
Question
How Can Clinicians Apply and Interpret the Video Head Impulse Test (vHIT) in Everyday Practice?
Answer
INTRODUCTION
Since its adoption into clinical practice in 2009, the Video Head Impulse Test (vHIT) has significantly reshaped how clinicians evaluate the vestibulo-ocular reflex (VOR) in patients with dizziness and balance disorders. Unlike the traditional bedside head impulse test (HIT), which depends on visual observation and provides only qualitative information, vHIT delivers an objective, quantitative assessment of VOR function across all six semicircular canals.
In my work as a neurologist specializing in vestibular disorders, vHIT has proven invaluable, not only for establishing diagnoses but also for tracking patient progress and guiding rehabilitation strategies. In this article, I will share practical insights into the clinical applications of vHIT, approaches for interpreting results in different pathological conditions, and examples of how this tool supports real-world decision-making.
OVERVIEW OF vHIT
The traditional Head Impulse Test (HIT) can identify overt saccades but fails to capture covert saccades, which occur during head movement and remain invisible to the naked eye. The Video Head Impulse Test (vHIT) overcomes this limitation by using high-speed infrared video to measure both overt and covert saccades, while also calculating VOR gain. This provides a precise and objective assessment of semicircular canal function.
From a physiological perspective, type I hair cells are most responsive to high-frequency head movements, exactly the range assessed by vHIT, whereas type II hair cells respond primarily to low-frequency stimuli, such as those tested with calorics. This explains why vHIT and caloric testing may sometimes yield different results: each evaluates a distinct frequency domain of vestibular function.
CLINICAL APPLICATIONS OF vHIT
1. Peripheral Vestibular Disorders
In cases of acute unilateral vestibulopathy (AUVP), vHIT typically reveals reduced gain and corrective saccades on the affected side. During the acute phase, both type I and type II hair cell functions are impaired, resulting in abnormal findings on both vHIT and caloric testing. Over time, however, high-frequency function (type I) often recovers more quickly, so vHIT results may normalize while caloric deficits persist.
In Ménière’s disease, the pattern is more variable. Early in the disease course, high-frequency function is often preserved, leading to normal vHIT findings alongside abnormal calorics. In advanced stages, both assessments are commonly impaired.
vHIT also plays a critical role in diagnosing bilateral vestibulopathy. These patients show a characteristic bilateral reduction in VOR gain across the horizontal canals, often accompanied by scattered overt and covert saccades. Compared to caloric testing—which can be uncomfortable and time-consuming—vHIT provides a rapid, non-invasive way to confirm bilateral deficits. Equally important, it enables clinicians to monitor compensation and residual function, guiding rehabilitation strategies and informing patients about long-term prognosis.
2. Central Disorders
Certain central pathologies, such as cerebellar lesions or vestibular migraine, can paradoxically present with elevated VOR gain. This is often accompanied by anti-compensatory quick eye movements—an important clinical clue pointing toward a central rather than peripheral origin.
3. Acute Vestibular Syndrome (AVS)
One of the most valuable applications of vHIT is in the emergency setting to differentiate central from peripheral causes of AVS. In a patient with spontaneous nystagmus and vertigo, a normal vHIT raises concern for a central lesion, such as a posterior circulation stroke. In contrast, a clearly abnormal vHIT strongly supports a peripheral cause, such as vestibular neuritis.
INTEGRATION WITH OTHER TESTS
vHIT is not a replacement for calorics or vestibular-evoked myogenic potentials (VEMP), but rather a complementary tool. For example, a patient with abnormal calorics but normal vHIT likely has a low-frequency deficit, common in Ménière’s disease, whereas concordant abnormalities on both tests suggest broader vestibular involvement.
INTERPRETING vHIT RESULTS
Key Parameters
- VOR gain: Normal values are >0.8 for the lateral canals and >0.7 for the vertical canals.
- Saccade type:
- Overt saccades: Occur after the head movement and are visible to the naked eye.
- Covert saccades: Occur during the head movement and can only be detected with vHIT.
- Mixed patterns: A combination of overt and covert saccades.
Patterns in Pathology
- Pure overt saccades: Often associated with more severe or uncompensated vestibular deficits.
- Pure covert saccades: Suggest partial compensation; patients may experience fewer symptoms despite measurable deficits.
- Mixed patterns: Frequently observed during recovery phases.
- High VOR gain (>1): Should raise suspicion of central causes such as cerebellar dysfunction or vestibular migraine.
Gain Calculation Methods
There are three primary approaches to calculating gain:
- Velocity gain – assessed at ~60 ms after movement onset.
- Regression gain – based on linear regression of head versus eye velocity.
- Area-under-the-curve ratio – comparing integrated head and eye velocity.
In routine clinical practice, velocity gain is the most widely adopted method due to its simplicity and reliability.
CASE EXAMPLE
Patient Details
65-year-old male
Presenting Complaints
- Daily episodes of oscillopsia (objects appearing to shake) with head movements while walking, ongoing for the past two months
- Unsteadiness during ambulation
- Symptoms triggered both spontaneously and in positional contexts, especially when turning the head right or left or when looking downward
- The patient has stopped driving and discontinued morning walks due to imbalance
- Reports reduced focus and concentration
Clinical Impact
- Dizziness Handicap Inventory (DHI): 36 (mild to moderate handicap)
- Visual Vertigo Analog Scale (VVAS): 30 (suggestive of visual motion sensitivity)
Investigations
- Reduced vestibulo-ocular reflex (VOR) gains in both lateral canals (Right: 0.68, Left: 0.72)
- Scattered overt catch-up saccades observed
- Findings consistent with bilateral vestibulopathy with poor compensation
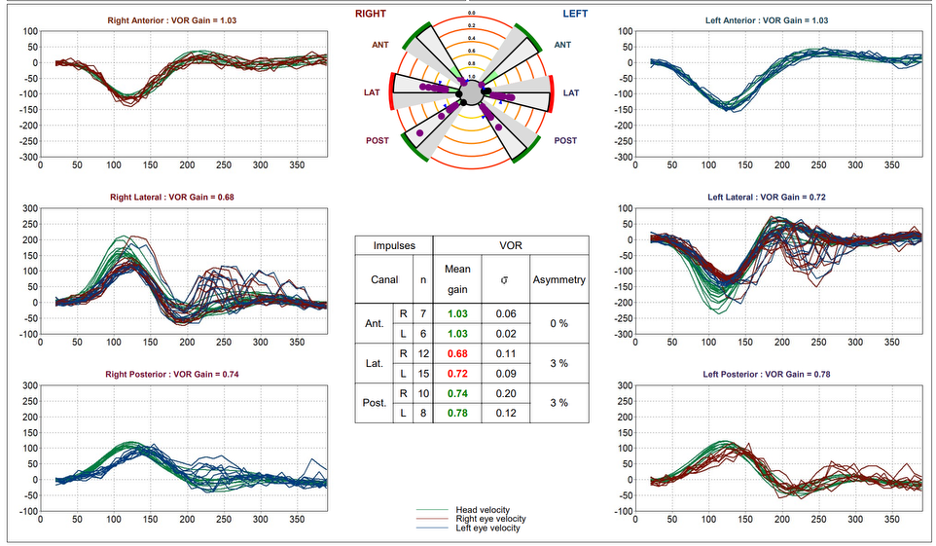
Fig. 1 Horizontal canal vHIT traces showing bilaterally reduced VOR gain. Scattered overt catch-up saccades are evident after head impulses, consistent with bilateral vestibular dysfunction.
Diagnosis
Uncompensated Bilateral Vestibulopathy.
Management
Patient initiated on Vestibular Rehabilitation Therapy (VRT) aimed at improving gaze stabilization, postural control, and central adaptation.
PRACTICAL CONSIDERATIONS IN TESTING
To ensure accurate vHIT results, several factors should be kept in mind:
- Seat the patient on a stable chair with the head upright and eyes focused on a small target approximately one meter away.
- Use passive head impulses; active head movements can mask vestibular deficits.
- Minimize jaw clenching or talking during testing, as these can create artifacts by shifting the goggles or altering camera alignment.
- In pediatric patients, maintaining attention can be challenging; engaging visual targets can help sustain focus. In individuals with cognitive impairment, clinical history and complementary tests may provide more reliable information.
FUTURE PERSPECTIVES & INTEGRATION IN CLINICAL PRACTICE
The role of vHIT is evolving beyond its traditional use as a diagnostic tool. Increasingly, clinicians are applying it to:
- Monitor rehabilitation progress by tracking changes in covert saccade frequency and VOR gain over time.
- Guide therapy decisions, including the intensity and timing of vestibular rehabilitation programs.
- Complement the functional Head Impulse Test (fHIT), which assesses a patient’s ability to maintain visual acuity during head movements—helping to bridge the gap between laboratory measurements and real-world function.
Technological advances, such as remote camera systems by Inventis, have also made vHIT more comfortable and accessible. This is particularly valuable for pediatric patients and for individuals who may struggle with tight-fitting goggles.
KEY TAKEAWAYS
- vHIT provides a rapid, quantitative assessment of all six semicircular canals and captures both overt and covert saccades.
- It serves as a complement, not a replacement, for other vestibular tests such as calorics and VEMP.
- Interpretation requires consideration of gain values, saccade patterns, and the overall clinical context.
- Characteristic patterns differ across peripheral, central, and mixed vestibular pathologies, shaping both diagnosis and management.
- vHIT is a valuable tool for guiding and monitoring vestibular rehabilitation over time.
References:
- MacDougall HG, et al. The video head impulse test: diagnostic accuracy in peripheral vestibulopathy. Neurology. 2009.
- Halmagyi GM, Curthoys IS. A clinical sign of canal paresis. Arch Neurol. 1988.
- Strupp M, et al. Peripheral vestibular disorders: an update. Lancet Neurol. 2020.
Resources for More Information
- Discover our solutions for vestibular analysis on our website:
https://www.inventis.it/en-na/solutions/balance-unique-solutions
- Check out the following courses published on AudiologyOnline:
Continued and its subsidiaries provide professional education authored by qualified Subject Matter Experts for continuing education purposes. These materials are intended for educational purposes and do not constitute medical advice or a substitute for individual clinical judgment. Continued is not a clinical healthcare provider; the licensed professional is solely responsible for ensuring that the application of any techniques or information presented is within their legal scope of practice and jurisdictional requirements.
