Introduction
Understanding why individuals with hearing loss decide to adopt—or delay adopting—hearing aid technology is critical for improving clinical outcomes. The decision-making process is complex and is influenced by a multitude of factors extending beyond the pure audiological findings. This course explores recent research into the contextual, intra-personal, and interpersonal variables that shape a patient's readiness and commitment to hearing rehabilitation. By adopting a whole-person perspective that considers a patient's self-perception, social world, and emotional state, clinicians can better guide patients toward successful hearing aid adoption.
Learning Objectives
As a result of this course, participants will be able to:
- Identify how some contextual variables influence hearing aid adoption
- Identify how some intra-personal variables influence hearing aid adoption
- Identify how some interpersonal variables influence hearing aid adoption
What Does "Hearing Aid Adoption" Mean?
In the context of hearing healthcare, hearing aid adoption refers to the process where an individual with hearing loss decides to purchase and commit to using hearing aids as part of their treatment and rehabilitation. This process is often protracted; data suggests that, on average, it takes approximately nine years from the time a patient first suspects a hearing loss to the time they actually adopt hearing aids.
Researchers and clinicians are constantly striving to identify the factors that contribute to this "tipping point," pushing a patient toward adoption versus deciding it is not the right time for them. Understanding these drivers is essential for developing effective clinical strategies.
Theoretical Approaches to Understanding Hearing Aid Adoption
Behavioral science offers two key frameworks for understanding the patient journey toward hearing aid adoption:
Health Belief Model: This model suggests that a person's readiness to take preventive health action (like adopting hearing aids) is influenced by their perception of the problem. Key components include perceived susceptibility (risk of having hearing loss) and perceived severity (seriousness of the condition), which combine to form a Perceived Threat. This threat, combined with perceived benefits and barriers, and external Cues to Action, ultimately influences whether the patient performs the Preventive Health Behavior (adopting hearing aids).

Figure 1. Theoretical Approaches to Understanding Hearing Aid Adoption
Stages of Change Model: This model views behavioral change as a cycle, suggesting patients move through distinct phases, including pre-contemplation, contemplation, preparation, action, and maintenance. Patients may also experience relapse, but ideally enter an upward spiral where they learn from each setback. In the context of hearing aids, patients may spend significant time contemplating the decision and preparing to take action before committing to purchase and consistent use.
What Drives Hearing Aid Adoption?
It is often expected that the greater the degree of objective hearing loss measured on the audiogram, the higher the rate of hearing aid adoption should be. However, research indicates that this correlation is not as strong as clinicians might anticipate.
A study by Kochkin (2009) and others (Gopinath et al., 2011; Chien & Lin, 2012) demonstrated that the relationship between the degree of hearing loss and the hearing aid adoption rate is relatively shallow. While adoption does increase with severity, the overall adoption rate remains low despite the degree of hearing loss a patient is dealing with. This key finding underscores that objective hearing loss does not fully predict hearing aid adoption.

Figure 2. Graph of HA Adoption Rate vs. Degree of Hearing Loss
And the winner is...self-perceived hearing ability
If objective loss is a weak predictor, what is the strongest factor? Research, including a notable study by Palmer et al. (1999) and a follow-up by Sawyer, Dawes, Singh, & Munro (in press), points to self-perceived hearing ability as the single best predictor of hearing aid adoption.
In the Palmer et al. study, patients were asked to rate their overall hearing ability on a scale of 1 to 10, with 1 being the worst and 10 being the best. The patients’ self-rating was highly predictive of their subsequent decision to pursue amplification:
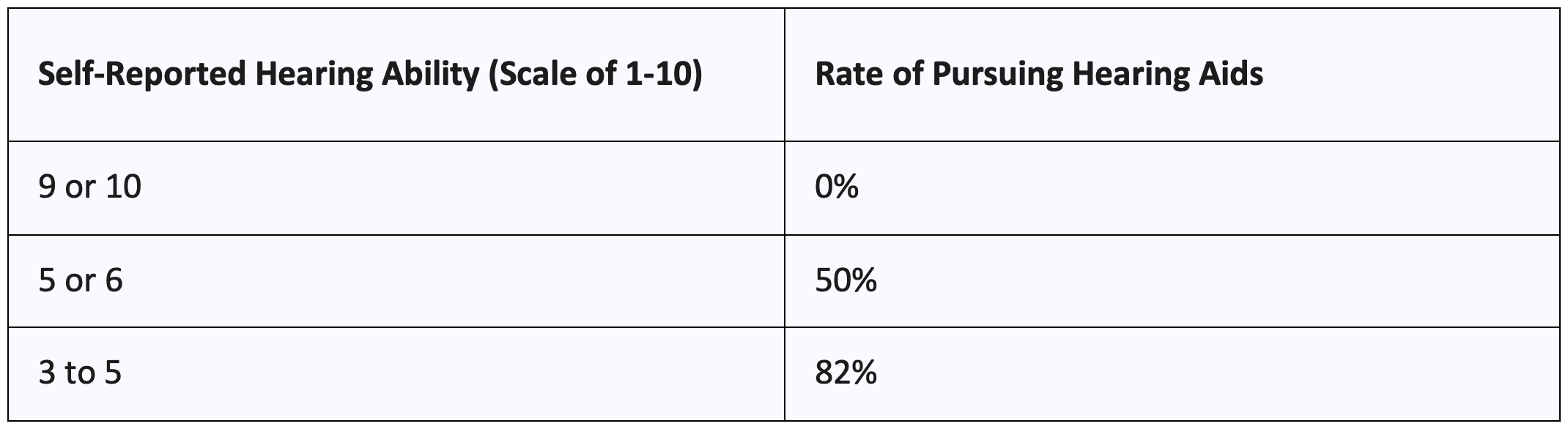
Figure 3. Self reported Hearing Ability vs Rate of Pursuing Hearing Aids
This was found to be true regardless of what the patient’s actual audiogram showed. The patient's subjective feeling about their own hearing disability drives their readiness to adopt.
Clinical Takeaways
Clinicians can easily assess a patient’s readiness for adoption by incorporating a simple self-rating question into their case history forms or initial interview: “On a scale of 1 to 10, with 1 being the worst and 10 being the best, how would you rate your overall hearing ability?”
If a patient rates their hearing ability as a 5 or 6 out of 10 or below, the clinical data suggests they are much more likely to be ready to adopt a hearing aid. This simple metric can help the provider gauge where the patient is in their hearing journey and how to frame the subsequent consultation.
The Role of Social Relationships in Hearing Aid Adoption
Humans are a pack species; relationships are critical to overall well-being and greatly influence our attitudes, beliefs, and decision-making processes. For patients navigating a decision as significant as hearing aid adoption, the influence of their social network is profound.
Why Study Social Relationships?
The importance of social connections extends well beyond decision-making. A meta-analytic review on social relationships and mortality risk found that social integration and strong social support were the biggest predictors of long-term well-being and reduced mortality, even more so than factors like smoking status, BMI, and alcohol consumption (Holt-Lunstad et al., 2010).
In the clinical setting, significant others play several roles:
- Informing Decision-Making: The decision to pursue hearing aids impacts the entire family, not just the individual patient. Significant others often help the patient weigh the pros and cons.
- Influencing the Patient’s Experience: A loved one's support and validation can significantly affect the patient's motivation and success with the rehabilitation process.
- Clinical Support: It matters who sits by the patient in clinical appointments and supports them through the process.
Hearing Loss and Third-Party Disability
Hearing loss affects a spouse's social-emotional health, a phenomenon known as third-party disability—disability experienced by family members due to a loved one’s health condition (Scarinci et al., 2012). A study on spouses of older people with hearing impairment found that 98% of the spouses reported at least a mild disability, manifesting as:
- Less involvement in social activities
- Greater loneliness
- Less engaged social participation
- Smaller social networks
- Less intimate spousal relationships
- Miscommunication during medical care
This indicates that when a loved one accompanies the patient to an appointment, they are often dealing with their own level of impact, which can be a powerful motivator for both parties to seek treatment.
The Role of Others in Hearing Aid Adoption
The mere presence of a significant other in the consultation room has been shown to influence adoption rates. A study of 60,964 patients found that hearing aid adoption was 63.8% when a significant other was present, compared to 50.6% when the patient attended the appointment alone (Singh & Launer, 2016).
This positive effect was most pronounced in patients with mild hearing loss:
- Mild Hearing Loss: The adoption rate was 96% higher when a significant other was present, compared to the adoption rate of those who came alone (72% vs 37%).
- Moderate/Greater Hearing Loss: While a significant other still provided a benefit, the difference in adoption rate was smaller, suggesting that greater severity of loss may intrinsically motivate the patient regardless of accompaniment.
For patients who are “on the fence,” particularly those with mild loss who may question the necessity of amplification, the validation and support of a loved one can be the decisive factor.

Figure 4. The Role of Others in Hearing Aid Adoption
Family-Centered Care Increases Patient Satisfaction
Beyond simply having a family member present, actively practicing Family-Centered Care (FCC) has been proven to increase patient satisfaction and adoption. A feasibility intervention study by Ekberg et al. (2022) measured patient satisfaction using the Net Promoter Score (NPS) across three conditions:
- Standard Care: No special protocols for family inclusion.
- Intervention I (External Inclusion): Staff was trained to ask a family member to attend all booking calls and reminder/confirmation communications.
- Intervention II (Internal Inclusion): Intervention I plus training staff to set up the room to include family members and setting an agenda that included both the patient and the family member.
The study found a dramatic increase in satisfaction (NPS) as family inclusion became more intentional:
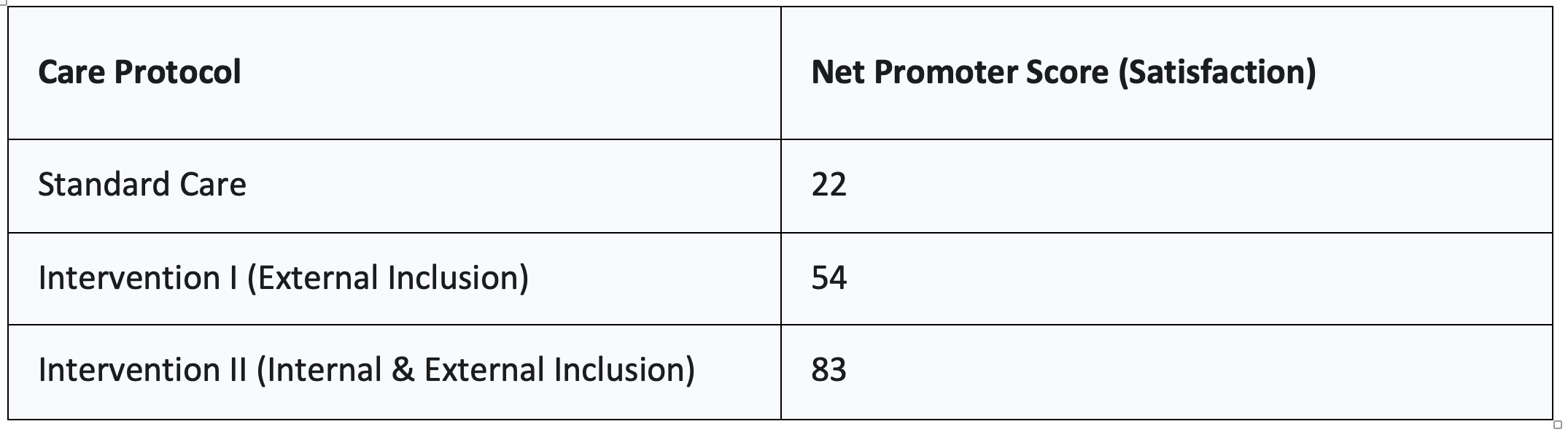
Figure 5. Care Protocol vs. Net Promoter Score (Satisfaction)
Clinical Takeaways
To foster a family-centered approach, consider the following:
- Proactively Invite Loved Ones: Always ask patients to bring a loved one to the consultation appointment. This is particularly crucial for those with milder hearing loss.
- Involve the Whole Office: Train all office staff to welcome the loved one and include them in the process, from booking to the final consultation.
- Incorporate the Loved One: Find ways to involve the loved one beyond just their presence. This can include demonstrating care and maintenance, or having them step outside during a hearing aid demo to experience the change in communication.
- Structure the Environment: Create a physical setting in the consultation room—such as a round table—where the patient, the loved one, and the clinician can sit together comfortably as a team.
The Role of Emotion in Hearing Rehabilitation
Emotion is a core mechanism by which humans interpret experience and is critical to social communication. While hearing aids process and amplify sound, the emotional experience of hearing loss and its subsequent treatment is a major, yet often overlooked, factor in the adoption process.
The quote from Joseph LeDoux (1996) states, "One of the most significant things ever said about emotion may be that everyone knows what it is until they are asked to define it." This ambiguity can make emotion difficult to address in a clinical setting, but ignoring it can inhibit rehabilitation success.
Hearing loss can be an emotional experience, bringing frustration, anger, and sadness. Furthermore, emotion has profound implications for decision-making.
The Impact of Emotion on Hearing Aid Adoption
Literature indicates that emotional readiness is strongly linked to hearing aid uptake.
A study by Grenness et al. (2015) analyzed 63 video-recorded initial audiology consultations. They found that:
- Emotional concerns were rarely addressed during the consultations.
- Audiologists often felt discomfort or were unsure how to handle the emotional side of hearing care.
- This lack of emotional engagement contributed to low hearing aid uptake, even when amplification was recommended.
Following this, Singh et al. (2017) explicitly investigated whether conversations about emotion facilitate hearing aid adoption. Participants were randomly assigned to complete one of two questionnaires in the waiting room, which were then used as a prompt for discussion:
- EMO-CHEQ (Emotions): Prompted discussion about the emotional experience of hearing loss.
- ECHO (HA Expectations): Prompted discussion about potential hearing aid ownership and expectations.
Clinicians rated their perceived comfort level with the conversation. The results demonstrated a clear trend:
The findings showed that while the HA Expectations condition (ECHO) remained relatively flat across all comfort levels, the EMO-CHEQ (Emotions) condition showed a strong positive correlation:
- When conversations about emotion were comfortable, hearing aid adoption increased significantly.
- When conversations were uncomfortable, patients tended to retreat, and the adoption rate was lower.
Clinical Takeaways
The key takeaway is that emotional readiness matters. Patients who are comfortable discussing their feelings with their provider are more likely to adopt hearing aids.
- Emphasize a Patient-Centered Approach: Build rapport and create a safe space for emotional sharing.
- Integrate Emotional Probing: In clinical interviewing, intentionally include questions that probe a patient's emotional experiences, such as:
- “How are you feeling about your hearing loss today?”
- “How has your hearing been impacting your emotional well-being?”
- “What are your deepest concerns about starting this process?”
By opening this conversation, the clinician facilitates the patient's emotional processing, which can lead directly to higher adoption rates.
What Influences Decision-Making?
The decision to pursue a hearing aid is a risk proposition for many patients, who weigh the high cost and the uncertainty of success (efficacy, cosmetics, trust) against the potential benefits. Biases, which cannot always be consciously controlled or explained by the patient, also affect this decision.
Physiological State and Risk-Aversion
Research has shown that even a patient’s basic physiological state—such as hunger or glucose level—can influence their decision-making and risk tolerance:
- Hunger and Decision-Making: A study from the Netherlands suggested that being hungry might be linked to more cautious, advantageous decision-making, possibly rooted in the evolutionary behavior of taking fewer risks when resources are scarce (de Ridder et al., 2014).
- Glucose and Risk: Conversely, another study found that increased glucose levels could increase risky behaviors in individuals with low self-control (Pfundmair et al., 2017).
The overall insight is that our body systems influence our cognitive load and risk tolerance, which in turn affects the complex decision to adopt hearing aids.
Time of Day and Hearing Aid Adoption Rates
Singh and Launer (2018) conducted a large retrospective study analyzing 24,842 first-time patient records to investigate whether appointment time impacted hearing aid adoption and return rates.
- Adoption Rate Dips: They observed that hearing aid adoption dropped significantly at 12:00 PM (Noon) and 4:00 PM compared to other times of the day. They suggested that patients who are "on the fence" are less likely to adopt during these times.
- Return Rate Dips: Interestingly, return rates also dipped at Noon and 4:00 PM. The researchers theorized that decisions made under higher cognitive load (perhaps associated with hunger/glucose dips, or end-of-day fatigue) might reflect a stronger commitment once the decision is made.
- International Consistency: A review of over 10,000 appointments in Belgium showed a similar trend, confirming the pattern was not unique to North America, though the dips were slightly delayed.
Clinical Takeaways
Clinicians can use this insight to optimize their scheduling:
- Prioritize Consultations: Schedule initial, high-stakes hearing aid evaluations and consultations earlier in the day to improve adoption rates.
- Recognize Fatigue: Avoid Noon and late afternoon time slots for patients who are likely to be "on the fence" and may be experiencing decision fatigue.
What about price unbundling?
Recent data suggests that the clinic's service model may also influence adoption rates. Picou et al. (2024) studied adult patients with no prior hearing aid experience who completed a hearing aid consultation.
They found that when services were unbundled (consultation fees charged separately), a higher percentage of patients adopted hearing aids. The authors concluded that unbundling and charging for consultations resulted in more efficient appointments and less time spent with patients who did not have the perceived hearing difficulty necessary for high adoption readiness.
This finding links back directly to the concept of self-perceived hearing ability: patients willing to pay a consultation fee are likely already at a higher stage of readiness, making the subsequent adoption more efficient.
Summary
Hearing aid adoption remains a challenge, but moving toward a whole-person perspective can significantly improve clinical success.
- Predictors: While objective hearing loss is a predictor of need, self-perceived hearing ability is the strongest predictor of adoption. Clinicians should use simple tools to assess this readiness.
- Social World: Adopting a family-centered approach that involves loved ones in the decision and care process increases patient satisfaction and adoption rates, especially for patients with milder hearing loss.
- Emotional World: Recognizing and addressing the patient's emotional experience of hearing loss, and creating a comfortable environment for this discussion, significantly drives higher adoption.
- Cognitive Processes: Contextual factors such as time of day influence risk tolerance and decision-making, suggesting that scheduling optimization can support adoption efforts.
By consciously considering the patient's social world, emotional state, and cognitive context alongside their audiological results, hearing care providers can foster a true partnership that increases the likelihood of successful hearing rehabilitation.
References
Chien, W., & Lin, F. R. (2012). Prevalence of hearing aid use among older adults with hearing loss: The National Health and Nutrition Examination Survey (NHANES), 2005–2010. Archives of Internal Medicine, 172(9), 743–745.
de Ridder, D., Kroese, F., Adriaanse, M., & Evers, C. (2014). Always gamble on an empty stomach: Hunger is associated with advantageous decision making. PLOS ONE, 9(10), e111081.
Ekberg, K., Timmer, B., Francis, A., & Hickson, L. (2022). Improving the implementation of family-centred care in adult audiology appointments: A feasibility intervention study. International Journal of Audiology, 61(12), 990–999.
Gopinath, B., McMahon, C. M., Burlutsky, G., Mitchell, P., & Wang, J. J. (2011). Hearing impairment and the prevalence of hearing aid use in older Australians. Annals of Epidemiology, 21(9), 698–701.
Grenness, C., Hickson, L., Laplante-Lévesque, A., & Davidson, B. (2015). The influence of emotion in initial audiology consultations for older adults. Journal of the American Academy of Audiology, 26(6), 565–574.
Holt-Lunstad, J., Smith, T. B., & Layton, J. B. (2010). Social relationships and mortality risk: A meta-analytic review. PLOS Medicine, 7(7), e1000316.
Kochkin, S. (2009). MarkeTrak VIII: The high price of low hearing aid adoption rates. Hearing Review, 16(5), 10–18.
LeDoux, J. (1996). The emotional brain: The mysterious underpinnings of emotional life. Simon and Schuster.
Palmer, C. V., Yu, K., & Lindley, G. (1999). The effects of hearing aid recommendations on hearing aid purchases. Journal of the American Academy of Audiology, 10(10), 578–585.
Pfundmair, M., Lermer, E., & Frey, D. (2017). Glucose increases risky behavior and attitudes in people low in self-control: A pilot study. Social Psychology, 48(1), 47–53.
Picou, E. M., Wiacek, R., Ricketts, T. A., & Roberts, R. A. (2024). Hearing aid adoption rates among adults without hearing aid experience in an audiology clinic before and after price unbundling. International Journal of Audiology, 63(1), 1–10.
Sawyer, M., Dawes, P., Singh, G., & Munro, K. J. (in press). Self-reported hearing difficulty is the single best predictor of hearing aid adoption. Ear and Hearing.
Scarinci, N., Worrall, L., & Hickson, L. (2012). Factors associated with third-party disability in spouses of older people with hearing impairment. Ear and Hearing, 33(6), 698–708.
Singh, G., & Launer, S. (2016). Social context and hearing aid adoption. Trends in Hearing, 20, 1–12.
Singh, G., & Launer, S. (2018). Time of day and hearing aid adoption. Trends in Hearing, 22, 1–14.
Singh, G., Launer, S., & Glista, D. (2017). Does discussing emotion during audiology appointments facilitate hearing aid adoption? International Journal of Audiology, 56(2), 117–124.