Over the past several years there have been many prescriptive fitting formulas developed and tested to fit hearing aids. These fitting formulas have evolved from providing a single target curve for linear instruments to providing 2 or more target curves for wide dynamic range compression (WDRC) hearing aids. For example, NAL, developed by the National Acoustics Laboratory of Australia (Bryne & Dillon, 1986), was designed for fitting linear circuits1. However, with the advent of WDRC circuits, a fitting algorithm was needed that could provide multiple gain curves for multiple input levels.
Clinicians typically view prescriptive target curves (e.g., for soft, average, and loud input levels) as the starting point, used to preliminarily set the electroacoustic characteristics for fitting hearing instruments. Depending on the patient's subjective comments, preferences and observations, final use gain settings will vary from these initial settings.
Two separate studies, Leijon, et al. (1990) and Gerling (1992) compared patient preference between prescribed gain and preferred use gain.2,3 Prescribed gain was defined as gain closely matched to NAL targets, whereas preferred gain was defined as the gain level at which patients wore their hearing aids on a daily basis. All subjects were fit with linear analog instruments. Real ear measurements were conducted to ensure that hearing aid gain closely matched prescribed targets. Results revealed that most subjects preferred less gain than was prescribed. Gerling hypothesized that "prescribing the same gain for all individuals simply because they have the same hearing thresholds will result in inaccuracies of too little as well as too much gain."
While it may be unrealistic to expect any fitting formula based on threshold or supra-threshold data to tell us precisely how much gain will be required for a particular patient, it is desirable. To initially fit the patient with gain (and other) settings that maximally approximate final use settings, has long been the ultimate goal of hearing aid prescription fitting formulas. Therefore, it is our goal to determine the final settings as quickly as is possible, i.e., "final settings first." Accomplishing the goal of determining the final settings first, will theoretically reduce the patient's acoustic discomfort when first fit, will reduce the number of hearing aid "check" appointments, will increase user satisfaction, will reduce returns for credit based on acoustic issues, will reduce the number of follow-up visits required for parameter adjustments, and will contribute overall to a smoother, less stressful adaptation process. It's no wonder then that so many fitting formulas have been proposed.
Beltone Electronics Corporation tackled this challenge in 1996 when we introduced a two-channel, WDRC circuit, called the CSP-II. We wanted an algorithm that would provide target gain curves for soft, average, and loud inputs. Loudness growth theory told us that restoring loudness to approximate the loudness perception of a normal listener (i.e., a soft sound is perceived as soft, average is average, and loud is loud) would result in greater patient satisfaction with amplification. However, we also realized that, despite our best efforts, we would not always have complete loudness growth data provided with every hearing instrument order. Therefore, we needed an algorithm that could adapt its targets based on the quantity of information available. The result was Beltone's Adaptive Fitting Algorithm (BAFA).
In reviewing the many different, previously available, hearing instrument fitting algorithms, we determined that algorithms appear to share 4 common goals:
- To make speech audible.
- To increase speech intelligibility.
- To provide a range of loudness, and,
- To keep sounds below the patient's discomfort level.
In some cases, these goals are unfortunately, somewhat mutually exclusive. For example; Which is more important, normalizing loudness, equalizing loudness, or maximizing intelligibility? To the hearing impaired patient, all are important. However, depending on the hearing loss, the auditory processing ability of the patient, the desired acoustic signal and the noise environment within which the desired signal "lives", the result of amplification will vary.
Loudness normalization makes sounds that are soft/average/loud for normal listeners perceived as soft/average/loud for hearing impaired listeners. Intuitively, this makes sense; however, such a formula results in more low frequency gain, relative to mid-and-high frequency gain. Unfortunately, loudness normalization can cause problems regarding intelligibility due to the upward spread of masking. A loudness equalization approach makes all speech sounds equally loud. While this is not how normal listeners perceive speech, it may provide better speech intelligibility for some hearing impaired listeners. If maximizing speech intelligibility is the goal, appropriate (and variable) gain must be applied to each frequency band to make all speech sounds equally loud. Combining the attributes of loudness normalization and loudness equalization may make more speech sounds available to the patient, while maintaining a comfortable listening environment.
BAFA combines loudness normalization and loudness equalization. The prescription which BAFA recommends is dependent on the data entered. When both thresholds and loudness data are entered, the fitting formula follows more of a loudness normalization approach. However, if only puretone thresholds are provided, BAFA estimates loudness perception levels and uses a loudness equalization approach.
The prescription targets are estimated using loudness data collected by Beltone's Research Audiology Department for normal listeners, and 1/3 octave band data from Cox and Moore, 1988.4 Combining the patient's thresholds with our loudness data and the Cox and Moore work, a mathematical equation extrapolates the probable loudness data for the patient. Targets are based on normalizing loudness and factoring in reduced low frequency gain to yield equalized loudness for speech, i.e., less gain for low frequencies. The target for soft inputs (50dB) have less low frequency reduction than for high inputs (Bass Increase at Low Levels, or 'BILL') while targets for average inputs (70dB) approximate NAL-RP targets (Bryne & Cotton, 1988).5
In cases where only threshold data is available, estimating loudness has been found to be satisfactory in setting preliminary target gain. Some studies have suggested that estimated loudness measures may be just as valid as measured MCLs and UCLs (LDLs) in setting prescriptive targets. Cox & Bisset (1982) found MCLs and UCLs can vary greatly among individuals. They commented "There is a predictable relationship between MCLs and UCLs on the average. However, it is probably naïve to expect that an estimate of comfortable loudness will be all that is needed to make very accurate predictions of aided preferred listening level (PLL) in each individual case. Investigations are needed of factors other than comfortable loudness which may determine an individual's aided PLL. Such factors might include: speech intelligibility, distortion, background noise, or personality traits." 6 An investigation of their proposed factors may demonstrate if individual evaluations of loudness comfort levels are superior to estimated loudness data in deriving target gain curves.
A complete data profile for BAFA calculations includes thresholds and three loudness points: Lower Level of Comfort (LLC), Upper Level of Comfort (ULC), and Loudness Discomfort Level (LDL). With most hearing instrument orders dispensers provide thresholds and LDL levels. As previously mentioned, BAFA will estimate missing data points using normative loudness (internally collected) data. The goal of the BAFA fitting prescription is to maintain the relationship among soft, average, and loud sounds. Sounds that are soft/average/loud for normal listeners are perceived as soft/average/loud for the hearing impaired listener. To determine the LLC and the ULC, we compare the normal dynamic range (threshold to LDL) to the reduced dynamic range, as shown by the hearing loss threshold-LDL difference. We then plot the missing LLC and ULC, taking care to maintain the relationships among the four points (see figure 1).
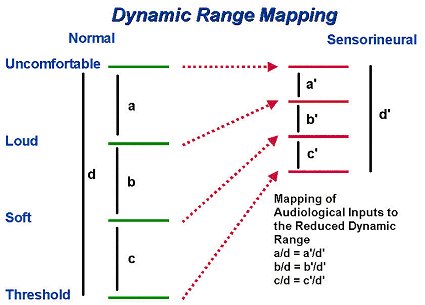
Figure 1: Mapping of Audiological Inputs to the Reduced Dynamic Range. Normative data is constant. Impaired thresholds are entered. Impaired LDLs are entered or extrapolated. Then, ULCs and LLCs are mapped to maintain the proportions between the normal dynamic range and the hearing impaired dynamic range.
Targets are then generated, bearing these principles in mind:
- for loud inputs, the ULC of the impaired listener should match the ULC of the normal listener
- for soft inputs, gain should equal the difference between the normal threshold and the impaired threshold, providing the loss is in the mild-moderate range
- for severe losses, gain for soft inputs is reduced to match the normal LLC
- gain for average inputs is interpolated to fall between the loud and soft gain levels.
The resulting target curves will demonstrate that:
- For mild losses, the gain difference between soft and average sounds will be greater than between average and loud sounds
- for moderate losses, the three gain curves will be equally distributed, i.e., approximately the same amount of gain difference will be provided between the average and soft or loud inputs
- for severe losses, the gain difference between the soft and average sounds is smaller than between the average and loud sounds.
During developmental field trials we discovered that the generated gain for soft inputs was producing unacceptable complaints regarding feedback. Consequently, the formula was amended to reduce high frequency gain for soft inputs. This illustrates a constraint on the mathematical prescriptive formula due to limitations of hearing instrument circuitry and issues related to the physical fit, size and dimensions of the ear canal and the hearing instrument. As advanced circuitry evolves we expect these constraints to lessen, and perhaps be eliminated entirely.
BAFA has been successfully used with analog and digital hearing instruments. BAFA has proven to be an effective starting point for fitting all hearing instrument styles and circuits. Our goal remains to initially fit the patient with gain (and other) settings that maximally approximate final use settings, while appreciating the inherent unpredictability of personal preference in judging satisfactory hearing instrument gain.
Topics still to be studied include, but are not limited to, examining the differences between BAFA targets and final use gain; comparing the effects of using measured vs. average loudness levels; and determining the effects of hearing aid wearing experience on final use gain levels.
The BAFA formula was developed by Stavros Basseas Ph.D and Mary Meskan Ph.D. The authors wish to acknowledge their contributions to the BAFA protocol, and their assistance in developing this article.
References:
1. Byrne, D. and Dillon, H. 1986. "The National Acoustic Laboratories' (NAL) New
Procedure for Selecting the Gain and Frequency Response of a Hearing Aid." Ear and Hearing. 7. pp.257-265.
2. Leijon, A.; Lindkvist, A; Ringdahl, A.; Israelsson, B. 1990. " Hearing Aid Gain in Everyday Use After Prescriptive Fitting." Ear and Hearing. 11. pp. 299-305.
3. Gerling, I. 1992. "Evaluation of Prescriptive Fitting." Journal of the American
Academy of Audiology. 3(5). pp. 331-337.
4. Cox, R. and Moore, J. 1988. "Composite Speech Spectrum for Hearing Aid Gain Prescriptions." Journal of Speech and Hearing Research. 31(1). pp.102-107.
5. Byrne, D. and Cotton, S. 1988. "Evaluation of the National Acoustic Laboratories' New Hearing Aid Selection Procedure." Journal of Speech and Hearing Research. 31(2). pp.178-186.
6. Cox, R. and Bisset, J. 1982. "Prediction of Aided Preferred Listening Levels for Hearing Aid Gain Prescription." Ear and Hearing. 3(2). pp. 66-71.
Additional Suggested Readings:
Byrne, D. 1986a. "Effects of Bandwidth and Stimulus Type on Most Comfortable Loudness Levels of Hearing-Impaired Listeners." Journal of the Acoustical Society of America. 80. pp. 484-493.
Byrne, D. 1986b. "Effects of Frequency Response Characteristics on Speech Discrimination and Perceived Intelligibility and Pleasantness of Speech for Hearing Impaired Listeners." Journal of the Acoustical Society of America. 80. pp. 494-504.
Byrne, D. 1996. "Hearing Aid Selection for the 1990s: Where to?" Journal of the American Academy of Audiology. 7. pp. 377-395.
Byrne, D. and Dillon, H. 1986. "The National Acoustic Laboratories' (NAL) New Procedure for Selecting the Gain and Frequency Response of a Hearing Aid." Ear and Hearing. 7. pp.257-265.
Byrne, D. and Tonisson, W. 1976. "Selecting the Gain of Hearing Aids for Persons with Sensorineural Hearing Impairments." Scandinavian Audiology. 5. pp.51-59.
Dillon, H. and Storey, L. 1998. "The National Acoustic Laboratories' Procedure for Selecting the Saturation Sound Pressure Level of Hearing Aids: Theoretical Derivation." Ear and Hearing. 19(4). pp. 255-266.
Click here to visit the Beltone website.
