
Marketing may not be the most emphasized topic in audiology programs around the country, if it is even covered much at all. Most private practice audiologists would agree, however, that successful marketing is probably the most important factor that will determine whether or not their practice is profitable, and subsequently successful.
If you are an audiologist trying to market your practice, how can you do it effectively? How can you succeed, if not thrive, going up against competitors that are spending 10% of their gross revenues on marketing, which appears to be the average? Even if you are willing to invest that much money, how do you know you are maximizing your return on investment?
First, start by getting in the right frame of mind to think differently about the way you market your audiology practice. It is said that Albert Einstein defined "insanity" as doing the same thing over and over again but expecting different results each time. Mr. Einstein would probably say that the hearing care industry is insane because it has generally marketed the same way for decades yet it has not reached the substantial potential. I am not suggesting that you forget all of the traditional ways of marketing and advertising your practice;I am simply suggesting that you keep an open mind to a new technique - Medical Referral Marketing. Instead of marketing directly to consumers, market to their physicians in an effort to get these physicians to refer them to you for hearing care.
Medical Referral Marketing is not really new at all! It has been taking place within the medical community (i.e. physician-to-physician) for a long time. Most medical specialists rely on other doctors for most of their new patient acquisitions. Doctors that primarily market directly to the consumer are generally the exception, not the rule. These include plastic surgeons, cosmetic and general dentists, Lasik surgeons, and certainly anyone trying to market Botox or the myriad of elective cosmetic services to Baby-Boomers and Generation Xers that yearn to be young again.
Most patients that require the services of a medical specialist are referred by their primary care physician (PCP) or another medical specialist. For example, if a 65-year old man complains to his PCP about persistent urinary problems, he would most likely be referred to a urologist. The urologist may perform tests that diagnose prostate cancer. The urologist would then refer the patient to a medical or radiation oncologist for cancer treatment.
How did the patient arrive at that particular urologist? It is because his PCP, his regular family doctor, someone he knows and most likely trusts, recommended that specific urologist. Did the patient have a choice? Sure he did. However, unless he had been to another urologist beforehand or had been influenced by someone else he trusts (whether it is another doctor, a relative, or friend), he will most likely take the advice of his PCP.
Why did his PCP refer him to that particular urologist? It was because the PCP had enough knowledge about this urologist's capabilities and trusted that this particular urologist was the best to care for his patient. Simply put, doctors refer to others that they know and trust. More specifically, doctors refer to professionals that they know are capable and that they trust will care for their patients in a way that will not reflect poorly on them for the referral.. This element of trust is an important factor to understand, because the referring doctor's reputation is at stake;therefore, doctors must be comfortable with those to whom they refer their patients.
The same pattern explains why that same patient arrived at a particular oncologist's office. It's because the urologist recommended him. The patient trusts the urologist's recommendation because his PCP trusts the urologist. The urologist, in turn, trusts the oncologist. Once again, it is all about trust. Does another urologist or oncologist have an opportunity to market directly to this patient to influence him to make a choice that may be different from his doctor's recommendation? Yes, if they are willing to spend enough money to reach this patient and make enough of an impact to influence him. However, it may not be cost-effective for these specialties to use this approach.
Imagine that you woke up today with an excruciating toothache. The first thing that you would probably do is make an appointment with your dentist. If your dentist then determines that you need a root canal, he or she would most likely refer you to an endodontist, a root canal specialist. If you knew someone that recently had a root canal and that person recommended a particular endodontist, you may bypass your general dentist and seek that endodontist directly. However, the likelihood that you would go to the Yellow Pages or Google to look for an endodontist is slim to none. If you have never had a root canal, you may not have even known what an endodontist does until now. That is because, traditionally, direct-to-consumer advertising is not common in endodontics;it is simply not cost-effective. Professional referral marketing is the norm. The same is true for the other dental specialties: orthodontics, periodontics, prosthodontics, and oral surgeons. They all market to the general dentist.
In this article, I will explain why medical referral marketing for an audiology practice represents a huge opportunity and how an audiology practice should implement a successful medical referral marketing program. I will examine the 'Keys to Success,' as well as the potential pitfalls, so that you can maximize your marketing budget's return-on-investment.
First, consider how the hearing care industry has historically advertised. Through the decades, practices have typically marketed directly to the consumer, using traditional advertising media as the primary method for acquiring new patients. Among dispensing practices, the most common method is print ads, followed by direct mail. Print ads are typically placed in local newspapers and magazines that cater to the senior demographic, which represents the highest percentage of hearing instrument users. Direct mail is generally done to age-specific lists, usually ages 65+. These lists are readily available through list compilers. Many of the most qualified list compilers can overlay (combine) multiple "selects," or factors, such as household income, to customize a list as specific to your needs as you are willing to pay. Contact the Direct Marketing Association (www.the-dma.org) for their list of recommended compilers or me at www.HealthcareMarketingTools.com for a recommendation.
Television and radio became a popular media for marketing in the 1980's, especially among manufacturers that tried to build brand name recognition at the consumer level. Beltone™ and Miracle-Ear™ successfully built their brands through national television campaigns. TV has now become a more viable option for dispensing practices. Cable TV companies offer local options that enable advertisers to broadcast within a smaller geographic area, making it more cost-effective to drive patients to fewer locations.
In addition to brand recognition, Beltone™ and Miracle-Ear™ have generated thousands of prospect leads for their exclusive dispenser networks. Beltone™ and Miracle-Ear™ can afford to spend more on direct-to-consumer advertising because they distribute their products through an exclusive dispenser network. Other manufacturers have focused their marketing efforts on the professional (their customer), not the end-user. They have to in order to convince hearing care practices to choose their products over their competitors.
Public relations efforts within the industry continue among manufacturers and dispensing practices. Manufacturers try to gain free press whenever they introduce a new product or software. Dispensing practices frequently build ad campaigns around announcements such as, "May is better hearing month," and try to get the media to supplement their efforts. I applaud the manufacturers that donate free instruments to needy patients. The Starkey Hearing Foundation is a great example of a manufacturer's commitment to help those that are most needy to hear better, and they deserve any publicity they receive for it. These efforts recently resulted in Bill Austin appearing on ABC's Dancing With the Stars, showing him donating hearing aids in Mexico with actress Marlee Matlin. Although this may inspire some of you to buy more Starkey products, is it driving any prospects through your doors?
The internet is certainly the newest marketing medium within the industry, and it appears to be growing significantly. According to Dybala (2007), the term "hearing aids" is searched on the internet over 2 million times annually. More practices are creating web sites in order to keep up with the pace;however, seniors are the least likely to search on the internet. Although this may not be the greatest opportunity to capture new patients today, it will most likely change in the future as Baby Boomers continue to age. Simply having a website will not be enough. Search engine optimization will be the most critical and pay-per-click campaigns may also be necessary for a practice to have the necessary presence on Google and other top search engines, in order to effectively compete on the web.
Keep in mind that your website should also be a resource for your medical referral sources, your patients, and their families. In the future, more people will require information electronically. Audiology practices that deliver information electronically, such as e-newsletters, pod casts, and web casts, will be in a more competitive position. Today's audiology practice needs more than just a website. It needs a website and a web STRATEGY.
Now, look at the messages that have been conveyed through these media. If your marketing is going to be successful, it is extremely important to have an emotionally compelling message to your target audience. Consumers generally respond emotionally to a marketing message and then justify a purchasing decision rationally.
Most of the messages that have been communicated to consumers throughout the years have been related to products and technology. First, it was hearing instrument size. From the advent of body aids, each technological progression became smaller and less conspicuous for the patient: BTEs, ITEs, ITCs, and CICs. Vanity has always been an issue for the "active" senior;therefore, the smaller the better. Each progression spurred marketing campaigns and generated new patients as well as opportunities to upgrade existing patients that saw the benefit of investing in smaller instruments that better fit their lifestyle.
Hearing instrument circuitry and software have also been commonly used themes in consumer marketing campaigns. Each has attempted to convince the patient that not only does size matter, but what is inside the hearing aid as well as your audiologist's ability to program it with the right software also matters. Important note -any marketing message directed to the consumer that focuses on hearing aids or related hearing instrument technology will only appeal to those in the marketplace that are consciously looking to buy a hearing instrument in the near future! These people are already asking themselves what hearing aid to buy and who to buy it from. Typically, prospects that respond to a product message are no longer questioning whether they need a hearing aid;they are past that point already. Marketing to this population does not represent the greatest opportunity, which I will prove when I share some compelling statistics with you from the MarkeTrak VII survey (Kochkin, 2005).
Other technology has also been used in marketing messages throughout the years. Since the advent of the audiometer, "Hearing Test for Senior Citizens" has been a common headline in many a print ad and direct mail piece. In the mid 90s, the introduction of the video otoscope enabled patients to see their ear canals for themselves for the first time. This spurred headlines such as "Hearing loss or just earwax buildup?"
The hearing test and video otoscope are topics that have been extremely successful in the marketplace with consumer-direct advertising. The reason for their success is because they promise to provide customers with valuable information and answers to important hearing care questions at a very important stage in their personal educational process. These questions include the following: Do I have a hearing problem? If so, how bad is it? What is causing the problem? How can I fix it?
Many audiologists are simply marketing "better hearing." These advertisements promote experienced, certified audiologists, utilizing comprehensive testing methods and the latest equipment to determine if patients have a problem, why, and what the best course of treatment would be for them. Even if you are marketing better hearing and not hearing aids, does consumer-direct marketing represent the biggest opportunity?
Consider the following statistics from MarkeTrakVII, a survey conducted in 2004 by the Better Hearing Institute among individuals in the U.S. with hearing loss. This is the latest data of this kind that is currently available (Kochkin, 2005).
The first compelling statistic from MarkeTrakVII is hearing instrument adoption rates. These are the percentages of people with hearing loss who own hearing instruments from 1984-2004:

During this period, the industry had not successfully reached even one out of four hearing- impaired Americans. With all of the various media we now have to reach consumers, all of the product and software innovations to reduce instrument size and improve listening quality, and all of the different ways we can market hearing aids and better hearing to consumers, we still cannot help more than one out of four hearing-impaired Americans! Direct-to-consumer marketing, no matter how you try to dress it up, does not seem to be getting this industry the penetration it needs and the hearing-impaired population deserves.
The second compelling statistic is the number of people with hearing loss (in millions) from 1989 to 2004 with projections through 2050:
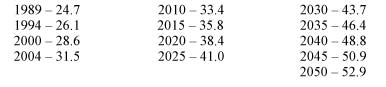
The industry has been growing due to population growth fueled by the aging of the Baby Boomer generation. This growth has also fueled complacency within the industry. I also believe that advances in technology and manufacturing have lead to increased gross profits for manufacturers and dispensers, and this is also partly to blame for complacency. I am not suggesting that generating profits is not a good thing. I make my living helping practices make more money;therefore, that would be hypocritical. My point is that change is difficult. Change usually does not occur until the pain of change itself becomes less than the pain of staying the same. This industry is at a comfort level that has not forced it to make a radical paradigm shift in the way it markets its products and services.
How can we reach more of the hearing-impaired population in order to increase hearing aid acquisition rates? Most importantly, if the industry is too complacent to make a concerted effort to change, what can you do in your individual market? The answer is marketing to physicians. I will explain why this represents the greatest marketing opportunity for this industry.
Assume we are now approaching 33 million hearing-impaired Americans (33.4% projected in 2010). If we assume the adoption rate of 23.5% in 2004 remains unchanged, then approximately 7.75 million people currently own hearing instruments (users). That leaves 25.25 million hearing-impaired non-owners (HINOs). Before we can figure out how to truly reach these 25+ million HINOs, we have to understand the psychology of this group and what is important to them.
Although many studies have shown that there are considerable negative psychological, social, and health effects of untreated hearing loss, hearing loss is gradual and there is no pain involved;therefore, it is "invisible" to the patient for a long time. This is why denial appears to be the primary barrier to getting a patient to seek help and accept amplification. Why would a patient in denial respond to a marketing message about better hearing, much less a marketing message about hearing aids? They are not interested because they believe there is no need.
Because hearing loss is gradual, most patients experience hearing loss for long periods of time before being properly evaluated and diagnosed, if they even seek help at all. Typically, patients' families, friends, and co-workers notice the hearing loss before they do. Unfortunately, the influence that these third parties have on the patient is negligible. Attempts to convince the patient to seek help and get tested usually go unheeded due to denial. According to MarkeTrakVII, 50% of adults with hearing loss have never had their hearing tested professionally. Those that do often have a hearing loss for 7-10 years (sometimes more) before finally getting their first hearing test (Kochkin, 2005). I refer to this as the "River of Molasses". The "River of Molasses" is the unusually long period of time that a HINO is "stuck" living with hearing loss before getting a hearing test for the first time, if ever at all. Direct-to-consumer marketing messages communicating better hearing may only appeal to HINOs that have been floating along the "River of Molasses" long enough to finally realize they may have a hearing problem and decide to seek help. This represents a very small percentage of the 25.25 million HINOs.
Marketing messages communicating hearing aids will only appeal to a small percentage of the potential market as well. MarkeTrak VII estimates the mean age of hearing instruments to be 4.5 years (Kochkin, 2005). Many audiologists would agree that this is the best time to begin to market potential upgrades to existing patients. The instruments may be nearing the end of their useful lives and there may be more advanced technology that could benefit the patient, especially if the loss has changed significantly. Even if half of the 7.75 million current hearing aid users represented resale opportunities, how many would justify the additional expense by the incremental benefit? Certainly these are the exceptions.
It is important to note that internal marketing to current patients should always be an important part of an overall marketing plan. All practices should have programs and processes in place to market to their patients to upgrade technology and to generate patient referrals. Keep in mind that the best ways to communicate to your current patients about new technology and encourage them to refer others are face-to-face during regular hearing aid maintenance appointments, direct mail, and email. I am amazed at how many practices spend so much money on newspaper advertising with hearing aid messages, when these messages only appeal to existing users and HINOs that are at the furthest point on the "River of Molasses" that they are already thinking about purchasing hearing instruments. This is not as cost effective because you are paying to reach a high percentage of readers that are not viable prospects.
The industry's biggest opportunity will be successfully reaching these HINOs earlier as they float down the "River of Molasses". A radically different approach must be used, because traditional marketing messages through the typical media are not making enough of an impact. Even the HINO's spouse, family members, friends, and co-workers do not seem to be making enough of an impact to influence the HINO to take action. In my opinion, the most influential person can be the patient's physician, especially the PCP. PCPs are in a good position to identify whether or not their patients have hearing loss because they can either screen in their office or refer, preferably to your office, patients who show signs of hearing loss. Most importantly, patients generally listen to their doctor's instructions.
MarkeTrakVII estimated that only 12.9% of people were screened for hearing loss during physical exams in 2004. In 1990, it was 20.2%. This downward trend represents an opportunity to market the need for better hearing care to the medical community. Kochkin (2005) suggests several outstanding recommendations for marketing to the medical community;however, many of these ideas are not cost-effective for the industry. He suggested the following:
- Paid public service announcements in medical magazines. (Good idea, but who is going to pay for it?).
- Getting hearing loss screeners in physicians' hands. (PCPs are already working harder every year.).
- Creating pull-through from patients. If they can ask their doctors for Nexium™ or Viagra™, they can ask for a hearing screening. (Great in theory but even if all of the manufacturers agreed to invest in a "Got Milk?" type of campaign, it would be a drop in the bucket compared to the money the pharmaceutical companies spend to create awareness.).
- Getting AARP and other large consumer organizations to help put pressure on the medical community to include hearing screenings during physical exams. (Great idea, but who is taking the lead?).
- Leveraging the Medicare Prescription Drug, Improvement, and Modernization Act of 2003, encouraging physicians to use screening questionnaires to determine if patients have hearing or dizziness problems. (This is among the best of Dr. Kochkin's recommendations. It reinforces one of the effective tactics in a local medical referral marketing program.).
How do you get physicians in your market to refer their patients to you? How do you educate them so that they see the need and influence them so that they trust you? Keep in mind that medical referral marketing is a process. There is no "magic bullet" in marketing an audiology practice in general, nor is there one to marketing to physicians. It is a process that must be followed step-by-step.
This process takes time. I describe it as being similar to farming. Marketing is the way you feed your practice. Centuries ago, before you could drive to the grocery store, you fed your family by either farming or hunting and fishing. Hunting and fishing get an immediate return for your efforts - you shoot, you kill, you cook, and you eat. Farming, on the other hand, takes time. You have to find the right field to plant the farm, plow the field, plant the seeds, water and fertilize the seeds, and tend to the crop for a long time until it grows and is ready for harvest. That is what the medical referral marketing process is like. You have to identify who the physicians are within your market, reach out and communicate with them in various ways, build relationships with them, and cultivate the relationships until you gain their trust. You will not be ready to "harvest" until you have first accomplished all of these tasks. Historically, the hearing care industry has used "hunting" methods of marketing because it wants an immediate return and does not have the patience to farm. There are eight steps to the "farming" medical referral marketing process.
Step 1 - Designate a practice liaison or practice representative within the practice to manage and implement this process. Ideally, this should be an audiologist, but this is not completely necessary. The practice representative will be the liaison to your referral community, building name recognition through education and relationship building. The key will be for this person to have strong verbal communication skills and not be intimidated by physicians or their staff. For a solo audiology practice, this is often the owner.
Step 2 - Compile a database of all PCP practices within your marketing area that would represent potential referral sources. Capture as much information about each practice as possible. Include each physician's name, as well as each staff member's name and title, if possible. Among key staff members, the most important will be the referral coordinator. In smaller practices, this function will be part of the nurse or office manager's responsibilities. Also compile all contact information including address, main telephone number, back-office telephone number, fax number, and email addresses. Some of this data will be readily available through list compliers, telephone books, or the internet. Unpublished information, such as back-office lines and general staff members' names and titles, you will have to gather as you go along. This database should constantly be updated and added to as you go;therefore, I suggest using some type of contact management software.
In addition to PCPs, consider adding other medical specialists to your target list, especially those specialists that treat conditions common to seniors. This would include cardiologists, urologists, oncologists, ophthalmologists, and others. Also consider adding additional specialists who practice in areas that are heavily populated by seniors, because they would also tend to treat a higher percentage of HINOs.
Step 3 - Begin to build a relationship with the referral coordinator. The referral coordinator is the "gatekeeper" that you must influence enough to gain his or her trust in order to gain access to the doctor(s). Begin with a series of direct mail educational campaigns addressed specifically to the referral coordinator by name. Emphasize that your goal is to help them. Give them facts to show healthcare professionals understand how prevalent hearing loss is in our society, how over three out of four hearing-impaired Americans go undiagnosed or untreated, and that studies have linked untreated hearing loss to many negative social, psychological, and health conditions. Mention that you would be happy to meet briefly to help them understand the signs of hearing loss and what should be done to correctly evaluate the patient. Let them know that you will call to confirm they received this important information. The goal is to meet the referral coordinator in person.
Follow up the mailing with a telephone call to the referral coordinator to confirm that he or she received the information and to try to schedule an appointment. Keep in mind that you will not be successful reaching everyone by telephone and may have to "cold call" many practices to try to get through to the referral coordinator.
Step 4 - Meet with practices in person. When calling on a medical practice, whether it is by appointment or a cold call, your practice representative must come armed and prepared. The representative should have a comprehensive practice kit, which includes professionally designed branded collaterals and information that communicate in detail not only what the practice does (comprehensive audiometric testing, hearing instrument dispensing, maintenance and repairs, assistive devices, vestibular testing and rehabilitation, etc.), but also lists the practice's capabilities. This will put you in a better position to communicate your unique brand and why the medical practice should choose you when referring patients. Other important tools should include copies of published studies on hearing loss prevalence and the health effects of hearing loss on the patient, as well as hearing loss screening forms to enable the medical office to identify potential candidates requiring evaluations.
Step 5 - Get access to the doctor and the rest of the staff. Leverage the relationship you develop with the referral coordinator to gain access to the physician and the staff. Try to develop relationships with each physician and staff member to gain trust. Another tactic is to offer to provide a brief "lunch & learn", where you can meet with all physicians and staff during lunch to conduct a brief educational talk. In a busy practice, you may only get their time during lunch but your investment in their meal is money well spent.
Step 6 - Market to targeted practices on an ongoing basis. Remember, this is like farming;you may not gain trust and subsequently receive referrals immediately after meeting with a medical practice for the first time. Provide ongoing educational mailings and establish an ongoing call cycle to continue to meet with practices in person in order to build awareness and recognition within the medical community.
Step 7 - Track results. As you start to gain referrals from these physicians, it will be important to track referral totals from your list. This is your "Key Referrer" list. Your outreach call cycle, or how frequently you attempt to market face-to-face with these practices, will depend on the number of referrals you are getting from each practice. In my experience, practices that have mature medical referral marketing programs will have a key referrer list whereby the "Pareto Principle" (commonly known as the "80/20 Rule") will apply. In this case, 80% of the referrals will typically come from 20% of the referring sources and vice-versa. These are your "A" referrers. Your "B" referrers represent the next 15% and "C" the remaining 5%.
Contrary to what most people would think, your call-cycle should be more frequent with your A's, than with your B's or C's. The logic is that you want to ensure that you maintain the relationships and trust that you worked so hard to build. Also, you can usually leverage relationships and trust that you have already built to develop new relationships. Perhaps one of the physicians will help you gain the trust of his or her partner for example. Staff members also represent a huge opportunity due to the fact that they may spend more time with the patient than the physician does, and, therefore, may be in a better position to identify the signs of hearing loss and subsequently bring it to the physician's attention.
Step 8 - Communicate consistently with your referral sources. Send the physician a copy of the patient's audiogram, along with a report detailing the results and your course of treatment. Include a completed patient satisfaction survey to reinforce that you are delivering the high level of care they expect you to provide to their patient. Continually ask for feedback from the physicians as to how you can help them help their patients further. Lastly, and most importantly, thank your referral sources for their trust in you to serve their patients.
By now you can see why traditional consumer-direct marketing efforts are not the most cost-effective way to market your audiology practice. Reaching the HINOs earlier on the ''River of Molasses" represents your biggest opportunity, PCPs are in the best position to help you leverage that opportunity by influencing their patients to get their hearing tested. You will need to take it upon yourself to build relationships with physicians in your market so that they trust you and will entrust you with their patients. Like farming, this is a process that takes time.
There are some Keys to Success that everyone implementing a medical referral marketing program should follow:
- Do not stop your other advertising if it is generating a profitable return-on-investment. Always have a comprehensive marketing program for your practice. Never have all of your eggs in one basket.
- Have patience. Remember that this is farming and it may take many months before you build enough awareness and trust within the medical community to generate referrals.
- Invest in professional branding and creative development. Retain a marketing company with a background in audiology. Choose one with a proven track record that also understands how to "brand" your practice so you can differentiate it from your competition. Do not try to do this on your own. It is essential to have the proper tools to market to the medical community and even more important to present the proper, professional image.
- Train your practice representative properly. It is critical that your representative knows the dos and don'ts of working with medical practices and the proper communication techniques. Your efforts must come across professionally and you cannot come across looking needy or greedy.
- Stick with it consistently. Practices that do not work the process long enough to build the trust and awareness they need will not be successful. Furthermore, practices that stop marketing consistently once enough referrals are generated will eventually lose those referrals. Like in farming, it not only takes time to harvest the crop, but once the harvest is complete, the field will eventually die if it is ignored.
Rich Hachenburg is the President and Founder of Competitive Edge Healthcare Marketing, a full-service marketing firm that specializes in working with physicians and healthcare practices. Rich has over 24 years of consulting experience, 18 of which have been in the healthcare field. Rich started his career in healthcare marketing with Beltone Electronics Corp., where he served as Regional Manager and progressed to Area Vice President Southeast. Rich founded Competitive Edge in 2002 and has since served virtually all healthcare specialties, including physicians, medical specialists, dentists, audiologists, and physical therapists.
Rich helps his clients market their practices more effectively by developing comprehensive marketing plans, creating marketing tools and materials, and coaching the key employees toeir plans so that they can achieve their goals. Rich has personally consulted with over 2000 healthcare practices.
For more information, Rich can be contacted through his company web site, www.HealthcareMarketingTools.com, directly by email at [email protected], or by telephone at 561-477-6348.
References
Dybala, P.D. (2007, October 25). Internet, Marketing and Your Practice Website. AudiologyOnline, Recorded Course 9916. Retrieved March 20, 2008 from the e-Learning section on www.audiologyonline.com
Kochkin, S. (2005). MarkeTrak VII: Hearing loss population tops 31 million. Hearing Review, 12, (7), 16-29.
