range of adjustability is calculated based on the patient's audiogram. SoundPoint is available for patient use within fifteen seconds (Figure 3).
Figure 3. SoundPoint animated initialization screen.
3. Instruction: When the SoundPoint system has completed the startup screen, the patient is presented with simple directions for the use of the system (Figure 4).
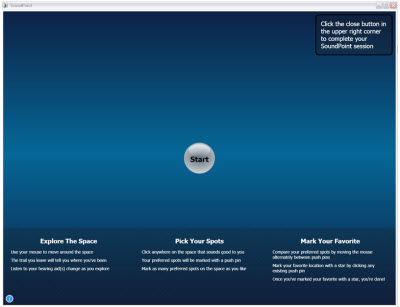
Figure 4. SoundPoint Instructional screen. Patients are invited to a) explore the space, b) mark promising areas, c) compare those areas, and d) mark their favorite.
4. Navigation: While listening to a speech-in-noise recording constructed from the Connected Speech Test (Cox, Alexander & Gilmore, 1987), the patient explores the SoundPoint screen by moving a pointer with a mouse or by dragging a finger across the screen when using an iPad interface. As the pointer is moved, the patient experiences changes in terms of overall loudness, frequency shaping and compression. The patient can leave markers (pushpins) on the screen at the locations of appealing settings, and quickly and easily compare the various qualities of sound achieved by instantly switching between the favorites (Figure 5). When a preferred fitting is identified (gold star), the settings are instantly stored in the hearing aid and in the patient database by Inspire OS fitting software.
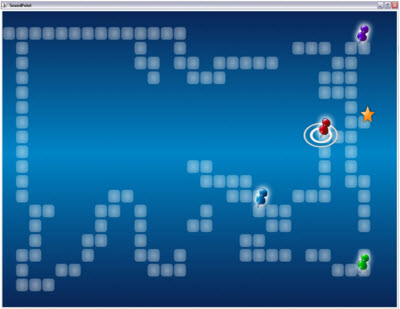
Figure 5. SoundPoint navigation in process. Settings of interest are indicated by colored pushpins. When directly comparing favorites, the current favorite is highlighted by animated rings around the pushpin. The selected favorite becomes a gold star.
The SoundPoint system can be used with any of the prescriptive fitting algorithms supported by Inspire™, or the patient can fine-tune the settings that are already in the hearing aids to optimize sound quality. The system is currently available in Starkey S Series iQ and Wi Series hearing instruments.
SoundPoint offers benefits beyond time savings and patient satisfaction. The system can help the clinician to substantiate vague complaints by revealing patient preferences. The clinician can monitor the parameters that are being changed in real-time, identify patient preferences and help in alleviating patient concerns.
Experimental Validation
Twenty-nine hearing impaired adults participated in a clinical trial. Detailed results of this trial are discussed by Abrams and colleagues (2011). Participants were fit via the SoundPoint approach during one visit and by an experienced audiologist during another. Fitting condition order was randomized and counterbalanced, and followed by a two-week field trial with each fitting. Following each fitting, probe microphone measurements were conducted to assess audibility of speech level inputs, and a Speech Intelligibility Index (SII; American National Standards Institute [ANSI], 1997) value was calculated using the probe microphone and audiometric data. Participants completed questionnaires designed to evaluate perceived benefit, satisfaction and confidence in the fitting process. Additionally, the participants' preference between the SoundPoint fitting and the clinician fitting was compared in both a laboratory setting and a blinded multi-memory field trial. In this study, the authors found that a significant majority of participants preferred the fittings conducted via SoundPoint in terms of sound quality and perceived speech intelligibility.
The usability of SoundPoint was evaluated on four main metrics - ease of use, likeability, usefulness and learnability. Learnability is the capability of a software product to enable the user to learn how to use it and is an important factor in the design of complex software applications (Brooke, 1996). Figure 6 shows that 90% of participants found that SoundPoint was easy to use and that 75% of participants would want to use the system to adjust their hearing aids in the future. There were no major learnability issues found with SoundPoint (90% of participants) and 100% of the participants found SoundPoint to be a useful tool for evaluating the sound quality of different fitting parameters. In general, participants reported that the system was easy to use, intuitive and helpful in arriving at acceptable fitting settings.
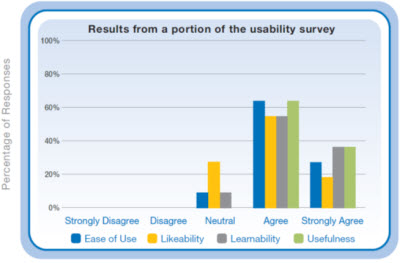
Figure 6. Results from selected questions from the usability survey administered to the subjects regarding SoundPoint. Ease of Use is based on the subject response to the statement "I thought that the system was easy to use"; Likeability, the statement "On my next visit, I would want my hearing-aid adjusted using this system"; Learnability, the statement "It was easy to get started when it came to learning how to use the interface"; and Usefulness, the statement "I found the system's interface (exploring the space with a mouse) an easy way of evaluating the quality of sound settings in my hearing-aid."
When the audibility data were considered, it was revealed that SII predicted speech recognition performance did not differ significantly between fitting approaches. Speech Intelligibility Index values were used to calculate predicted performance on the CST using the transfer function described by Sherbecoe and Studebaker (2002). As expected, predicted performance increased with stimulus presentation level, and no significant differences were observed between fitting conditions, indicating that participants were able to navigate to preferred settings that should produce similar speech intelligibility performance to that obtained via traditional fitting methods.
Fitting preference was investigated in a blinded all pairs comparison test in which each fitting was compared to each of the others a total of ten times. Participants listened to either a running passage of speech in quiet or in the presence of café background noise. Comparisons were performed to investigate preference in terms of perceived sound quality and perceived speech understanding. Figure 7 shows that in terms of sound quality the SoundPoint fitting was preferred over the clinician fitting 30% of the time where as the clinician fitting was only preferred over the SoundPoint fitting 3% of the time. The majority of the participants did not indicate a preference between the two fittings. Therefore, 97% of our subjects would have been pleased with the hearing aid settings obtained via SoundPoint. Similar results were found for the participants' perceived speech understanding preferences.
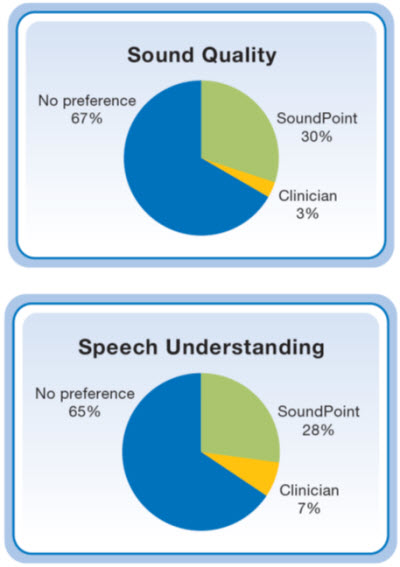
Figure 7. Percentage of statistically significant preferences for sound quality (top) and perceived speech understanding (bottom) for both the clinician fitting and the SoundPoint fitting.
During the third field trial, participants were asked to blindly compare the clinician settings and SoundPoint settings in the field via multi-memory switching. SoundPoint settings were preferred by more participants than the clinician settings (13 vs. 7); while 9 participants indicated that they had either no preference between the two settings or were not able to hear a difference between them. Despite the fact that 7 participants preferred the clinician fitting, and 9 did not indicate a preference, 27 participants reported that they would prefer to use their SoundPoint settings in the field for an extended period of time. These results suggest that the three primary goals of SoundPoint were achieved, as sound quality was highly adjustable while maintaining audibility, participants were able to navigate the system with ease, and preferred the results to those achieved by traditional methods.
The experimental and clinical trials conducted with SoundPoint validate the application of the system for the fitting and fine-tuning of hearing aids. Results of these studies demonstrate the benefits of patient-assisted hearing aid fittings. Based on these findings, professionals incorporating fittings using the SoundPoint tool can expect patients to experience greater perceived benefit and be more satisfied with their hearing aid fittings than traditional fitting methods.
Positively influencing perceived benefit and satisfaction of hearing aid wearers has been a challenge for clinicians for many years. Even measurable performance advantages will often result in little change in perceived benefit. It has been reported in the healthcare literature that increasing patient involvement in their healthcare decisions increases satisfaction with the treatment provided. The new body of research surrounding SoundPoint is consistent with these data. SoundPoint helps to bridge the gap between patient and clinician, easing communication and resulting in improved fitting outcomes.
References
Abrams, H., Edwards, B., Valentine, S., Fitz, K. (2011). A patient-adjusted fine-tuning approach for optimizing hearing aid response. Hearing Review, 18(3),18-27.
American National Standards Institute. (1997). Methods for the calculation of the speech intelligibility index (ANSI S2.5-1997). New York: Author.
Cox, R.M., & Alexander, G.C. (1987). Development of the connected speech test (CST). Ear & Hearing, 8(Supplement), 119S-126S.
Brooke, J. (1996). SUS: A "Quick and Dirty" Usability Scale. In P.W. Jordan, B. Thomas, B.A. Weerdmeester, I.L. McClelland (Eds.), Usability evaluation in industry (pp. 189-194). London: Taylor & Francis.
Dillon, H., Zakis, J.A., McDermott, H., Keidser, G., Dreschler, W., & Convery, E. (2006). The trainable hearing aid: what will it do for clients and clinicians? The Hearing Journal, 59(4), 30-36.
Frosch, D.L. and Kaplan, R.M. (1991). Shared decision making in clinical medicine: past research and future directions. American Journal of Preventive Medicine, 14(4), 285-294.
Kiessling, J. (2001). Hearing aid fitting procedures - state-of-the-art and current issues. Scandinavian Audiology, 30(1), 57-59.
Liejon, A., Eriksson-Mangold, M., & Bech-Karlsen, A. (1984). Preferred hearing aid gain and bass-cut in relation to prescriptive fitting. Scandinavian Audiology, 13, 157-161.
Sherbecoe, R.L. & Studebaker, G.A. (2002). Audibility-index functions for the connected speech test. Ear & Hearing, 23, 385-398.
Roberts, K.J. (1999). Patient empowerment in the United State: a critical commentary. Health Expectations, 2(2), 82-92.
