Medical professionals rely on auscultation to routinely examine the status of the circulatory, respiratory, and/or gastrointestinal systems. Auscultation is defined as listening to internal sounds of the body and represents an essential component in the delivery of health care services. The procedure is accomplished through the use of a stethoscope, a medical device specifically designed to enable physicians, nurses, and other medical professionals to detect and analyze heart, lung, and/or bowel sounds for purposes of differential diagnosis. The art of auscultation not only requires a level of clinical skill, but also assumes the presence of optimal listening conditions that would enable the practitioner to hear what needs to be heard.
For medical professionals with hearing loss, the routine use of traditional stethoscopes inherently creates several challenges. Physicians or nurses with hearing loss may experience difficulty hearing certain internal body sounds since the presence of a hearing loss may prohibit the ability to actually hear necessary heart, lung, and/or bowel sounds for differential diagnosis. While amplified stethoscopes designed to compensate for hearing loss are commercially available, medical professionals who are current users of amplification are faced with additional challenges that may preclude the successful use of amplified stethoscopes in conjunction with hearing instrumentation. The goal of this article is to provide audiologists with an overview of viable stethoscope options while also addressing associated limitations for purposes of facilitating realistic expectations.
Stethoscope Types & How They Work
There are two general types of stethoscopes, acoustic and electronic. Acoustic stethoscopes involve transmission of sound from a chest-piece to the listener's ears via an air-filled hollow tube. The dual-sided chest-piece contains a flat, disc-shaped disc called the diaphragm on one side and a smaller, disc-shaped bowl called the bell on the other side. While both heart and lung sounds are low frequency sounds, this dual chest-piece design enables users to better hear different body sounds since each specific body sound is tuned to a different frequency range. For example, the diaphragm is designed to pick up relatively higher pitched body sounds than the bell, specifically, it is typically used to listen to breath/lung sounds. While breath/lung sounds may range from 70 Hz to 4000 Hz (Cardionics, 2008), most fall under 2000 Hz (Noland, 2009). Perhaps the most critical lung sounds used for differential diagnosis fall in the 200 to 600 Hz frequency range (Abrams, 1987). The bell is designed to pick up lower frequency sounds. It contains a hole at its bottom center; when the hole is manually opened, the bell picks up lower frequency body sounds when cupped against the patient. The bell is more suitable for listening to heart sounds, which fall in the 20 Hz to 650 Hz frequency range (Rennert, Morris, & Barrere, 2004), although the most essential heart sounds for differential diagnosis fall in the 70 to 120 Hz frequency range (Noland, 2009; Cardionics, 2008).
Electronic stethoscopes work in the same manner as acoustic stethoscopes. The main difference between the two is that electronic stethoscopes are battery-operated devices designed to amplify body sounds so that they can be more easily heard. By the nature of this differentiation, all amplified stethoscopes are electronic in nature since they are designed to amplify body sounds to compensate for the presence of a hearing loss.
Audiological Considerations Associated with Auscultation
While there appears to be some discrepancy regarding the exact frequencies of various internal body sounds, in general, it ms important for audiologists to remember that both heart and breath sounds are essentially low frequency sounds. This becomes an important factor in ultimately establishing success with the practitioner interested in and motivated to using hearing instruments during auscultation procedures. Often times, the listening needs of the practitioner as dictated by audiometric configuration differ significantly from the listening needs of that same practitioner during routine auscultation procedures. While the audiogram may require the audiologist to program the hearing aid such that high frequency amplification is emphasized, the practitioner's need to use a stethoscope during routine clinical procedures requires the audiologist to provide a low frequency emphasis program. Furthermore, while hearing instruments may provide some flexibility in the low frequencies, the general frequency response of hearing instruments is not sufficient to adequately reproduce body sounds for differential diagnosis (Cardionics, 2008). As different options are either discussed or attempted with practitioners, it is critical for audiologists to keep in mind the listening needs associated with auscultation and to assess any potential limitations posed by current hearing instrument technology worn by the practitioner.
Amplified Stethoscopes for Non-Hearing Instrument Users
Medical professionals with hearing loss who are not current users of hearing instrumentation will achieve success in using one of several stand-alone amplified stethoscopes. In this context, stand-alone amplified stethoscopes refer to battery-operated, electronic stethoscopes specifically designed to amplify body sounds for those health care professionals with hearing loss who are not current wearers of hearing instruments. As shown in Figure 1, commercially available amplified stethoscopes include the Welch Allyn Master Elite, the 3M Littman, Electromax, and the Cardionics E-Scope II. As stand-alone products, these stethoscopes are not designed to interface with hearing instruments; rather, they are used in the same fashion as traditional stethoscopes with the exception that amplified stethoscopes provides amplification of heart and breath sounds. Each device offers the ability to switch between the two listening modes; the bell mode amplifies the much lower frequency heart sounds whereas the diaphragm mode amplifies breath sounds, which are relatively higher in frequency as compared to heart sounds.

Fig 1. Left to Right: WA Master Elite, 3M Littman, Electromax, and E-Scope II
Amplified Stethoscopes for the Hearing Instrument Wearer
For those medical professionals who are current wearers of hearing instrumentation, several options may be available although the selection of scope will be influenced by a variety of factors. First, potential solutions will be influenced by the specific type of hearing instrument worn by the practitioner in terms of whether the hearing instrument is a custom device, a traditional Behind-the-Ear (BTE), or perhaps an open-fit or receiver-in-the-ear (RITE) BTE. Second, hearing instruments equipped with t-coils may offer additional options to consider. Third, some solutions are associated with inherent drawbacks that may not be aesthetically acceptable to the practitioner. In other cases, the solution has traditionally been associated with marginal success. The best approach is to become familiar with viable options associated with each general situation and to address each situation as needed on a case-by-case basis.
Option 1: Removal of Hearing Instruments During Auscultation Procedures
The most straightforward option involves removal of hearing instruments prior to auscultation and relying on the use of a stand-alone amplified stethoscope (Figure 1A-1D). One of the drawbacks of this approach involves the constant removal and re-insertion of hearing instruments prior to and then following the use of a stethoscope. It is possible that practitioners with relatively mild degrees of hearing loss may be able to effectively communicate in a quiet patient-care environment without hearing instruments and rely on the use of an amplified stethoscope to hear necessary body sounds as a compensatory mechanism for their hearing loss. This may not represent the most ideal solution but in some instances, it may be a viable option.
Option 2: Use of Stethomate tips for Custom Hearing Instrument User
An ear canal occupied with a custom hearing instrument precludes the use of a traditional stethoscope earpiece unless a special adapter is incorporated onto the stethoscope's earpiece. Stethomate tips are such adapters for current users of custom hearing instruments (ITE through CIC) and are shown in Figure 2. These flexible adapters resemble the listening bell portion of a hearing aid listening stethoscopes although they are more substantial both in size and rigidity. Stethomate tips replace the original eartips of the stand-alone amplified stethoscope's earpiece; with the eartip of the earpiece removed, the narrower portion of the stethomate tip connects to the earpiece of the stethoscope. When the modified stethoscope earpiece is inserted in the ears, the wider portion of the stetomate tip makes contact with the outer most surface of the custom hearing instrument's faceplate with the cupped portion residing over the majority of the faceplate, including the microphone port.

Figure 2. Stethomate Tips
Theoretically, this configuration is designed to deliver body sounds from the stethoscope to the hearing instrument such that the body sounds may be amplified by the hearing instrument according to the practitioner's hearing needs. There are several challenges associated with using stethomate tips. First, the earpiece components of amplified stethoscopes are spring-loaded, making the stethoscope earpieces fit snuggly in the ear canal during use. Since custom hearing instruments also fit snuggly in the ear canal, the added pressure of the stethomate tips on the hearing instrument from the stethoscope's spring-loaded earpiece will create pressure on the hearing instrument such that using the amplified stethoscope may become somewhat uncomfortable. It is important to relay to customers both the potential comfort and functional challenges associated with stethomate tips. The issue of comfort is difficult to predict as it is influenced by factors such as ear canal anatomy and personal tolerances that will only become evident once the patient attempts this configuration.
The second challenge involves the need for the cupped portion of the stethomate tip to reside over the microphone of the hearing instrument. If the microphone port is located too close to the outer edge of the hearing instrument's faceplate, the solid, outer surface of the stethomate tip may actually cover and occlude the microphone port. In this case, the hearing instrument will not pick up sounds from the amplified stethoscope. The functional issue related to the stethomate tip achieving appropriate positioning over the microphone is difficult to predict.
Finally, in the event the stethomate tips fit comfortably and properly reside over the microphone port of the hearing instrument, the challenge in programming the hearing instrument to where it will adequately replicate low frequency auscultations for differential diagnoses remains questionable. At best, this solution is associated with minimal success. Medical practitioners pursuing this option should be made aware of the inherent limitation of stethomate tips in order to establish realistic expectations.
Option 3: Use of Special Earmold Designed to Interface with Custom Hearing Instruments
An earmold may be designed to interface with either a CIC or ITC, serving as an interface between the earpiece of the stethoscope and the hearing instrument. For CIC hearing instruments, the earpiece of the stethoscope resides in the recession of the special earmold with a sound bore drilled directly over the microphone opening (Morris, 2003). For ITC instruments, the stethoscope's earpiece is replaced with a screw-on ball designed to snap into a special earmold designed to interface with the hearing instrument (Morris, 2003). Stethoscope earpieces must be custom made for this application.
Option 4: Use of Amplified Stethoscope Configured to Interface with Hearing Instruments
Potential options for hearing instrument wearers will be influenced by several factors including general instrument type (i.e. custom versus BTE) and whether or not the hearing instrument is equipped with a t-coil. The following section will address each factor individually although it is important to keep in mind that a combination of these factors may need to be addressed in a particular patient situation.
Custom hearing instrument wearers
Beyond the stethomate tips previously mentioned, custom hearing instrument wearers have the option of using a version of the E-Scope II amplified stethoscope that has been specifically modified to interface with custom hearing instruments. As shown in Figure 3, this version resembles the traditional stand-alone E-Scope II model with the exception that the ear pieces have been completely removed. In lieu of the ear pieces, a pair of headphones are worn during auscultation while the custom hearing instruments remain in the ear canals. This configuration assumes that there is sufficient space between the microphone of the hearing instrument and the headphone cushion to avoid the potential for feedback. Two different headphone styles, traditional headphones and convertible headphones, are available (Figure 4). Traditional headphones (Figure 4a) will work with most custom hearing instruments; convertible headphones (Figure 4b), worn over or behind the head, will also work with most custom hearing instruments. In addition, an oversized headphone (Figure 4c) is available and may be necessary if the use of the standard or convertible headphones results in excessive feedback.

Figure 3. Modified E-Scope for use with custom hearing instruments

Figure 4A. Traditional headphones

Figure 4B. Convertible headphones

Figure 4C. Oversized headphones
Unfortunately, a common reaction to this configuration is one of reluctance on the part of the medical professional due to aesthetic concerns. Some medical professionals may feel self-conscious using a stethoscope in a non-traditional manner despite experiencing success. While audiologists can provide options and information, the individual in need of an amplified stethoscope will make the ultimate decision in terms of the solution of choice based on a variety of factors.
BTE hearing instrument wearers
Wearers of BTE hearing instruments have several potential options. The breadth of the solution pool for BTE wearers depends on several factors including whether the BTE is a traditional, open-fit, or receiver-in-the-ear (RITE) hearing instrument. Furthermore, additional options may be available in those instances where the BTE is equipped with a t-coil. This section will specifically address options related to general BTE types whereas the next section will address t-coil related options.
In this context, a traditional BTE hearing instrument refers to a BTE hearing instrument that is attached to an earmold via standard tubing. Open-fit instruments include smaller BTE devices that do not rely on earmolds; rather, these devices are equipped with a thin tube extending from the BTE instrument into the ear canal which remains anchored in the ear via a vented silicone dome. Finally, a RITE hearing instrument is similar to an open-fit instrument with the exception that the receiver of the instrument is resides in the ear canal rather than within the body of the BTE. Since the receiver resides in/the ear, electrical wiring replaces tubing in a RITE instrument.
Open fit or RITE BTE instrument wearer
There are two potentially viable solutions in this situation. Whether or not either solution leads to a successful outcome cannot be predicted ahead of time and will require taking the time and effort to try out. One potential option for wearers of open fit or RITE BTE instruments is to try and use any of the four previously mentioned stand-alone amplified stethoscopes (Figure 1A - 1D). Since open fit and RITE BTE instruments leave a good portion of the ear canal unoccluded, the patient may be able to use a stand-alone amplified stethoscope without having to take the hearing instruments out of the ears. The second option involves using the previously mentioned version of the E-Scope II (Figure 3) specifically modified to interface with custom hearing instruments whereby the patient would use the E-Scope II with a pair of traditional, convertible, or oversized headphones in lieu of the traditional ear pieces.
Traditional BTE
The general option for traditional BTE wearers tends to be limited to the use of the modified E-Scope II (Figure 3) with a pair of oversized headphones. In this situation, the oversized headphones are key since the headphones must be large enough to encompass the microphone of the BTE. Standard headphones are typically too small to sufficiently encompass the microphone port of the BTE and facilitate optimal listening. The one exception applies to those patients with normal low frequency hearing who wear an earmold with a reasonably large vent. In this situation, it may be possible to use standard headphones with the modified E-Scope II rather than the oversized headphone since the stethoscope sounds are directed into the ear canal via the large earmold vent rather than routed via the microphone of the BTE. According to Applebaum (2003), the vent should be at least 0.5 cm in diameter for this set up to be successful.
Another possible option for traditional BTE wearers is the use of a modified version of the E-Scope II designed to specifically interface with BTE instruments. This specific version closely resembles the previously described version of the E-Scope II modified for use with custom hearing instruments, however, instead of headphones, the hearing instruments interface with the amplified stethoscope either via direct audio input (DAI) (Figure 5A) or via an induction earhook such as a Silhouette (Figure 5B). In the DAI configuration, a special DAI cable connects to the stethoscope base and the other end of the DAI cable connects to the BTE via an audio shoe or boot. The signals are routed monaurally or binaurally to the BTE(s) via corresponding monaural or binaural DAI cables. For BTE wearers with equipped t-coils, an induction ear hook in the form of a Silhouette may be used to route signals to the BTE by way of the instrument's t-coil. The Silhouette plugs into the stethoscope base and then placed behind the ear between the mastoid bone and BTE. The sounds picked up by the E-Scope will be transmitted to the user's BTEs via the Silhouette by way of the t-coil.
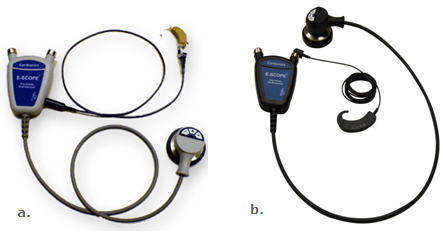
Figure 5. a). E-Scope II with DAI connection; b). E-Scope II with Silhouette
According to the manufacturer of the E-Scope, the DAI and Silhouette configurations typically have limited success and therefore should only be considered as a last resort. The frequency response of hearing instruments as well as the relatively small size of the hearing instrument's receiver is not generally conducive to reproducing low frequency body sounds favorably (Noland, 2009). Even with direct audio input into the hearing device, the sound quality needed to properly diagnose heart or lung sounds is lacking. Furthermore, the frequency response characteristics of a t-coil creates inherent challenges. T-coils are more sensitive to picking up frequencies above 1000 Hz whereas auscultation requires listening to body sounds that are of much lower frequency. This combination of factors significantly limits the viability of both configurations as potentially successful solutions. However, anecdotal reports from practicing audiologists indicate that this configuration represents a viable solution in some cases and, therefore, should not be immediately dismissed. Research exploring performance characteristics of hearing instruments configured to an amplified stethoscope is needed to assist in understanding the benefits and/or limitations of these solutions.
Conclusions
Offering medical professionals with hearing loss potential stethoscope solutions presents a challenging patient management issue for the audiologist. While viable options are available, there are inherent challenges ranging from aesthetic appeal to technological limitations that can lead to frustration for both the patient and the audiologist. Audiologists should assess the unique needs and preferences of each individual, establish realistic expectations, and be prepared to try one or more potential solutions before deciding upon the most appropriate course of action.
References
Abrams, J. (1987). Essentials of cardiac physical diagnosis. Philadelphia: Lea & Febiger.
Applebaum, S. (2003). Stethoscope use without behind-the-ear hearing aid removal. Journal of the Association of Medical Professionals with Hearing Losses,5(3). Retrieved January 29, 2010 from www.amphl.org/articles/applebaum2003.pdf
Cardionics (2008, April). Use of Phonak Savia hearing aids with E-scope electronic stethoscope. Technical Information Bulletin (No. E-7710) (Available from Cardionics, www.cardionics.com).
Morris, R. (2003, August 4). Cope with scopes: stethoscopes and hearing aids - what are the options? AudiologyOnline, Article 439. Direct URL: www.audiologyonline.com/articles/article_detail.asp?article_id=439 Retrieved January 29, 2010 from the Articles Archive on www.audiologyonline.com
Noland, M. (2009, September). Stethoscopes and hearing aids (Technical white paper issued by Cardionics, www.cardionics.com).
Rennert, N., Morris, F. & Barrere, C. (2004, February). How to cope with scopes: stethoscope selection and use with hearing aids and CIs. Hearing Review, p. 34-38.

