
Question
What Are the Key Fitting Priorities When Programming a MED-EL Cochlear Implant?
Answer
Understanding the Role of Maximum Comfortable Loudness
When fitting a MED-EL cochlear implant, the clinician's primary focus should be on measuring accurate Maximum Comfortable Loudness (MCL) levels. MCL represents the highest level of stimulation that remains comfortable for the patient - in other words, very loud but not uncomfortable, just below the threshold of discomfort. Appropriately set MCLs help preserve the natural loudness hierarchy of sounds in the patient's environment, ensuring that loud sounds are perceived as loud, medium sounds as medium, and soft sounds as soft. All other fitting parameters, including threshold (THR), stimulation strategy, and Automatic Sound Management (ASM) settings, can generally be left at their defaults to start. The MAESTRO software's default fitting parameters are based on years of clinical experience and feedback from audiologists and are appropriate for the majority of patients.
A Common Misconception: MCL and Environmental Loudness
A frequent question from clinicians new to MED-EL programming is whether setting MCL to maximum means the patient is always hearing at maximum loudness. The answer is no. With MED-EL, a patient only hears at MCL when two conditions are simultaneously met: the user volume setting is at 100%, and the input level is approximately 105 dB SPL. At all other times, stimulation occurs below MCL and is scaled to the actual sound input level (Stoebich et al., Ear & Hearing, 1999). This distinction is clinically important because it means that appropriately set MCLs allow for a full dynamic range of perception, rather than constantly stimulating at maximum levels. Clinicians should also keep in mind that MCL terminology and fitting ranges differ by manufacturer; always refer to the appropriate loudness growth chart for each cochlear implant brand.
Expected Map Shape and General Fitting Ranges
With MED-EL, most patients with normal cochlear anatomy and consistent neural survival will exhibit a flat MCL map shape across all electrode channels, with similar MCL values and similar pulse durations throughout. This flat configuration is both consistent and predictable, and clinicians should expect it as the baseline presentation. Average MCL levels typically range from 8 to 15 charge units (qu) at initial activation, rising to approximately 15 to 25 qu on a stabilized map. Caution is warranted when MCL levels are unusually high, as overstimulation can result in poor speech discrimination or, in more serious cases, Facial Nerve Stimulation (FNS).
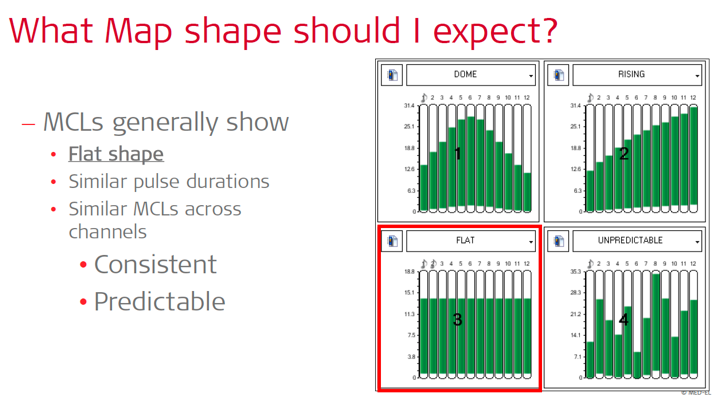
Figure 1. Four possible MCL map configurations in MED-EL MAESTRO software. The flat map shape (highlighted) is the expected presentation for patients with normal cochlear anatomy and consistent neural survival, characterized by similar MCL levels and pulse durations across all channels.
A Practical Quick-Fit Approach
For an efficient initial fitting, clinicians can use ARTFit or AutoART to set MCLs to ECAP thresholds - a conservative but audible starting point. From there, the clinician goes live in MAESTRO and raises MCLs globally using a loudness growth chart, confirming that normal conversational speech is comfortable and that the default volume is set to 100%. Progressive maps should be created to ease the patient into full stimulation levels over time. ASM parameters may be adjusted as clinically indicated; MED-EL's adaptive intelligence in the mild setting is recommended across all age groups. For bimodal users, bimodal synchronization should be configured before the processor is programmed. This streamlined workflow ensures that patients leave their initial appointment with access to their full dynamic range while minimizing the risk of overstimulation.
Patient Factors That May Affect Programming
Clinicians should keep several patient-specific factors in mind that may require adjustments beyond the standard fitting approach. A history of meningitis may be associated with cochlear ossification, difficulty reaching MCL, or non-auditory percepts such as FNS. Patients with enlarged vestibular aqueduct (EVA/LVA) may be more prone to map fluctuations. Temporary changes in loudness perception can also arise from active middle ear conditions, recent medication changes, or other health status shifts. Additional considerations include slower-than-expected progress, unreliable loudness reporters, inconsistent device use, long durations of auditory deprivation, and abnormal cochlear anatomy. MED-EL representatives are available to assist with complex programming concerns, and clinicians are encouraged to reach out when these situations arise.
This Ask the Expert is an edited excerpt from the course, Hedley-Williams, A. (2026) MED-EL Made Simple: A First Fit in 7 Easy Steps. AudiologyOnline. https://www.audiologyonline.com/audiology-ceus/course/med-el-made-simple-first-42074
Continued and its subsidiaries provide professional education authored by qualified Subject Matter Experts for continuing education purposes. These materials are intended for educational purposes and do not constitute medical advice or a substitute for individual clinical judgment. Continued is not a clinical healthcare provider; the licensed professional is solely responsible for ensuring that the application of any techniques or information presented is within their legal scope of practice and jurisdictional requirements.