
One of the biggest fitting challenges for hearing care professionals is handling the high expectations of hearing instrument users. With modern technology, wearers seek high speech intelligibility in noise and a high level of overall listening comfort in a variety of acoustic environments. In addition, many of these consumers desire hearing instruments that are discrete, easy to use, comfortable to wear, and robust. A new product, CENTRA Active, combines the latest advancements in signal processing with receiver-in-canal (RIC) technology and a series of proprietary innovations to meet these requirements. This approach allows a feedback-free and occlusion-free fitting for a wide range of hearing losses (see Appendix I). Behavioral studies show that CENTRA Active also provides an outstanding spontaneous acceptance. The special acoustics and features of CENTRA Active are discussed in detail in this paper.
Each year we observe advanced technology resulting in new algorithms in digital hearing instrument signal processing. Notable recent examples of this from Siemens are e2e wireless™ technology (Powers & Burton, 2005), SoundSmoothing™ (Keidser, O'Brien, Latzel, & Convery, 2007; Chalupper & Powers, 2007) and the Learning Volume Control, referred to as "DataLearning" (Dillon et al., 2006; Chalupper & Powers, 2006). Field studies and clinical research has shown that these advancements enhance patient benefit.
In addition to innovations in signal processing, however, there also is a need for advancements that will increase patient acceptance of hearing instruments. Consumer surveys (e.g., Kochkin, 2002) indicate that many hearing aid users desire hearing instruments which are discrete, easy to use, comfortable to wear and provide overall listening comfort. It is therefore important that advancements in signal processing be combined with other innovations - for example, style and ease of use - to accommodate the other desired attributes of hearing instruments and ultimately lead to increased use and benefit.
A style and substance solution
A new hearing instrument from Siemens, CENTRA Active, combines the advanced and clinically proven signal processing strategies of the CENTRA hearing instrument family with new design and handling features to enhance cosmetics, usability, and patient wearing comfort. CENTRA Active includes the following digital signal processing features from the successful CENTRA product family:
- SoundSmoothing
- Learning Volume Control ("DataLearning")
- e2e wireless
- Automatic, multi-channel adaptive microphone directional processing
- Speech and Noise Management with Wiener Filter and modulation-based digital noise reduction (DNR)
- Fast-acting, adaptive phase cancellation feedback control
- Data logging
- Remote control option
- 16-channel compression system
Receiver-In-Canal Technology
In recent years, the behind-the-ear (BTE) open canal (OC) hearing instrument has enjoyed increased popularity. As reviewed by Mueller (2006), there are many advantages to OC fittings, and patient surveys have shown that these instruments provide improved benefit and satisfaction (Gnewikow & Moss, 2006; Taylor, 2006). One advantage of the OC fitting is in regard to cosmetics, an important concern for most consumers. With RIC BTEs, the aid itself can be relatively small since the receiver, one of the largest components, is placed outside the instrument's housing into the ear canal. This, of course, makes the hearing instrument less visible and more cosmetically appealing. The thin wire used to transfer the signal to the receiver in the ear canal is also thinner and less conspicuous than typical earmold tubing.

Figure 1. Components of the external receiver including the dome with C-Guard and the receiver housing.
CENTRA Active's RIC unit and dome are shown in Figure 1. The receiver unit consists of the receiver wire, the housing spout, the receiver, and the receiver housing all integrated into one piece that securely attaches to the instrument body with a click-and-turn connection. The CENTRA Active dome tip includes an integrated C-Guard barrier membrane. This membrane prevents even liquid cerumen from impacting the receiver (Branda & Chalupper, 2007). The C-Guard membrane is slightly recessed from the tip of the dome to prevent damage to the membrane. Domes are easily but securely attached to the receiver spout tip, so that they can be changed as needed. CENTRA Active can be fit with either open or closed earpieces. Open domes are available in three sizes (6, 8, and 10 mm) and closed domes are available in two sizes (8 and 10 mm). It is also possible to use a conventional closed earmold with the RIC technology.
CENTRA Active's receiver housing is ergonomically bent to assure easy insertion and a comfortable fit in the ear canal. In addition to comfort, the receiver housing was carefully designed so that it fits appropriately around the bend of the ear canal, and the outlet is maintained in the center of the canal. With a straight receiver housing, there is a risk that the tip may be pushed against the canal wall. In addition to discomfort, this may cause an increased risk of feedback, reduction in the amplified signal, cerumen accumulation, as well as cause the receiver to work its way out of the canal.
Acoustic advantages of RIC
In addition to the cosmetic and "ease-of-use" benefits of CENTRA Active, there also are important acoustic advantages that have been optimized in the Active design. As reviewed by Mueller (2006), improved high frequency amplification is a desired attribute of OC fittings. Mueller and Ricketts (2006) demonstrate that when the coupling in the ear canal allows for a residual ear canal resonance, this resonance then contributes to the amplified signal. That is, in the region of the residual resonance, less amplifier gain is needed to achieve the desired ear canal SPL. This residual ear canal resonance usually is in the 2000-3000 Hz range, which are important frequencies for speech understanding, especially in background noise.
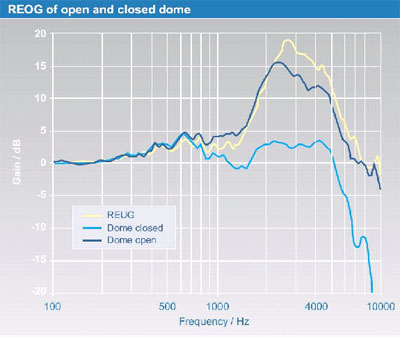
Figure 2. Illustration of the real ear occluded gain (REOG) for both the open and closed domes of CENTRA Active. The real ear unaided gain (REUG) is shown for comparison.
Figure 2 shows the real ear unaided gain (REUG) for the open ear canal. Observe that there is a 13-17 dB peak in the 2000 to 4000 Hz range. In a closed hearing aid fitting this open-ear advantage is eliminated, as the canal is closed and resonant properties are altered. However, observe in the dark blue curve of Figure 2, when the receiver fitted in the open dome is placed in the canal, all the open-ear effects remain. The curve for the closed dome shows that there is nearly no difference to the REUG below 1 kHz, but rather significant attenuation at higher frequencies. The following sections examine the consequences of these acoustic properties on occlusion and feedback stability.
In addition to improved high-frequency amplification, another desired benefit of the CENTRA Active RIC is the reduction of the occlusion effect. The occlusion effect, often described as a "hollowness" of one's own voice, is known to be bothersome, and in some instances prevents individuals from using amplification. Physically, the occlusion effect relates to an increase of sound pressure level at low frequencies inside the ear canal. While the curves shown in Figure 2 suggest that the ear canal is not significantly occluded below 1 kHz, this is not a direct measure of the "occlusion effect," as REOG is measured with an external signal.
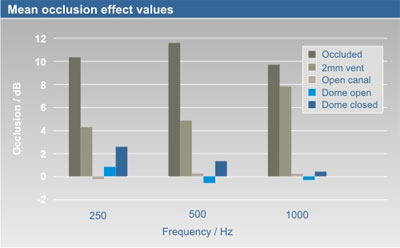
Figure 3. Occlusion measurements for CENTRA Active fitted with both the open and closed dome. Results from MacKenzie (2006) for occluded, 2mm and OC tips shown for comparison.
To confirm that CENTRA Active's ear pieces do not cause an occlusion effect, testing was conducted with ten individuals (five males and five females). Each subject was fitted with the most appropriate dome size and wire length. The amount of occlusion was measured by subtracting the level in the open ear canal from the level in the test condition (open dome, closed dome). Subjects vocalized an "ee" during the measurements to generate an "internal" test signal. The results of this testing, using the open and closed dome, are shown in Figure 3. For comparison, these mean findings are displayed with the mean data from MacKenzie (2006), which illustrate the expected amount of occlusion for an occluded fitting, an open fitting and a vented fitting (2-mm vent). Note that with CENTRA Active, negligible occlusion is present. Even with the tighter fitting closed dome, average occlusion is no more than 2-3 dB — a value that would not be bothersome nor even noticeable for most patients.
There is a direct relationship between sound quality and the smoothness of the frequency response. The receiver and coupling system of CENTRA Active were optimized to provide a smooth response with extended amplification in the higher frequencies. Figure 4 illustrates measures taken in the ear of the KEMAR for both the open and closed domes. Notice that the frequency response of Active is smooth throughout the frequency range, with high-frequency amplification extending to 8000 Hz.
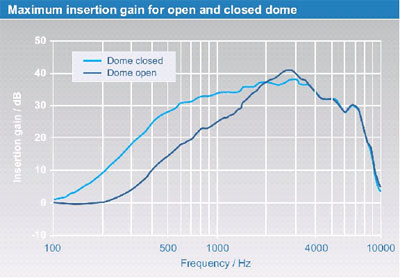
Figure 4. Measured maximum insertion gain (IG) for both the open and closed domes of CENTRA Active.
Observe that for both domes, gain in the higher frequencies is similar. Because there is less ear canal leakage with the closed dome, gain with this fitting option is 10 to 15 dB greater in the lower frequencies.
Maximum insertion gain, displayed for CENTRA Active in Figure 4, can be practically applied only if feedback is absent. To accomplish this, the maximum gain without feedback (also known as "critical gain" or "maximum stable gain") must be larger than the maximum insertion gain. A commonly used method to determine the critical gain for a given individual is an open loop gain (OLG) measurement (see Dillon, 2001 for review). The critical gain measurement in CONNEXX also applies the open loop gain technique.
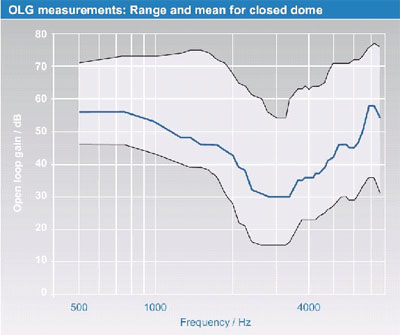
Figure 5. The mean open loop gain (OLG) for CENTRA Active (closed dome), with minimum (botttom black line), average (blue line) and maximum (top black line) values.
Figure 5 shows the range (i.e. minimum and maximum values) and mean of the critical gain measurements for 50 subjects with CENTRA Active fitted with the closed dome. Observe that there is an extremely large individual variance - up to 40 dB for some frequencies! Some patients, especially in the low frequencies, have stable gain values much larger than the maximum gain of CENTRA Active. Note that the average critical gain at 3000 Hz is about 30 dB; this is the frequency region where the SPL is typically the greatest in the ear canal, and hence the probability of feedback is greatest. The mean maximum stable gain in this region is about 10 dB below the maximum insertion gain shown in Figure 4. Due to the large individual variability, individual critical gain measurements are recommended when this instrument is fitted. Because the open dome is less occluding (see Figure 3), the average stable gain will be somewhat less at all frequencies than shown in Figure 5 for the closed dome.
With any OC fitting, the risk of feedback is higher than that of a closed fitting. This feedback risk indicates the need for an effective feedback cancellation system. CENTRA Active's feedback cancellation system provides between 10 and 20 dB additional stable gain. Factors that influence this are individual hearing loss, individual anatomy, and the acoustical situation. Since the feedback path can vary by up to 20 dB in daily life conditions (e.g. due to chewing, proximity to reflective surfaces, etc.), a combination of OLG optimization (e.g. by using OPEN) and an adaptive feedback canceller is able to provide feedback-free listening for most patients in daily life (see Appendix II).
Clinical studies
As discussed, the acoustic benefits of CENTRA Active are numerous. Therefore, whether these design attributes would translate to improved patient satisfaction was the subject of a recent study conducted at the Hörzentrum in Oldenburg, Germany (www.hoerzentrum-oldenburg.de/web_en/start/index.shtml). Twenty experienced hearing instrument wearers with moderate symmetrical hearing loss participated in the study. CENTRA Active was compared to three other premium OC hearing instruments from major manufacturers. One of the comparative products also employed RIC technology, while the other two were traditional BTE designs with the receivers located in the instrument housing.
Each of the four hearing instruments was fitted to the subjects, and ear canal recordings were made for three different sound examples: speech in quiet, speech in a background babble noise, and music (flute). These recordings were then played back-to-back to the participants using a paired-comparison paradigm. By using recordings, the participants were blinded to the products themselves, and factors such as size of the hearing instrument, comfort of the fitting, etc., were not confounding variables. In each round, all products were compared to each other, and in each comparison, the participant was instructed to pick a "winner" (the hearing instrument that they would prefer to use). In the case that two instruments sounded the same, the subject was to indicate that as well. The complete round-robin procedure was repeated two times, resulting in a total of 18 comparisons for each hearing instrument.
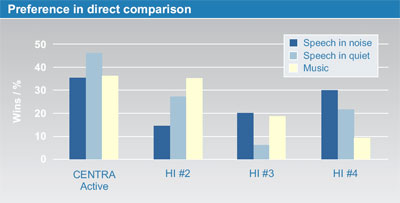
Figure 6. Percent of wins in paired comparison test for three different listening conditions. Data represents pairings where differences were noted.
The results of this research are illustrated in Figure 6. Shown are the percent of wins for each product for each listening condition. As all devices were premium products, in several of the comparisons, no difference could be detected. However, observe that when differences were noted, CENTRA Active consistently had the most wins for all three listening conditions. These findings reveal that even when compared to the highest level of competition, the signal processing and acoustics of Active have a distinct advantage.
Fitting guidelines
In general, fitting decisions and procedures concerning CENTRA Active are similar to other members of the CENTRA family. However, there are some specific issues to consider for CENTRA Active. In observing the published fitting range, it's important to consider that the upper limit of the range is calculated based on NAL-NL1, Acclimatization Level 2, with an additional 5 to10 dB headroom to allow for the peaks of speech, temporary volume control adjustments, and/or progressive hearing loss.
Programming CENTRA Active requires Siemens fitting software CONNEXX 5.4, SiFit database 5.4.2 (or higher). First Fit can be performed using the following fitting algorithms: Siemens OPEN, NAL-NL1 or DSL. The OPEN algorithm (Chalupper & Kasanmascheff, 2005) uses NAL-NL1 as the audiologic rationale to calculate input frequency-specific gain and output values. In addition, the OPEN formula automatically optimizes the frequency response if it is predicted that the NAL-NL1 output values will exceed critical gain. In most cases, because of CENTRA Active's fast-acting feedback cancellation system, the NAL-NL1 targets can be met, so the OPEN algorithm is a conservative approach to further guard against unwanted feedback.
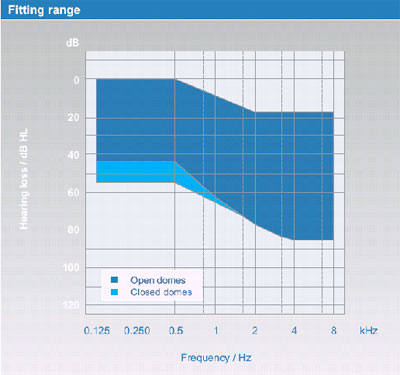
Figure 7. The shaded areas on the audiogram represent the recommended fitting range for CENTRA Active with open and closed domes.

Figure 8. Illustration of the procedure for replacing the external receiver of CENTRA Active.
Receiver Selection & Replacement
The receiver unit is available in four different wire lengths; the most appropriate length can be easily determined for each patient using the CENTRA Active measuring gauge. The receiver assembly is easy to attach and remove (see Figure 8). To remove, simply rotate the "turn-and-click" connection counter-clockwise (noticeable click). To attach, take the new receiver and then turn the connection clockwise (noticeable click). This easy process is also used to replace damaged receivers in office and eliminates the need to send out the hearing aid for receiver repair.
AquaProtect: Maintaining high reliability and function
The second major advancement in the CENTRA Active is a feature referred to as AquaProtect, which is actually the combination of three new technologies: C-Guard, which is a new cerumen protection system, a unique GORE exchangeable microphone cover, and the use of a special nanocoating. A recent study (Infratest, 2006) examining the aging population identified that almost three quarters of people over the age of fifty are participating in some form of athletic activity. Fifty percent of all golfers are over the age fifty. Recent research has revealed that with modern hearing aids such as the CENTRA Active, the average age of hearing aid users is sixty (Kochkin, 2006). If we simply consider the 60 to 70 year age bracket, there is an overwhelming majority (84%) ef people participating in activities such as hiking and bicycling (Infratest, 2006). These types of activities invite an increased exposure to moisture from the environment and quite often perspiration. It is apparent that hearing instrument technology needs to not only meet communication demands that we discussed in the previous section, but also those demands imposed by physical and outdoor activities. AquaProtect is designed to handle these lifestyle requirements.
C-Guard
A critical component of AquaProtect is C-Guard. Hearing instrument receivers are commonly exposed to both moisture and cerumen. Due to its placement in the ear canal, the receiver needs to be securely protected without a negative impact to the frequency response. Such protection requires an acoustically transparent barrier that shelters the instrument from cerumen, debris, and moisture.
The C-Guard consists of a thin membrane secured to a plastic housing that is integrated securely into the CENTRA Active dome ear tip. This membrane creates a gas-tight seal to prevent moisture and cerumen from entering the receiver. The C-Guard membrane is also effective against less dense types of cerumen that can bypass other wax protection systems. The membrane is designed with high compliance and low mass so it remains acoustically transparent. A special design in the receivers used with C-Guard involves the addition of a tiny barometric relief vent providing a consistent pressure balance on both sides of the membrane. The balance prevents expansion and shrinking of the air pressure in the receiver tube and thus inhibits added impedance on the system. With CENTRA Active the pressure balance is realized through the GORE microphone cover, discussed in the next section, which blocks water and moisture but is permeable to air.
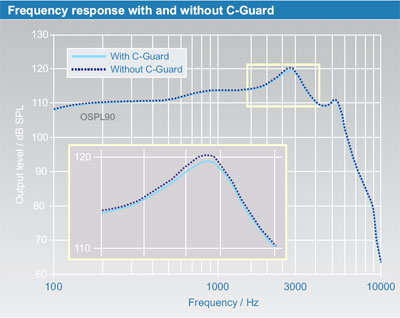
Figure 9. Frequency response with and without C-Guard.
With placement directly in the ear canal, C-Guard is directly exposed to moisture and cerumen. Over time, debris can begin to build up on the membrane. With proper cleaning (simply wiping with a clean, dry cloth), the C-Guard has been shown to function for three months or more with no diminished performance. If acoustic performance appears to be inhibited, a new C-Guard can be applied by simply changing the CENTRA Active dome. As C-Guard was designed for maximum ease of use, no special tools or cleaning methods are necessary.

Figure 10. Clip-on microphone cover.
GORE Moisture Protection
The clip-on microphone cover is an industry-first design using GORE moisture protection technology (Figure 10). Clip-on covers are not unique to CENTRA Active and AquaProtect, however, the GORE membrane sets this design apart from all others. The GORE protection mimics the nature of human skin to repel water and water vapor. This membrane is ultra thin with approximately 1.2 billion tiny pores per cm2. Water molecules are 20,000 times larger than these pores, thus, the GORE can protect against moisture without completely blocking the microphones. There is no acoustical impact of this design, even at very high frequencies, which are highly sensitive to impact from such barriers.
In addition to protecting against moisture, the clip-on cover is an excellent shield against dirt and debris. Hearing instrument microphones, because of the necessity to collect sound, are positioned on hearing instruments at locations that often are vulnerable to environmental factors. The GORE membrane prevents dirt and other debris from coming into contact with the CENTRA Active microphones.
Another benefit of the GORE membrane and the clip-on cover is the reduction of wind noise. The shearing effect of the wind grazing the microphone ports creates turbulences, vibrates the diaphragms of the microphones, and is consequently perceived as "wind noise." This can be a great disadvantage in any listening situation and is a primary concern for those hearing instrument wearers who participate in outdoor activities. The GORE membrane minimizes this effect by creating a noticeable decrease in wind noise, especially in the low frequencies where wind noise is most prevalent.
To objectively test the effectiveness of the wind noise reduction function of the clip-on microphone cover, measurements were conducted both with and without the clip-on cover in place. The instrument was exposed to a variety of wind speeds and output measures were conducted in both the uncovered and covered conditions.
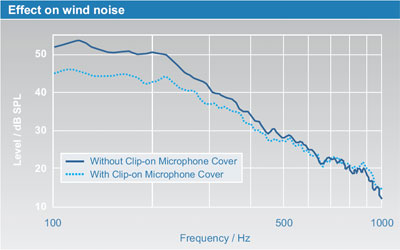
Figure 11. Wind noise reduction with clip-on microphone cover.
As shown in Figure 11, the clip-on cover reduced wind noise up to 7 dB at low frequencies, with wind speeds as slow as 15 km/h. With the added function of CENTRA Active's digital processing with wind noise reduction (eWindScreen), this is extremely effective for active hearing instrument wearers exposed to wind conditions.
Nanocoating
The third important component of AquaProtect is nanocoating. Nanotechnology involves investigating, producing and applying structures smaller than 100 nanometers (nm). A nanometer is one billionth of a meter. For a size comparison, one should consider that the width of human hair is about 80,000 nm. As an interdisciplinary process, nanotechnology can be found in the cosmetics industry, pharmaceutical industry, environmental technologies, chemistry, biology, and very recently in hearing instrument technology. An excellent technical introduction to nanotechnology has been published by Drexler (1992).
"Nano," coming from Greek for "dwarf," today is often used as a reference to things that are merely small in size but that do not incorporate actual nanotechnology as defined above. Siemens AquaProtect utilizes true nanotechnology in the form of nanocoating. The hearing instrument case undergoes a special process of using precise temperatures and application to ensure that the case is appropriately protected. Nanocoating results in a hydrophobic and oleophobic surface and also minimizes capillary action. Hydrophobic and oleophobic mean that the surface repels water and oils. Capillary action, which nanocoating minimizes, refers to the tendency of liquids to move into a narrow opening, such as pores or openings in a surface. Nanocoating is also effective at repelling dirt and debris, thereby assisting in the ease of cleaning a hearing instrument. Additionally, for extra hygienic benefit, nanocoating helps prevent microbial growth, which often occurs on the hearing instrument housing (Sturgulewski, Bankaitis, Klodd, & Haberkamp, 2006; Bankaitis et al., 2002).
Clinical Studies
To determine the effectiveness against exposure to intermittent contact with water, five CENTRA Active hearing instruments with AquaProtect were tested along with fifteen hearing instruments without AquaProtect. For a duration of 10 minutes, 0.07 liters of water per minute were focused on the hearing instruments from all sides. The test was not designed to completely immerse the instruments in water, but to simulate the type of exposure to moisture that may be encountered with perspiration due to physical activity or with exposure to rain.
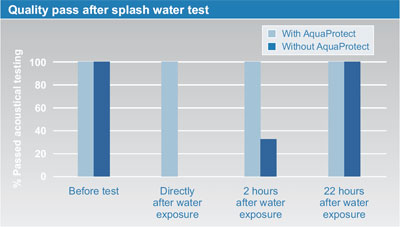
Figure 12. Results from intermittent exposure to water.
Results for this test can be observed in Figure 12. Following the exposure to the water, the instruments immediately underwent an acoustical analysis to determine functionality. All instruments without AquaProtect failed acoustic testing. All of the CENTRA Active instruments with AquaProtect passed acoustic testing. The acoustical tests were repeated two hours later and of those instruments that had previously failed, only 33% passed. It was not until 22 hours after the time of exposure to the water that all instruments passed acoustical analysis. These results indicate that hearing instruments without AquaProtect are highly susceptible to failure for two hours or more after direct contact with water, even if exposed for only brief periods of time.
In a second study, conducted by the Academisch Medisch Centrum Amsterdam (AMC), C-Guard was compared to a leading wax protection system (Boymans, Dreschler, &Veenman, 2006). Ten hearing-impaired subjects with mild sloping hearing loss wore custom hearing instruments for a period of weeks. All participants were fitted bilaterally. One side was equipped with C-Guard and the other side used the alternative wax protection. At the end of the trial, subjects were asked which system they preferred regarding various aspects like problems with moisture (sweat, humidity, rain, etc) and ear wax, feedback and frequency of battery and filter changes. On average, subjects reported to have mild to moderate problems with ear wax, with two of them having no problems at all and two with severe problems.
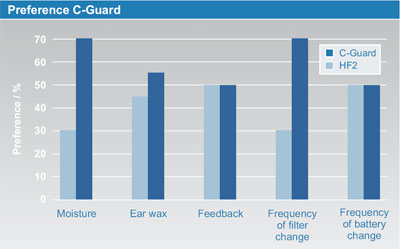
Figure 13. Preference for C-Guard when compared to a conventional wax protection system.
Subjects reported a significant reduction in moisture problems with the C-Guard. Importantly for ease of use, subjects reported that C-Guard was easier and required fewer changes. This is illustrated in Figure 13, which shows a clear preference for C-Guard with regard to moisture and frequency of filter changes. As expected, for subjects with small ear wax problems there is only a small advantage of the C-Guard compared to conventional systems, as most wax systems perform fairly well at blocking dense, thick cerumen. Not surprisingly, there is no difference between wax systems regarding feedback and battery lifetime. Additional objective measurements of acoustic performance verified that the C-Guard was acoustically transparent (see also Figure 9).
Another recent study was designed to evaluate the ease and effectiveness of the C-Guard system (Branda & Chalupper, 2007). Fourteen clinics in Germany and ten in France provided C-Guard to patients known to have prior hearing instrument repair issues related to wax and/or moisture. This field trial consisted of three visits. The first visit involved providing the system to the hearing instrument wearer and giving him or her instructions on how to clean and replace the C-Guard. The second visit was at the three-week follow-up timeframe where the C-Guard membrane was inspected and the subject was asked to complete a questionnaire. The final visit occurred after either six weeks or the first change of the C-Guard by the subject, whichever came first. In this final visit, the subject was again asked to complete another questionnaire. In total, C-Guard was provided to 75 subjects and placed on 116 custom hearing instruments. The mean subject age was 70 years with a range from 59 to 84. Half of the subjects were previous wearers of hearing instruments. The other half were first-time wearers, although some had previously attempted and rejected hearing instruments due to wax-related issues.
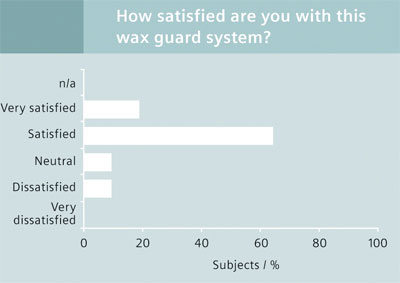
Figure 14. Patient satisfaction with C-Guard.
As shown in Figure 14, the benefit of C-Guard is clearly reflected in the satisfaction ratings of the patients. More than 60% were "satisfied;" 18% were "very satisfied." Importantly, 100% of the patients stated that they would recommend the C-Guard to others.
Innovative Rechargeable Battery
The third major advancement introduced in the CENTRA Active is the rechargeable battery. It is well known that hearing aid batteries are an area where hearing instrument wearers are seeking improvement. Reports indicate that factors such as costs associated with batteries, ease of use, and battery life are long-standing concerns for the hearing instrument wearer (Kochkin, 2002). A rechargeable battery can help address these concerns.
Requirements for rechargeable batteries
To investigate the issues surrounding rechargeable hearing aid batteries, studies were conducted by independent market research institutes in the USA, France and Germany (Wessner, Schindhelm, & Heyder, 2005). The institutes, using a group discussion format, met with forty-eight experienced hearing instrument wearers, forty-eight future hearing instrument wearers, and thirty-two hearing care professionals in sixteen group sessions.
The results of these focus group sessions revealed several advantages concerning the rechargeable battery concept. The hearing aid users reported less handling/replacement difficulties, no need to locate source of new batteries, and other economic and environmental advantages. The professionals reported that there would be less involvement in ordering and stocking batteries, and that hearing aids would be viewed as "more modern" if they had rechargeable batteries.
There also were a few potential disadvantages identified by the research. An obvious concern was battery life and recharging time, as these factors will affect daily hearing instrument use. Another concern identified related to alternate power supplies and options when the hearing aid wearer forgets or is unable to recharge a battery. These advantages and disadvantages were discussed and weighed in the focus groups to identify preferences and requirements for a rechargeable option, which all groups preferred. These results were then used in developing the rechargeable system for the CENTRA Active.
Long-Lasting Battery
It is critical that the rechargeable battery be long lasting. Two main options available for battery technology were the nickel-cadmium (NiCd) cell and a nickel-metal hydride (NiMH) cell. The NiCd cell was determined to not be as environmentally friendly, and also had a memory effect which could potentially decrease daily longevity of the battery. Memory effect refers to the fact that with some rechargeable systems, performance time is based on "memory" of previous time durations prior to being recharged. With batteries that have a memory effect, over time, a battery that was typically recharged while still at half capacity may lose capacity and not last as long as an identical battery that was consistently exhausted before being recharged.
The NiMH battery was determined to be a better option for the rechargeable hearing instrument. NiMH provides approximately double the power per package as compared to NiCd. Additionally, NiMH batteries do not contain any dangerous heavy metals like mercury, lead or cadmium and are therefore more environmentally friendly.
Battery Size and Capacity
Along with choosing the appropriate battery technology, battery size must be considered in designing the optimum rechargeable solution. The 675 sized cell had been used in prior rechargeable options, however, current cosmetic demands dictate that a smaller cell size is required. Advancements with NiMH battery technology provide improved power levels in smaller sizes of 10, 312, and 13 cells that were not previously available. The primary goal with a rechargeable battery is to achieve a full day's use at minimum. The commonly used zinc air batteries of course have a higher capacity than rechargeable batteries. This comparison, however, is not appropriate for the rechargeable battery, which needs to power a hearing instrument for a full day and then charge overnight.
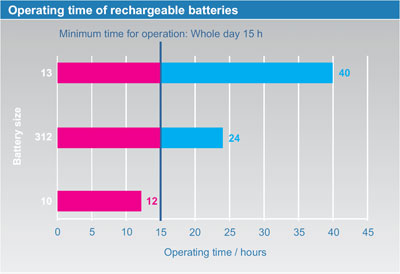
Figure 15. Battery operating time (linear, all adaptive signal processing switched off).
As mentioned, in choosing the appropriate size for the rechargeable battery, the minimal standard is that the battery needs to operate for at least one full day. However, as this must be guaranteed for all hearing instrument wearers, in this case one full day could mean operation up to 15 hours! Figure 15 shows operating time in hours for three sizes of batteries according to current measurement standards (linear settings, adaptive parameters off). One can see from the displayed usage hours that a size 10 battery does not have the capacity to operate the hearing instrument for a full day and is therefore not a reasonable option for selecting an appropriate battery size.
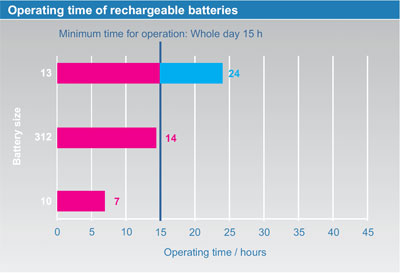
Figure 16. Realistic battery operating time (all signal processing activated).
When comparing the size 13 and size 312 batteries more closely, it is important to consider the effects on the battery when other aspects of digital processing, such as digital noise reduction, are activated. One can expect a higher demand on the battery due to the increased processing. Therefore, the hours indicated in Figure 15 must be modified to take into account these extra demands. Figure 16 provides a more realistic expectation of operation time from the battery with full functionality of the features of a typical digital hearing instrument. From this chart, it can be seen that a 312 size battery will not provide a long enough operating time for a full day. It is therefore concluded that the practical battery size to achieve cosmetic acceptance and appropriate use time is the 13 size NiMH battery.
Discharge Behavior
Another factor to consider with a battery cell is the discharge behavior. Discharge behavior refers to the rate and transition from full battery capacity to the cutoff voltage where it ceases to supply power. The discharge with the NiMH rechargeable battery is very smooth and consistent, similar to the zinc air battery.
Temperature Effects
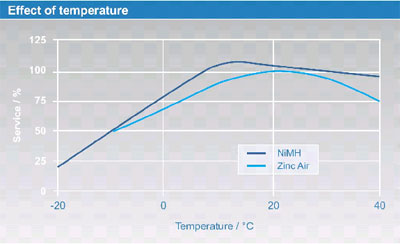
Figure 17. Effect of temperature on NiMH and zinc air batteries.
As shown in Figure 3, NiMH cells work at temperatures from -20 to +40 degrees Celsius (-4 to +104 degrees Fahrenheit). However, at very low temperatures, battery lifetime may decrease to 25% of the nominal value at room temperature. For comparison, zinc air batteries operate from -10 to +40 degrees Celsius (+14 to +104 degrees Fahrenheit) and also are less efficient at very low temperatures than at room temperature. As a rule of thumb, NiMH batteries show a similar behavior as zinc air cells - apart from being rechargeable.
Easy and Effortless Recharging
With the selection of the rechargeable size 13 NiMH battery, the next important requirement to address is that of recharging. As indicated by the market research discussion groups, recharging needs to be an easy and effortless process. Factors such as use of monaural versus binaural hearing instruments, dexterity concerns, and efficient charging times contribute to determining what is "comfortable and acceptable" for a given hearing instrument wearer.
CENTRA Active Charger

Figure 18. Charger with hearing instruments.
The rechargeable system designed by Siemens for CENTRA Active incorporates many advantages for the hearing instrument wearer in an intelligent and efficient package. Charging is performed in a compact charger unit that, with the addition of a small silica gel pillow, can also dry the hearing instruments while the batteries are charging. The unit is capable of charging two instruments simultaneously. The instruments are simply placed inside the charging cavities in the charger (Figure 18). The hearing instrument battery doors do not need to be opened, nor do the batteries need to be removed. This is important to support ease of handling. When the instruments are detected, the charger will turn the hearing instruments off automatically to eliminate any risk of feedback while charging. At this point, lights on the charger will indicate that charging is progressing normally or if there are any problems with the charging process (Figure 19).
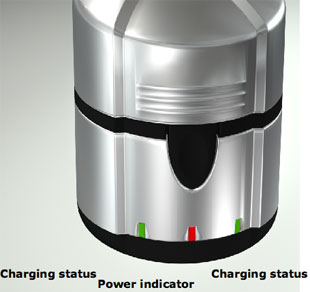
Figure 19. Indication of charging status.
When normal charging is occurring, the green status light will blink to indicate the charging process. If the charger detects a non-rechargeable battery, a defective battery, or batteries with reversed polarity, it will alert the hearing instrument wearer with a steady orange charging status light and will not attempt to charge the batteries. As discussed, the battery can last for an entire day and evening before recharging is required. Additionally, as NiMH batteries have no memory effect, there is no negative impact on daily use by recharging a battery that is not fully discharged. The charging process itself with CENTRA Active only takes five hours.
Multi-Stage Charging
In addition to ease of handling, the optimum rechargeable solution must avoid overcharging and also maintain a high number of recharge cycles. In contrast to inexpensive pen chargers, the Siemens charger uses a microprocessor controlled multi-stage procedure which varies the charging current as a function of the on-going charge of the battery. In the beginning, a very high charging current is applied to ensure optimum charging speed. Approaching the complete charge of the battery, the charging current is reduced stepwise to avoid overcharging. Thus, both optimum speed and high safety are achieved. At the conclusion of charging, the charger will indicate that the batteries are fully charged with a steady green charging status light.
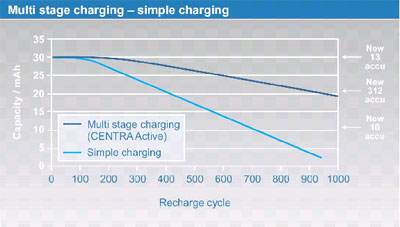
Figure 20. Number of recharge cycles.
With the Siemens charger, a NiMH battery can be recharged about 300 times without significant degradation of capacity (see Figure 20). After more than 300 charging cycles the charging capacity decreases gradually and typically approaches the capacity of a 312 NiMH after about 1000 cycles - a capacity which often is not sufficient for one full day of operation. That means that the Siemens rechargeable battery system (i.e. Siemens charger in combination with Siemens battery) allows one single battery to be used between 500 and 1000 times. Figure 6 also shows that with other charging procedures, the battery lifetime is likely to be less than 500 recharge cycles.
Summary
Research and anecdotal evidence alike indicate that hearing instrument wearers desire hearing instruments that are discrete, easy to use, comfortable to wear, provide overall listening comfort, and perform in a variety of acoustic environments. Research also indicates that these patients receive significant benefit from the latest algorithms and special features available with modern hearing instruments. The goal, therefore, when a new product is introduced, is to couple the new advanced algorithms with new appealing hearing aid designs as well as ergonomic advances. CENTRA Active meets this goal by accommodating all these desired attributes and more.
Using the latest RIC technology, this innovative product provides a wide range of gain and output, a smooth extended frequency response, and an occlusion-free fitting. Innovations in handling, robustness, and design have also been achieved. Moreover, clinical trial results have supported patient's preference of CENTRA Active over other premium solutions. In summary, CENTRA Active meets the requirements of a wide range of patients, and its design and features are expected to further enhance patient benefit and satisfaction.
References
Bankaitis, A.U. (2002). What is growing on your patient's hearing aids? The Hearing Journal, 55(6), 48-56.
Boymans, M., Dreschler, W.A., & Veenman, J. (2006). Testing a wax-protection foil for receivers in ITE hearing aids. Unpublished study report.
Branda, E., & Chalupper, J. (2007). An efficient and effective method to protect hearing aids against moisture and cerumen. The Hearing Review, 14(3), 56-89.
Chalupper, J., & Kasanmascheff, R. (2005). Using psychoacoustic models for fitting ski-slope hearing losses. In Rasmussen, Poulsen, Andersen, Simonsen, Larsen, Holmen Center Tryk, & Kolding (Eds.), Hearing Aid Fitting - Proceedings of 21st Danavox Symposium, (pp. 619-630). Denmark.
Chalupper, J., & Powers, T. A. (2006). Changing how gain is selected: The benefits of combining datalogging and a learning VC. The Hearing Review, 13(13), 46-55.
Chalupper, J., & Powers, T. A. (2007). New algorithm is designed to take the annoyance out of noise. The Hearing Journal, 60(4), 42-48.
Dillon, H. (2001). Hearing instruments. New York: Thieme.
Dillon, H., Zakis, J. A., McDermott, H., Keidser, G., Dreschler, W., & Convery, E. (2006). The trainable hearing aid: What will it do for clients and clinicians? The Hearing Journal, 59(4), 31-36.
Drexler, K. E. (1992). Nanosystems: molecular machinery, manufacturing, and computation. Hoboken, NJ: Wiley.
Gnewikow, D., & Moss, M. (2006). Hearing aid outcomes with open and closed canal fittings. The Hearing Journal, 59(11), 66-72.
Infratest. (2006). Best-Ager-Studie. DBV Winterthur: Wiesbaden.
Keidser, G., O'Brien, A., Latzel, M., & Convery, E. (2007). Evaluation of a noise reduction algorithm that targets non-speech transient sounds. The Hearing Journal, 60(1), 29-39.
Kochkin, S. (2002). MarkeTrak VI: Consumers rate improvements sought in hearing instruments. The Hearing Review, 9(11), 18-22.
Kochkin, S. (2006). BHI survey looks at thin-tube/open-Fit BTEs. The Hearing Review, 13(10). Retrieved September 22, 2007, from www.hearingreview.com/issues/articles/2006-10_03.asp
MacKenzie, D. (2006). Open-canal fittings and the hearing aid occlusion effect. The Hearing Journal, 59(11), 50-56.
Mueller, H. G. (2006). Open is in. The Hearing Journal, 59(11), 11-14.
Mueller, H. G., & Ricketts, T. (2006). Open-canal fittings: Ten take-home tips. The Hearing Journal, 59,(11), 24-39.
Powers, T. A., & Burton, P. (2005). Wireless technology designed to provide true binaural amplification. The Hearing Journal, 58(1), 25-34.
Sturgulewski, S., Bankaitis, A. U., Klodd, D.L., & Haberkamp, T. (2006). What's still growing on your patients' hearing aids? The Hearing Journal, 59(9), 45-48.
Taylor, B. (2006). Real-world satisfaction and benefit with open-canal fittings. The Hearing Journal, 59(11), 74-82.
Wessner, K., Schindhelm R., & Heyder, T. (2005). Multi-national focus group study on rechargeable hearing aids. Unpublished manuscript.
Appendix I. Acoustics of RIC and conventional BTE systems
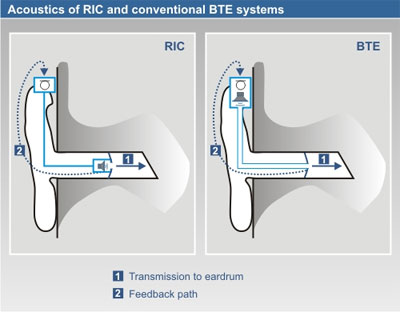
Figure A. Illustration of the sound transmission paths for the RIC and a conventional BTE, showing both the transmission of the amplified sounds to the eardrum (REAR) and also the path of the sound back to the hearing aid microphone (feedback path).
The RIC design most obviously differs from traditional BTEs because of the receiver location in the ear canal. However, the schematic drawings in Figure A show that the acoustic sound transmission paths to the ear drum and to the hearing instrument's microphone are very similar for traditional BTEs and receiver-in-canal instruments. Because of this similarity, the probability of acoustic feedback with a receiver-in-canal instrument as compared to a traditional BTE will also be similar. Factors that influence the occurrence of feedback include the intensity of the input signal, the intensity of the amplified signal in the ear canal, individual anatomy of the ear canal and outer ear, the openness of the fitting, and the location of the hearing aid microphone. As shown in Figure A, all of these contributing factors are essentially the same for hearing instruments with an external receiver and for traditional BTEs using the same earmold and microphone location. Similar considerations apply for the sound pressure level delivered to the eardrum.
Appendix II. Open loop gain (OLG) measurement
To understand the OLG technique, refer back to Figure A. This illustration shows that the sound travels through the hearing aid to the receiver and after it is delivered in the ear canal, a portion of the sound leaks back to the microphone and is picked up again. It is possible, therefore, to think of sound as a "closed loop" (from microphone to microphone) for all types of hearing instruments. When the OLG testing is conducted, however, the hearing aid signal processing path is split between microphone and receiver. That is, the microphone signal is not forwarded to the receiver. Hence, the loop is opened, which is why it is referred to as an "open loop" measure.
Now imagine what happens in the "closed loop" if there is no attenuation of the sound that leaves the receiver. As soon as any amount of gain is applied, the sound will be amplified by this amount in each run through the closed loop. Because of the speed of sound, this continuous looping effect quickly drives the gain to the maximum output of the hearing instrument. If there is a dominant frequency, there will be a whistle, or what has come to be known as feedback.
Given this knowledge of the physics of sound, it becomes clear that the amount of attenuation in the feedback path directly indicates how much gain can be applied without feedback. Hence, if we simply measure the attenuation between the ear canal SPL and the microphone, we know the maximum stable gain; this in fact is the OLG measurement. For example, if a tone was generated with a known output of 80 dB SPL and the microphone picks up this tone via the feedback path and measures its level to be 10 dB SPL, then the maximum stable gain would be 70 dB at this frequency. It is important to understand that this value is unrelated to the maximum gain provided by the hearing aid used to conduct the measurement. It simply indicates the maximum stable gain that potentially could be delivered, given the ear acoustics, earmold plumbing, and the microphone location of that particular fitting.


