The Hyperventilation Test: Unmasking Latent Vestibular Asymmetry
Introduction
The hyperventilation test (HVT) represents a peculiar and, in many respects, unique test within the spectrum of vestibular bedside examination. Unlike most clinical tests routinely employed in neurotology, the HVT does not directly stimulate the vestibular end organs but instead acts through systemic metabolic modifications that transiently alter the excitability of the vestibular system.
Over the past decades, several studies have clarified the mechanisms and clinical applications of hyperventilation-induced nystagmus (HVIN), highlighting its relevance in both peripheral and central vestibular disorders.
AudiologyOnline: Dr. Califano, what happens physiologically during hyperventilation, and why can this reveal vestibular asymmetries?
Dr. Luigi Califano: Hyperventilation is defined as ventilation exceeding metabolic requirements and is characterized by a reduction in arterial carbon dioxide tension (PaCO₂), leading to respiratory alkalosis.
This biochemical shift initiates a cascade of ionic and hemodynamic changes that affect both the central and peripheral nervous systems.
The decrease in PaCO₂ induces an increase in extracellular pH, which in turn modifies the distribution of hydrogen ions across cellular membranes. This process is coupled with ionic exchanges involving potassium and sodium, as well as an increase in intracellular calcium mediated by voltage-dependent channels sensitive to pH variations. At the same time, the concentration of ionized extracellular calcium decreases, further contributing to neuronal hyperexcitability.
In parallel, hypocapnia causes cerebral vasoconstriction and a reduction in tissue oxygenation, partly due to the leftward shift of the hemoglobin dissociation curve. These changes result in a complex interplay of metabolic and hemodynamic effects, including cellular hypoxia, alterations in cerebrospinal fluid pH, and modifications in intracranial pressure.
These changes may produce two main neurophysiological effects:
- Increased neuronal excitability, with a lower threshold for action potential generation.
- Transient disruption of central vestibular compensation, particularly of cerebellar inhibitory mechanisms that normally suppress vestibular asymmetries.
This second mechanism is especially important. In many vestibular disorders, particularly during chronic or compensated stages, central adaptation can mask peripheral deficits. Hyperventilation may temporarily reduce this compensatory effect, allowing the underlying vestibular asymmetry to re-emerge as nystagmus.
Pathophysiological basis of the HVT is summarized in Figure 1.
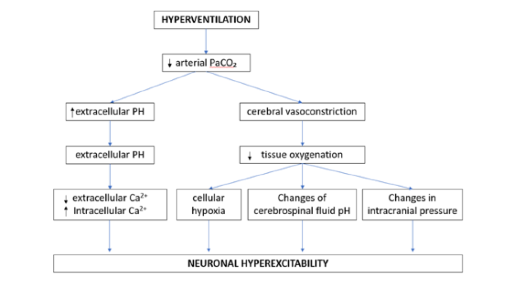
Figure 1: Pathophysiological basis of the hyperventilation test
AudiologyOnline: Dr. Martellucci, how is the hyperventilation test performed in daily clinical practice, and how should a positive response be interpreted?
Dr. Salvatore Martellucci: The hyperventilation test is typically performed with the patient in a seated position. The subject is instructed to perform rapid and deep respiratory cycles for approximately 60–70 seconds. Eye movements should be observed during hyperventilation and for at least one minute afterward, preferably using infrared video goggles, such as the Inventis Nystalyze system.
The test is considered positive when hyperventilation induces a nystagmus lasting at least a few seconds or when it significantly modifies a pre-existing spontaneous nystagmus. In videonystagmographic terms, variations in slow-phase velocity on the order of 5°/s are considered clinically relevant.
Despite its simplicity, the HVT requires careful execution and interpretation. Factors such as patient cooperation, depth of ventilation, and the method used to observe eye movements can significantly influence its sensitivity.
AudiologyOnline: Dr. Califano, how can hyperventilation modify spontaneous nystagmus, and how should the different HVIN patterns be interpreted?
Dr. Luigi Califano: The HVT may evoke nystagmus in a patient who does not exhibit it at baseline, or it may modify a pre-existing spontaneous nystagmus. Califano et al. identified four distinct patterns:
The paretic pattern is characterized by an enhancement of spontaneous nystagmus, typically beating toward the healthy side. This pattern is generally interpreted as the expression of an increased asymmetry between the two vestibular systems, resulting from the transient disruption of central compensation.
In contrast, the excitatory pattern consists of a reduction or inhibition of spontaneous nystagmus. In this case, hyperventilation appears to transiently improve the function of the affected side, possibly through enhanced neural conduction in partially demyelinated fibers or increased excitability of residual peripheral receptors. A strongly excitatory pattern, in which the direction of nystagmus is reversed, can be considered an extreme form of this mechanism.
Finally, in some cases, hyperventilation produces no observable effect, resulting in an absent HVIN pattern.
AudiologyOnline: Dr. Martellucci, in which clinical scenarios can the HVT provide the most useful diagnostic information?
Dr. Salvatore Martellucci:
PERIPHERAL VESTIBULAR DISORDERS
In peripheral vestibular disorders, the HVT is particularly useful for characterizing the stage and the probable origin of the disease. In the early phase of acute unilateral vestibulopathy, excitatory or strongly excitatory patterns may predominate, reflecting transient hyperexcitability or partial recovery of neural conduction in the affected vestibular nerve, thus supporting the hypothesis of vestibular neuritis. As the disease evolves, these patterns tend to disappear and are replaced by a paretic pattern.
In contrast, an absent or paretic HVIN in the early phase is more suggestive of the vascular origin of vestibulopathy.
RETROCOCHLEAR PATHOLOGY
The HVT shows particularly high diagnostic yield in vestibular schwannoma, with HVIN observed in the vast majority of cases. The presence of an excitatory pattern is especially suggestive of neural involvement, likely reflecting demyelination and altered conduction properties. In patients with unilateral auditory symptoms, particularly when the onset is not recent, this finding should prompt further investigation with MRI. A paretic pattern may nonetheless be observed in vestibular schwannomas, either in the absence of areas of demyelination, as is more likely in smaller tumors, or conversely in the presence of disruption of the nerve fibers, as frequently occurs in larger schwannomas.
CENTRAL VESTIBULAR DISORDERS
In central disorders, hyperventilation may produce different effects. In healthy subjects, cerebellar inhibitory activity compensates for the predominance of forces driving the eyes upward. In cerebellar disorders, the metabolic changes induced by the HVT may further impair cerebellar inhibitory function, thereby unmasking a downbeat nystagmus.
In other central conditions, particularly demyelinating diseases such as multiple sclerosis, hyperventilation may evoke or modulate nystagmus through different mechanisms. The induction of either upbeat or downbeat nystagmus is highly suggestive of an underlying demyelinating disorder.
AudiologyOnline: Dr. Califano, what key message should clinicians take away regarding the use of the HVT?
Dr. Luigi Califano: In conclusion, the hyperventilation test represents a powerful and versatile tool in vestibular diagnostics. Its ability to reveal latent asymmetries and to provide insight into underlying pathophysiological mechanisms makes it particularly valuable in the evaluation of complex vestibular disorders.
However, its interpretation requires a comprehensive clinical framework and should always be integrated with other findings from the vestibular examination.
References
Califano, L., Melillo, M. G., Vassallo, A., & Mazzone, S. (2011). Hyperventilation-induced nystagmus in a large series of vestibular patients. Acta Otorhinolaryngologica Italica, 31(1), 17–26.
Califano, L., Mazzone, S., & Salafia, F. (2013). Utility of the hyperventilation test in the evaluation of the dizzy patient. Current Opinion in Otolaryngology & Head and Neck Surgery, 21(5), 487–491. https://doi.org/10.1097/MOO.0b013e328364a8bb
Califano, L., Iorio, G., Salafia, F., Mazzone, S., & Califano, M. (2015). Hyperventilation-induced nystagmus in patients with vestibular schwannoma. Otology & Neurotology, 36(2), 303–306. https://doi.org/10.1097/MAO.0000000000000699
Califano, L., Salafia, F., Melillo, M. G., & Mazzone, S. (2017). Sensitivity and specificity of vestibular bed-side examination in detecting VIII cranial nerve schwannoma with sensorineural sudden unilateral hearing loss as presenting symptom. Acta Otorhinolaryngologica Italica, 37(4), 336–340. https://doi.org/10.14639/0392-100X-1284
Califano, L., Locatelli, G., & Melillo, M. G. (2022). Can hyperventilation test and duration of spontaneous nystagmus help differentiate between vascular and inflammatory aetiology of acute unilateral vestibular deficit? Acta Otorhinolaryngologica Italica, 42(6), 560–568. https://doi.org/10.14639/0392-100X-N1975
Chee, N. W., & Tong, H. M. (2002). Acoustic neuroma presenting as exercise-induced vertigo. The Journal of Laryngology & Otology, 116(8), 630–632. https://doi.org/10.1258/00222150260171641
Ciacca, G., Di Giovanni, A., Giacomo, L., Gullà, M., Ricci, G., & Faralli, M. (2024). Hyperventilation-induced nystagmus in acute unilateral vestibulopathy: A correlation with vestibulo-ocular reflex gain and clinical implication. The Journal of International Advanced Otology, 20(2), 164–170. https://doi.org/10.5152/iao.2024.231313
Hong, J. H., Yang, J. G., Kim, H. A., Yi, H. A., & Le, H. (2013). Hyperventilation-induced nystagmus in vestibular neuritis: Pattern and clinical implication. European Neurology, 69(4), 213–220. https://doi.org/10.1159/000345802
Huh, Y. E., & Kim, J. S. (2013). Bedside evaluation of dizzy patients. Journal of Clinical Neurology, 9(4), 203–213. https://doi.org/10.3988/jcn.2013.9.4.203
Kim, CH., Jeong, K. H., Ahn, S. H., Shin, D. H., Kim, Y. W., & Shin, J. E. (2015). Vibration- and hyperventilation-induced nystagmus in patients with Ramsay Hunt syndrome with vertigo. Otolaryngology–Head and Neck Surgery, 152(5), 912–918. https://doi.org/10.1177/0194599815570283
Lee, S. U., & Tarnutzer, A. A. (2025). Usefulness of nystagmus patterns in distinguishing peripheral from central acute vestibular syndromes at the bedside: A critical review. Journal of Clinical Neurology, 21(2), 161–172. https://doi.org/10.3988/jcn.2025.0105
Mandalà, M., Giannuzzi, A., Astore, S., Trabalzini, F., & Nuti, D. (2013). Hyperventilation-induced nystagmus in vestibular schwannoma and unilateral sensorineural hearing loss. European Archives of Oto-Rhino-Laryngology, 270(7), 2007–2011. https://doi.org/10.1007/s00405-012-2236-8
Monday, L. A., & Tétreault, L. (1980). Hyperventilation and vertigo. The Laryngoscope, 90(6), 1003–1010. https://doi.org/10.1002/lary.1980.90.6.1003
Robichaud, J., DesRoches, H., & Bance, M. (2002). Is hyperventilation-induced nystagmus more common in retrocochlear vestibular disease than in end-organ vestibular disease? Journal of Otolaryngology, 31(3), 140–143. https://doi.org/10.2310/7070.2002.10796
Staab, J. P., Ruckenstein, M. J., Solomon, D., & Shepard, N. T. (2002). Exertional dizziness and autonomic dysregulation. The Laryngoscope, 112(8), 1346–1350. https://doi.org/10.1097/00005537-200208000-00005
RESOURCES FOR MORE INFORMATION
For more information about Inventis, visit https://www.inventis.it/en-na


Luigi Califano, MD
Specialist in ENT and Audiology, Director of the Audiology Unit at the AORN San Pio Hospital in Benevento; speaker at numerous Italian and international conferences in the field of Audiology and Vestibology; organiser of training courses in Audiology and Vestibology since 2011; author of numerous scientific publications in peer-reviewed journals on Audiology and Vestibology.

Salvatore Martellucci, MD
Salvatore Martellucci is ENT medical director at the Latina Hospital. He deals with the treatment of ear, nose and throat pathologies in adults and children but also with the diagnosis and treatment of sleep apnoea, an increasingly common pathology associated with high cardiovascular risk. In addition to his outpatient activities and endoscopic diagnostics, he performs surgery in hospital and in private practice. Dr. Martellucci's main fields of interest are functional rhino-sinus surgery, cosmetic surgery of the nose, endolaryngeal phonosurgery, snoring and obstructive sleep apnoea surgery. He is a speaker at various congresses, seminars, webinars and author of publications in national and international scientific journals.