 From the Desk of Gus Mueller
From the Desk of Gus Mueller

It’s no secret that for many situations involving speech understanding, meaningful listening requires effort. When hearing loss is present, more effort is required, involving higher levels of mental processing and cognitive resources. And this effort often leads to listening fatigue. Because of this, hard-of-hearing individuals might “tune out” when listening effort increases considerably, or simply avoid these situations altogether.
It’s only been the last decade or so that listening-related fatigue has become commonly discussed among audiologists. One of the individuals who has led this discussion is Ben Hornsby, PhD. We invited him to bring us up to date on the topic here at 20Q two months ago (April ’26)—if you haven’t seen his excellent review article, you can find it here.
Obviously, our readers are very interested in the topic of listening fatigue, as in just two months, over 700 of you have read the article for CEUs. As you might guess from a Hornsby article, nearly all of the reviews were 4 or 5 stars. There was one 2-star rating, however, with the following comment:
“The meat of the topic was at question 19, and now I have to wait another month or two to get this information!”
It is true, Ben was just getting into the administration and scoring of the Vanderbilt fatigue scales, when our Mystery Question Person landed on the 20th Question (we do have rules). But . . . Anonymous Member, never fear, Dr. Hornsby is back, and he “brought the meat.”
Ben Hornsby, PhD, is an Associate Professor in the Department of Hearing and Speech Sciences at the Vanderbilt Bill Wilkerson Center, Vanderbilt University School of Medicine—a member of the Vandy faculty as teacher-scholar-researcher for the past ~25 years. Dr. Hornsby also directs the Hearing and Communication Research Laboratory at Vanderbilt.
Most of you know Dr. Hornsby from his 100 or more presentations and peer-reviewed journal articles, and his presentations at national and international scientific meetings. He has served as a Section Editor, Guest Editor, and reviewer for multiple scholarly journals. He is a Fellow of the American Speech-Language-Hearing Association and the International Collegium of Rehabilitative Audiology (ICRA).
This informative 20Q from Ben provides you with all the tools for implementing these scales into your routine practice—administration, scoring, and interpretation. You’ll easily be able to formally assess listening-related fatigue and use these findings in your counseling and treatment plans. Your patients will thank you.
Gus Mueller, PhD
Contributing Editor
Browse the complete collection of 20Q with Gus Mueller CEU articles at www.audiologyonline.com/20Q
20Q: Hearing Loss and Listening-Related Fatigue—Clinical Assessment
Learning Outcomes
After reading this article, professionals will be able to:
- Describe the development process and psychometric properties—including sensitivity, reliability, and validity—of the Vanderbilt Fatigue Scales for adults and children.
- Identify the appropriate qualitative and quantitative score cut-points for interpreting VFS results in adults and children, and explain the rationale for the modified criteria used with pediatric populations.
- Apply the Vanderbilt Fatigue Scales in clinical practice, including using scale results to guide patient counseling and measuring outcomes of interventions for listening-related fatigue.
1. Thanks for agreeing to another talk. I’ve been thinking a lot about “listening fatigue” since our last discussion.
I’m glad to hear our chat got you thinking about this issue. As I mentioned last time, the topic may not be the first issue raised by ALL your patients, but for some people with hearing loss, listening fatigue can be frequent, severe, and negatively affect their quality of life. So no problem, I’m happy to continue the discussion.

As I recall, when we finished our last talk, I was starting to tell you about some fatigue scales that we recently developed at Vanderbilt University Medical Center. The Vanderbilt Fatigue Scales (VFS’s) are the first scales specifically developed to measure listening-related fatigue. There are five versions of the VFS, two for use with adults (VFS-A) and three versions for use with children (VFS-Peds).
The adult scales include a 40-item version (the VFS-A-40; Hornsby et al., 2021) that, due to its length, is most appropriate for research purposes. The VFS-A-40 is a multidimensional measure that can provide a total fatigue score and four subscale scores: i.e., cognitive, physical, social, and emotional fatigue. The other scale for adults is the VFS-A-10, a brief, 10-item (a subset of VFS-A-40), unidimensional scale that can be used clinically or for research purposes (Hornsby et al., 2023). As you might guess, this is the one that has become the most popular among clinicians. You can see the test instructions and the first few test items of the VFS-A-10 in the image below.
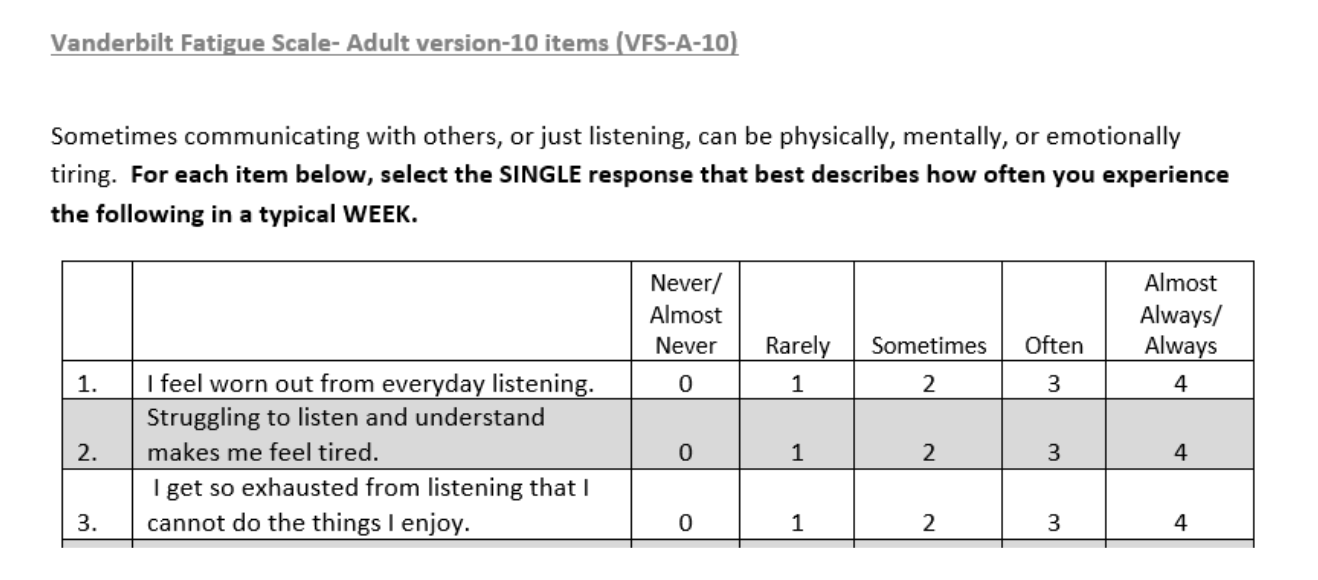
Figure 1. Instructions, example items, and response options for the VFS-A-10.
2. I like the fact it’s only 10 items. It looks like it is scored on a 0-4 scale, correct?
Yes, in fact, all of our scales use the same 5-point (0-4) Likert frequency scale with response options of “Never/Almost Never” (0 points), “Rarely” (1 point), “Sometimes” (2 points), “Often” (3 points), or “Almost Always/Always" (4 points), as shown in Figure 1. [The VFS-A-40 also has a few items that use a 5-point (0-4) Likert “agreement” scale (i.e., strongly disagree (0) to strongly agree (4)).]
For clinical purposes, you calculate an individual’s fatigue score by simply summing the responses across all scale items (or all subscale items). Higher scores reflect more frequent fatigue-related issues.1
Also, I’ll note that all our scales assess an individual’s “long-term” listening fatigue by asking about experiences during “a typical week” (See Figure 1).
3. Speaking of children, you said there are three more scales for assessing kids?
Right, you can assess listening-related fatigue in children using the pediatric versions of the VFS (VFS-Peds; Hornsby et al., 2022). This is a suite of measures that can be used for clinical or research purposes. It consists of a unidimensional child self-report scale (VFS-C; 10 items). While we developed this scale to be used with kids as young as 6 years old, we’ve found it is most appropriate for children aged 11-17 years. Given its complexity, younger children may struggle with the construct of fatigue.
You’re probably wondering, why do we need three scales? Clearly, whenever possible, it is preferable to have the person who is experiencing difficulty (e.g., fatigue) answer questions about their issues directly (i.e., via self-report). However, in some cases for example with young children, cognitive or developmental limitations may limit this option. In such situations, useful, and complementary, information can be obtained via proxy-reporting from parents or the children’s teachers.
This is why we included two additional proxy-report scales within the VFS-Peds. The VFS-P is a 12-item, multidimensional, parent proxy-report scale that contains two subscales (VFS-PMental- a 7-item mental fatigue subscale and VFS-PPhysical- a 5-item physical fatigue subscale). The VFS-P can be used to assess listening-related fatigue in children aged 6-17. Finally, the VFS-T is an 8-item, unidimensional, teacher proxy-report scale that can also be used with children aged 6-17.
Also, in terms of why three scales, in some cases, the parent or teacher can be more aware of the child’s fatigue than the child themselves. This may be especially true for children with long-standing hearing loss who have little insight into the uniqueness of their listening problems. The child who has grown up experiencing fatigue related to their hearing difficulties may be unaware that other children don’t experience the same thing. Parents and teachers, however, can compare the child’s issues with that of other children they interact with and can provide additional, complementary, information to the child’s self-report. In addition, there may be some children who are more aware of their fatigue issues than their parents or teachers. Thus, we encourage clinicians to administer all three scales when possible. Reports of significant fatigue-related issues by any respondent (child, parent or teacher) are of potential concern and may warrant follow-up.
4. Can I assume you’ve done some testing to ensure these scales are ready for clinical use?
No need to assume. Yes, we’ve done extensive work in this area. When developing scales there are three main areas to assess:
- Scale sensitivity: Does the scale precisely measure what you want it to (in our case listening-related fatigue)? i.e., is it able to detect small differences in fatigue between individuals or small changes in fatigue over time?
- Scale reliability: Are results obtained with the scale consistent internally and over time? i.e., Are responses across test items that are supposed to assess the same construct (e.g., VFS-P mental fatigue items) actually similar (internal consistency) and are responses stable over time (test-retest reliability)?
- Scale validity: Does the scale truly measure what we think it does (listening-related fatigue in our case)? i.e., Are scale results similar to results obtained using other fatigue measures and different from results of tests that don’t measure fatigue (construct validity)? And, do test items cover the full range of issues relevant to listening fatigue in people with hearing loss (content validity)?
If you want the nitty gritty details on how we assessed these things, look over our development and validation papers (Hornsby et al., 2021, 2022, 2023). But briefly, we started by following best practices for scale development (e.g., Boateng et al., 2018). Since there was no existing measure of listening-related fatigue, first we conducted focus groups and interviews with adults and children with hearing loss (and the parents and teachers/professionals who work with the children) and asked them about their experiences with listening-related fatigue. For example, was it a problem for them? What did it look like? What made it better or worse? We used this information to identify important themes that were relevant to the listening-related fatigue experienced by people with hearing loss (Davis et al., 2021a, 2021b). We also used comments from these meetings to create a large pool of potential test items (~100+ items for each scale) that addressed their fatigue-related issues. So, we know our scales have good content validity because the issues addressed and the test items themselves come, in large part, directly from the listening-related fatigue experiences of people with hearing loss.
5. 100+ items for a scale? That’s crazy. How did you decide which items to include in your final scales?
Yes, I’m pretty sure a 100-item scale wouldn’t be too popular with patients or clinicians! That said, identifying which test items were most effective was a multi-step process that did involve administering all 100+ items (for each scale) to lots of adults, children, parents and professionals (~200-600 respondents/group; we are very appreciative of everyone who took the time to help us do this!). We used multiple statistical approaches to analyze the data and shrink the large item pools to a smaller set of high-quality items for each scale. We then reanalyzed the results using the final, smaller, item pools (10 or 40 items for the VFS-A and 8-12 test items for each scale in the VFS-Peds) to confirm dimensionality, item quality, and other characteristics (e.g., construct validity) of our scales. For our clinical tools, the VFS-A-10 and VFS-Peds, we administered these final versions to additional (new) groups of adults (again ~200-600 respondents/group) and replicated the analyses using these new data sets. We also conducted “cognitive interviews” with adults and children with hearing loss (as well as parents and professionals) to ensure that all the final scale items were clear and understandable to the target populations.
6. After going through all that, were your early findings encouraging?
It was a multi-year, time-intensive, process. However, going through the kinds of steps I mentioned is critical if the goal is to develop a reliable, sensitive, and valid measure. And to answer your question, yes, the general findings were very encouraging. For example, in terms of sensitivity, all scales showed good precision (i.e., they provide a precise estimate of an individual’s listening-related fatigue) over a wide range of fatigue severities (i.e., only a little fatigue to very severe fatigue). Good precision makes the scales useful not only for identifying individuals with significant fatigue problems but also for detecting changes in their fatigue over time, or in response to an intervention. Again, if you are interested in statistical approaches that we used to assess sensitivity, you can look through the development and validation papers I mentioned above (Hornsby et al., 2021, 2022, 2023).
7. Thanks, but I’ll hold off on those papers for now. You said you also looked at test reliability?
Yes, and we were pleased to see that all our scales were reliable. That is they showed good internal consistency and good test-retest stability. Intraclass correlation coefficients (ICCs) provide a measure of scale stability over time. Values typically range between 0-1 with higher values reflecting better test stability. For our adult scale total scores, ICC values ranged from 0.68 (VFS-A-40; ~3-month test-retest period) to 0.95 (VFS-A-10; ~1-month test-retest period). ICCs for the VFS-Peds varied from 0.72 (VFS-T; ~2-week test-retest period) to .90 (VFS-P mental subscale; ~ 1-week test-retest period).
8. It sounds like you’ve created several great scales for measuring listening-related fatigue. How do you see these being used clinically?
Excellent question! We believe our scales can be useful in several ways.
- For identification: The most intuitive use is as an identification tool. As I mentioned last time, there is a subset of people with hearing loss who experience recurrent fatigue that is so severe it negatively affects their quality of life. Given this, I’d argue we should identify those people to see if their issues warrant monitoring (minimally) or some intervention to try and help reduce their fatigue-related problems.
- For counseling: Once an individual is identified as having significant fatigue problems, we believe clinicians can use responses to scale items to direct counseling and identify potential target issues or areas for intervention.
- As an outcome Measure: Should an intervention be warranted clinicians can use our scales as an outcome measure to assess the effectiveness of their intervention.
9. I work mostly with adults, which scale should I use? Would I give it to all my new and existing adult patients?
For clinical use with adults, we recommend using the VFS-A-10. It is simple and easy to use (~6th-7th grade Flesch-Kincaid grade reading level). Most adults can complete it on their own in 2-3 minutes.
In terms of who to give the scale to, some of our prior work suggests a strong association between perceived hearing difficulties and fatigue (Hornsby & Kipp, 2016; Alhanbali et al., 2018; Hornsby et al., 2024), so we suggest you administer the scale, at least initially, to anyone who has complaints of hearing difficulties. This would be new and existing patients, regardless of whether they use or don’t use hearing aids or other assistive listening devices. Whether you re-administered the scale on subsequent visits would depend on the patient’s initial score and any follow-up concerns.
10. Okay, let’s say I administered the VFS-A-10 to a new patient who was complaining about hearing problems. I summed the responses and got their total fatigue score- now what? How much fatigue is “too much”?
To make sure you are able to identify all individuals who may be experiencing fatigue that is so significant it could negatively affect their quality of life, we suggest you interpret your score both “qualitatively” and “quantitatively”. By qualitatively I mean in terms of the frequency of your patient’s fatigue-related complaints. Recall that all our scales use a 5-point Likert response format to ascertain the frequency of fatigue problems the individual experiences during a typical week. Response options range from 0 (meaning they never/almost never experience problems) to 4 (meaning they are always/almost always experiencing problems). Scores of 1, 2 or 3 indicate they experience the situations rarely, sometimes, or often, respectively. Thus, VFS scores (from any of our scales) tell us about how frequently a person is experiencing fatigue-related problems.
For example, given the VFS-A-10 has 10 items, a score of 40 tells us the person is “Always/Almost Always” experiencing fatigue-related issues- we know this because the only way you can get a score of 40 is by selecting “Always/Almost Always” in response to all 10 items. Likewise, a score of 0 means the person “Never” experiences any of the fatigue-related problems we queried them about.
While you can get scores of 10, 20, and 30 in multiple ways (i.e., by selecting multiple response options to different items), it is helpful to think of these values as if they were obtained by selecting the same response option for each test item. For example, scores of 10, 20 and 30 would be obtained if a respondent selected either “Rarely”, “Sometimes”, or “Often” to all 10 items, respectively. Using the same logic, a VFS-A-10 score ≤15 (midway between “Rarely” and “Sometimes”) suggests the person likely selected “Never” (0) or “Rarely” (1) to most test items (and perhaps occasionally a higher rating). Thus, if someone obtains a score of ≤15, it suggests that problems with listening-related fatigue are relatively rare for this individual (although they could experience fatigue issues in isolated instances). In contrast, to get a score of 25 (i.e., midway between “Sometimes” and “Often”) or greater, the individual likely selected “Often” (3) or “Always/Almost Always” (4) to most items (and perhaps occasionally a lower rating). Thus, individuals with scores of ≥25 are likely experiencing listening-related fatigue problems very frequently during a typical week, which increases the likelihood of their fatigue issues negatively affecting quality of life.
11. That seems reasonable, but I remember you said that everyone gets fatigued sometimes. Is there evidence that such “frequent” fatigue is uncommon or problematic?
Yes, there is. Research from our own lab has shown that such frequent fatigue-related issues (i.e., VFS-A-10 scores ≥25) are quite rare in adults without hearing loss. As part of our validation study (Hornsby et al., 2023), we collected VFS-A-10 responses from 220 adults with self-reported normal-hearing and NONE of them had scores >26. The median score was only 5 and ~88% of scores were ≤15 (suggesting fatigue-related issues were rarely occurring). Only one person without hearing loss had a score of 26. Figure 2 shows the distribution of scores for adults with and without hearing loss that were evaluated in that validation paper (Hornsby et al., 2023). The distribution of VFS-A-10 scores for adults without hearing loss is highly skewed towards lower scores and highlights the fact that scores of ≥25 are quite uncommon in this group (<1%).
Given how rare such scores are, we contend that ANY individual (with or without hearing loss) who is experiencing fatigue-related problems “Often-Almost Always” during a typical week (as reflected by VFS-A-10 summed scores of ≥25) warrants additional follow-up. I’ll add that ~25% of adults with hearing loss had scores >26 (Hornsby et al., 2023) and ~31% had scores ≥25, suggesting their fatigue-related issues were occurring “Often-Almost Always”. This is an important concept for clinicians to keep in mind when administering and interpreting any version of the VFS.2

Figure 2. Distribution of VFS-A-10 scores for adults with and without hearing loss (Adapted from Hornsby et al., 2023).
12. That all makes sense. You mentioned another “quantitative” interpretation approach. What is that?
Another way to determine whether a patient’s fatigue is concerning, is to compare their VFS score to “normative” scores, ie., scores from people who don’t have hearing loss or any other fatigue-related condition. A common approach is to calculate cut-offs, or cut-points, that are 1 or 2 standard deviations (SD) above the “normative” mean.
Using the VFS-A-10 data from the 220 adults with self-reported normal-hearing I mentioned above, we identified 1 and 2 SD cut-points of 13 (1 SD) and 19 (2 SD), respectively. Note that a VFS-A-10 score of 13 would suggest that fatigue-related problems were relatively rare (i.e., to get this low score respondents must select “Never” and “Rarely”-and occasionally a higher value- in response to most items). While this is the case for individuals without hearing loss, the impact of such infrequent fatigue on quality of life is unclear but well may be limited. Thus, using a VFS-A-10 score of 13 as a cut-point to identify individuals whose fatigue problems were causing significant negative effects would be inappropriate.
In contrast, individuals with scores that equal or exceed the 2 SD cut-point of 19 suggests their fatigue-related issues are, on average, occurring “Sometimes” (recall you would get a score of 20 if you selected “Sometimes” in response to all items on the VFS-A-10); although, in some situations they may be occurring more frequently (i.e., often or almost always). Given that scores of this magnitude are rare in adults without hearing loss, the 2 SD cut-point of ≥19 seems a reasonable marker for identifying those for potential follow-up, i.e., those with somewhat frequent fatigue-related issues that could negatively affect quality of life. Note that while VFS-A-10 scores of this magnitude (≥19) are rare for adults without hearing loss, almost half (~47%) of adults with hearing loss have scores in this range (Hornsby et al., 2023).
13. Do you recommend the same approach when interpreting VFS-Peds scores?
Yes, and to determine qualitative cut-points (i.e., VFS-Peds scores that suggest fatigue-related issues are occurring “Often-Almost Always”), we followed the same process described earlier, we just used the specific number of test items for a given VFS-Peds scale or subscale. For example, the VFS-PMental subscale has only 7 items, if the respondent selected “Sometimes” (2 points) or “Often” (3 points) in response to all 7 items they would have scores of 14 or 21, respectively. The midpoint of these scores is 17.5, so we rounded this and use a cut-point of ≥18 to identify children with “frequent” mental fatigue problems. Using the same process results in a VFS-PPhysical subscale cut-point of ≥13 and a VFS-T cut-point of ≥20. Since the VFS-C has 10 items, its cut-point is 25, the same as the VFS-A-10. The process of determining quantitative cut-points was also similar but we found some modifications were necessary to make sure we weren’t missing any children who were struggling with fatigue.
14. What sort of modifications did you need to make for the kid’s scales?
Well, one thing we noticed when analyzing data collected during the validation of the VFS-Peds (Hornsby et al., 2022) was that the distribution of scores for children with and without hearing loss overlapped substantially (See Figure 3) and much more so than they did for adults.

Figure 3. Distributions of VFS-C scores for a group of children with hearing loss (n = 116) and a group of typically developing children (no hearing loss or other parent-reported disability; n = 120). Data are from Hornsby et al. (2022), supplemented by additional participants collected at a later date (Davis et al., 2022).
This overlap occurs because fatigue-related problems in children without hearing loss seem much more common than for adults without hearing loss. Because the VFS-A-10 and the VFS-C use the same (0-4) Likert frequency ratings and both scales have 10 items, the range of possible scores (0-40) is also the same, easing comparisons between the adults and children. In contrast to the highly skewed distribution of normal hearing adults, the distribution of VFS-C scores for typically developing children (no hearing loss or any other disability) was broader and shifted to the right (towards higher scores). The median VFS-C score for children without hearing loss was 15- compared to only 5 in adults. In fact, about 12.5% of typically developing children had scores ≥25, suggesting their fatigue-related issues were occurring “Often-Almost Always”. Recall <1% of adults without hearing loss had scores in this range.
Using a quantitative approach, this rightward shift results in relatively high 1 and 2 SD cut-points compared to adults: 27 (1 SD) and 37 (2 SD) vs 13 and 19 for children and adults, respectively. Clearly using the 2 SD criterion (scores ≥37) for determining a cut-point, as we did with adults, would be inappropriate for children as it would suggest only those children who reported fatigue-related issues occurring "Almost Always" on virtually every test item would warrant follow-up. So, one modification we made for children was to recommend using a 1 (instead of 2) SD cut-point (i.e., scores ≥27) to identify children who may be experiencing fatigue-related issues that could have a negative academic, behavioral, or social impact. This value also seems reasonable as it approximates the qualitative cut-point score of ≥25, which captures children who are reporting fatigue-related issues occurring "Often-Almost Always".
In contrast, the median VFS-C score for children with hearing loss (median=20) was similar to that of adults with hearing loss (median=18), respectively. Likewise, the percentage of children with hearing loss who reported fatigue-related issues were occurring "Often-Almost Always" (VFS-C scores ≥25; ~34%) was similar to that of adults with hearing loss (VFS-A-10 scores ≥25; ~31%).
We saw similar patterns (i.e., overlap in distributions) when using the VFS-P and VFS-T to assess listening-related fatigue in children with and without hearing loss (data not shown). These findings suggest that listening-related fatigue may be especially problematic for children, regardless of their hearing status. Perhaps this is not surprising given the high listening demands routinely faced by children in academic settings.
15. You said using a 1 (rather than 2) SD cut-point criterion was one way you were trying to make sure you don’t miss kids who were actually struggling with fatigue. What was the other way?
The other way is by looking at the number of times a child says that a fatigue-related issue is occurring “Often” or “Almost Always”. In adults without hearing loss these two response options are rarely selected. In our “normative” VFS-A-10 sample of 220 adults without hearing loss, “Often” was only selected in ~4% of cases and “Always/Almost Always” was selected in <0.5% of cases.
Given how rare such responses are in adults without hearing loss, our underlying assumption is that it is potentially problematic whenever a child reports that a fatigue-related issue is occurring “Often” or “Almost Always” (i.e., selects either option when responding to a VFS item), regardless of their total (or subscale) score on a given VFS-Peds measure. Our concern is that a child with a lower total score (e.g., <27) could still be experiencing significant problems in a subset of situations. If so, we may want to address those specific settings. As such, we believe reviewing the number of situations (i.e., the number of test items) children are experiencing fatigue-related issues “Often” or “Almost Always” provides an additional metric for identifying children who may warrant follow-up, even when their total, or subscale, score on a given VFS-Peds measure does not exceed cut-point criterion. Specifically, as a complementary metric for children, we suggest using a criterion of 3 or more “Often” or “Almost Always” responses as a marker of concern, again, regardless of the child’s summed score.
This criterion was chosen based on statistical analysis of our VFS-Peds validation (Hornsby et al., 2022) and normative data sets (Davis et al., 2022). Using these data, we determined that across all scales (i.e., VFS-C, VFS-P, and VFS-T) respondents who selected 3 or more “Often” or “Almost Always” responses were significantly different, at a probability level of .8 (p < .2), from our normative samples (Davis et al., 2022). We chose to use a more liberal cutoff of p=.2 (instead of .05) because of the substantial overlap in the distribution of summed scores from our typically developing and hearing loss samples (Figure 3). For the VFS-P we chose to use a cutoff criterion based on the total number of “Often” or “Almost Always” responses across both the Physical and Mental subscales, rather than using subscale specific criterion. We felt this less conservative guideline was appropriate given our underlying assumption that frequent fatigue-related issues (regardless of the subscale) are of concern.
16. It sounds like there are a lot of different things to consider when interpreting scores for kids and adults! Do you have something I can use to make this easy to interpret on the fly?
Sorry, that’s on me. I do get a little carried away when explaining all this! In reality, administering the scales and interpreting scores is straightforward. Table 1 lists the criterion (cut-points) for the different versions of the VFSs. After administering a VFS, you’ll just compare your patient’s score to the cut-points listed in Table 1. For children, you’ll also check to see if they chose “Often” or “Almost Always” 3 or more times. Exceeding any of these criteria is a flag and suggests additional follow-up may be warranted.

Table 1. Guidelines for interpreting VFS scores across scale versions.
17. Let’s say I start giving the VFS-A-10 to my patients. What next? How do I talk with them about the results?
Good question. Clearly, the discussion you have will depend largely on the patient’s score and their responses to specific items. For example, let’s say their total score was relatively low (e.g., ≤15) suggesting fatigue-related issues were uncommon. Your discussion would be brief: you can explain that for some people, hearing struggles can lead to significant feelings of fatigue but that this doesn’t seem to be a problem for them, and then you go on with your normal counseling process.
The discussion would be quite different for someone experiencing more frequent fatigue-related issues. For example, Figure 4 shows actual VFS-A-10 responses for a 57-year-old male, seen for a hearing evaluation. His total score was 27, which exceeded both VFS-A-10 cut-off criteria. This suggests, compared both to normal hearing individuals and those with hearing loss, he is experiencing fatigue-related issues quite frequently. Feedback from clinicians suggests the questions and the patient’s responses, particularly when they respond “often” or “almost always” to an item, can be useful for guiding counseling discussion.

Figure 4. VFS-A-10 responses from a 57-year-old, male seen for a hearing evaluation at the Vanderbilt University Medical Center audiology clinic.
For this individual, a first step would be to acknowledge their problem — let them know that they aren't alone, that fatigue related to listening difficulties can be a real problem for some people with hearing loss, and educate them on the reasons for this connection (check out our prior 20Q discussion about why people with hearing loss may experience more listening-related fatigue if you need a refresher). We believe this education component can be an important rehabilitative tool. Having a better understanding of why and how hearing difficulties are related to their fatigue may allow the individual to take more control over situations that exacerbate their fatigue. Research shows that feelings of control can play an important role in determining whether fatigue will or will not develop in a given situation (Hockey, 2013).
In addition, clinicians can use scale to learn about specific situations or experiences that may be driving the individual’s fatigue. For example, you might ask the individual to “Tell me more about the everyday situations where you feel tired or worn out from struggling to listen and understand (Items 1 & 2).” Such discussions are not only useful in helping clinicians better understand the patient’s perspective on their fatigue, they can also help clinicians identify specific situations where fatigue-related issues occur most frequently and thus provide potential targets for interventions. This kind of information can be especially helpful for pediatric audiologists working with parents and IEP teams to address fatigue-related issues of children with hearing loss (See Davis and Hornsby, 2023 for case studies with children).
18. You mentioned interventions to help with fatigue. Are there effective interventions for listening-related fatigue?
Right, once you’ve identified someone who is having problems, the goal is to provide them with intervention options that may help reduce the issues they are experiencing. If your patient is being fitted with hearing aids, “reduction of listening fatigue” might be one of the items on the COSI. This discussion leads me to the third way we recommend the scales be used: as an outcome measure. I’d love to tell you that the literature was full of evidence-based interventions for reducing listening-related fatigue that have been shown to be both effective and efficacious. Unfortunately, systematic research in this area is just getting started. That said, there is some recent work showing that traditional interventions, specifically hearing aids and cochlear implants, can reduce listening-related fatigue (Holman et al., 2021; Hornsby et al., 2024).
For example, we recently published a longitudinal study examining changes in listening-related fatigue following receipt of a cochlear implant (Hornsby et al., 2024). We used the VFS-A-40 (scores can range from 0-160 on this scale) to measure listening-related fatigue in a group of CI candidates, and then again 2 weeks, 1, 2, 3, 6, and 12 months after their CI was activated. Mean fatigue levels (~100 out of the max 160 points) were quite high for CI candidates, suggesting they were having “frequent” fatigue-related problems. We saw a significant reduction in listening related fatigue as soon as 2 weeks post-activation. Fatigue levels continued to decrease, on average, out to 2-3 months post-activation before stabilizing at levels similar to that of experienced CI users (See Figure 5). Note that, by 12 months, average scores (~60 points) had decreased ~40 points from their pre-CI levels. This ~40-point change on the VFS-A-40, approximates a change of one response category (i.e., from “almost always” to “often” or “often” to “sometimes”, etc.). Such a large change suggests the benefit from receipt of a CI was not only statistically significant, but it was also clinically important (Jaeschke et al., 1989).

Figure 5. Changes in listening-related fatigue (VFS-A-40 scores) over time following receipt of a cochlear implant (CI). Also shown (at the 12-month time point for ease of comparison) are mean VFS-A-40 scores for groups of experienced (>12 months use) unilateral and bilateral CI users and a group of adults with self-reported normal hearing. Adapted from Hornsby et al (2024).
Holman et al. (2021) did a similar study looking at fatigue benefits from hearing aids in a group of new, adult hearing aid users. Consistent with Hornsby et al. (2024), they found hearing aids also provided a statistically significant reduction in listening-related fatigue (also measured using the VFS-A-40). Unfortunately, for those experiencing significant fatigue-related issues, the benefits provided by these traditional interventions may not be adequate. On Figure 5 we also plot the average VFS-A-40 score for a group of adults without any self-reported hearing loss (data from Hornsby et al., 2021). Their mean score of ~20 points suggests that they "rarely" to "never" experience listening-related fatigue issues. Note this is ~40 points lower than the experienced CI users (~60 points at the 12-month time point). Clearly cochlear implants help, but significant fatigue-related issues remain for many CI users.
19. Is there anything else besides a cochlear implant or hearing aids that we can do to help people who struggle with listening-related fatigue?
Quick answer, yes! That said, we need more research to empirically investigate the effectiveness of potential intervention options. In the interim, however, we believe that people with hearing loss and our own professional experiences can guide our counseling and intervention strategies. Recall, to develop our fatigue scales we conducted focus groups and interviews with adults and children with hearing loss, as well as parents of children with hearing loss and professionals who work with those children. These individuals told us about their experiences with listening-related fatigue, what issues led to its increase and what strategies they used to reduce or limit fatigue development. If you are interested in a detailed description of these focus groups and interviews, see Davis et al., 2021a, 2021b. However, here are some key points that may be relevant for both adults and children:
- Take steps to optimize the listening environment to maximize intelligibility and reduce listening effort—e.g., provide optimum amplification, reduce noise and reverberation, provide good visual cues, etc. Essentially, follow best practices. While we know that many factors can influence the magnitude of fatigue one experiences in a given setting, fatigue rarely develops without the application of effort. So, anything we can do to reduce applied effort in a setting has the potential to also mitigate fatigue.
- Utilize “listening breaks” when appropriate and/or schedule them into the day as needed. This was a recurrent suggestion from focus group participants- both adults and children (and their parents/teachers). Such “breaks” can take many forms, ranging from taking off assistive devices completely to a brief change in activity (e.g., shifting briefly from an active, and challenging, listening task to some other task). Clearly, children have less control than adults regarding when to take such breaks and what such breaks might entail and effective implementation would require coordination between the child and relevant adults (e.g., parents, teachers). See Davis and Hornsby (2023) for additional discussion of this issue in relation to children.
- Education: As we talked about earlier, educating adults and children with hearing loss, and those who work with them, about fatigue and its relation to their hearing loss and listening difficulties can be very beneficial. Such education is critical for adults and children to develop and enhance self-advocacy skills to better manage their fatigue-related issues. For example, a recent study by Klein et al. (2024) found that children who felt more comfortable asking to take a listening break (i.e., more comfortable self-advocating), reported less fatigue than those who were not comfortable doing so.
20. You’ve convinced me. I think this is something I’ll want to do with my patients. Are these freely available?
Absolutely! The scales are copyrighted, however, they can be downloaded and freely used for clinical or research purposes. Copies of the scales, user manuals, a summary sheet of management strategies for the pediatric population, and information on IRT scoring for those interested, are all available at a website we created for this purpose. This is the link https://www.vumc.org/vfs or just google “Vanderbilt Fatigue Scale” and it will get you to the website.
The scales have also gained broad international interest so if you have a non-English speaking patient you can check our site to see if the scale has been translated into their language. To date the VFS-A-10 and the VFS-Peds have been translated into 11 different languages. In addition, multiple collaborations with other research groups are ongoing and we hope to see them translated into even more languages in the near future. So, stay tuned!
References
Alhanbali, S., Dawes, P., Lloyd, S., & Munro, K. J. (2018). Hearing handicap and speech recognition correlate with self-reported listening effort and fatigue. Ear and Hearing, 39(3), 470–474. https://doi.org/10.1097/aud.0000000000000515
Boateng, G. O., Neilands, T. B., Frongillo, E. A., Melgar-Quiñonez, H. R., & Young, S. L. (2018). Best practices for developing and validating scales for health, social, and behavioral research: A primer. Frontiers in Public Health, 6, Article 149. https://doi.org/10.3389/fpubh.2018.00149
Davis, H., Camarata, S., Hornsby, B., & Bess, F. H. (2022). A user guide to the pediatric versions of the Vanderbilt Fatigue Scale (VFS-Peds). Vanderbilt University Medical Center; Vanderbilt Bill Wilkerson Center. https://www.vumc.org/vfs
Davis, H., & Hornsby, B. (2023). Listening-related fatigue in Deaf and hard of hearing students: Understanding and managing the "fatigue factor." The Volta Review, 123(1), 21–34.
Davis, H., Schlundt, D., Bonnet, K., Camarata, S., Bess, F. H., & Hornsby, B. (2021a). Understanding listening-related fatigue: Perspectives of adults with hearing loss. International Journal of Audiology, 60(6), 458–468. https://doi.org/10.1080/14992027.2020.1834631
Davis, H., Schlundt, D., Bonnet, K., Camarata, S., Hornsby, B., & Bess, F. H. (2021b). Listening-related fatigue in children with hearing loss: Perspectives of children, parents, and school professionals. American Journal of Audiology, 30(4), 929–940. https://doi.org/10.1044/2021_aja-20-00216
Hockey, G. R. (2013). A motivational control theory of fatigue. In G. R. Hockey (Ed.), The psychology of fatigue: Work, effort and control (pp. 132–154). Cambridge University Press.
Hornsby, B. W., Camarata, S., Cho, S. J., Davis, H., McGarrigle, R., & Bess, F. H. (2021). Development and validation of the Vanderbilt Fatigue Scale for Adults (VFS-A). Psychological Assessment, 33(8), 777–788. https://doi.org/10.1037/pas0001021
Hornsby, B. W., Camarata, S., Cho, S. J., Davis, H., McGarrigle, R., & Bess, F. H. (2022). Development and evaluation of pediatric versions of the Vanderbilt Fatigue Scale for Children with Hearing Loss. Journal of Speech, Language, and Hearing Research, 65(6), 2343–2363. https://doi.org/10.1044/2022_jslhr-22-00051
Hornsby, B. W., Camarata, S., Cho, S. J., Davis, H., McGarrigle, R., & Bess, F. H. (2023). Development and validation of a brief version of the Vanderbilt Fatigue Scale for Adults: The VFS-A-10. Ear and Hearing, 44(5), 1251–1261. https://doi.org/10.1097/aud.0000000000001369
Hornsby, B. W., & Kipp, A. M. (2016). Subjective ratings of fatigue and vigor in adults with hearing loss are driven by perceived hearing difficulties not degree of hearing loss. Ear and Hearing, 37(1), e1–e10. https://doi.org/10.1097/aud.0000000000000203
Hornsby, B. W., Picou, E. M., Ricketts, T. A., & Gifford, R. (2024). Listening-related fatigue in new and experienced adult cochlear implant users. Ear and Hearing, 45(4), 929–944. https://doi.org/10.1097/aud.0000000000001488
Jaeschke, R., Singer, J., & Guyatt, G. H. (1989). Measurement of health status: Ascertaining the minimal clinically important difference. Controlled Clinical Trials, 10(4), 407–415. https://doi.org/10.1016/0197-2456(89)90005-6
Klein, K. E., Harris, L. A., Humphrey, E. L., Noss, E. C., Sanderson, A. M., & Yeager, K. R. (2024). Predictors of listening-related fatigue in adolescents with hearing loss. Language, Speech, and Hearing Services in Schools, 55(3), 724–740. https://doi.org/10.1044/2024_LSHSS-23-00097
Footnotes
1 For researchers, the scales also allow for calculation of Item Response Theory (IRT) scale scores. These are a type of standardized score (like Z-scores) that use individual item weights to provide a more precise estimate of listening-related fatigue. However, these scores require computer calculations and are most appropriate for researchers when analyzing larger data sets. For our clinical discussion we’ll focus on the summed score.
2 The same process can be used to identify cut-points suggestive of fatigue-related issues that occur “Often-Almost Always” with all VFS measures. To do so the number of test items in the scale/subscale must be taken into account. See Table 1.
3 Given the VFS-A-40 has 40 test items, a score of 100 (out of a 160-point maximum) is analogous to a score of 25 (out of a 40-point maximum) on the 10 item VFS-A-10. Both scores suggest fatigue-related issues are occurring relatively frequently (i.e., somewhere between “Sometimes” and “Often”.
Citation
Hornsby, B. W. Y. (2026). 20Q: Hearing loss and listening-related Fatigue: Clinical Assessment. AudiologyOnline, Article 29691. Available at www.audiologyonline.com

