Question
How does robotic-assisted cochlear implant electrode insertion reduce intracochlear trauma and support better hearing outcomes?
Answer
The Problem: Variability in Manual Insertion
Cochlear implant electrode array insertion is one of the most delicate steps in otologic surgery and continues to rely almost entirely on manual, by-hand techniques. Like any manual microsurgical task, human kinetics naturally introduces variability in insertion speed, insertion force, pressure, and motion. Published research demonstrates that this variability can contribute to intracochlear trauma, which in turn can influence cochlear health and patient outcomes.1-3 This becomes increasingly significant as cochlear implant candidacy expands to include a growing population of patients who still retain functional acoustic hearing to preserve.
Biomechanical research illustrates this problem clearly: recorded insertion forces during manual insertions show frequent spikes and wide variability across electrode arrays and surgeons, whereas robotic-assisted insertions at a controlled speed of 0.5 mm/sec produce a dramatically smoother and more consistent force profile.4
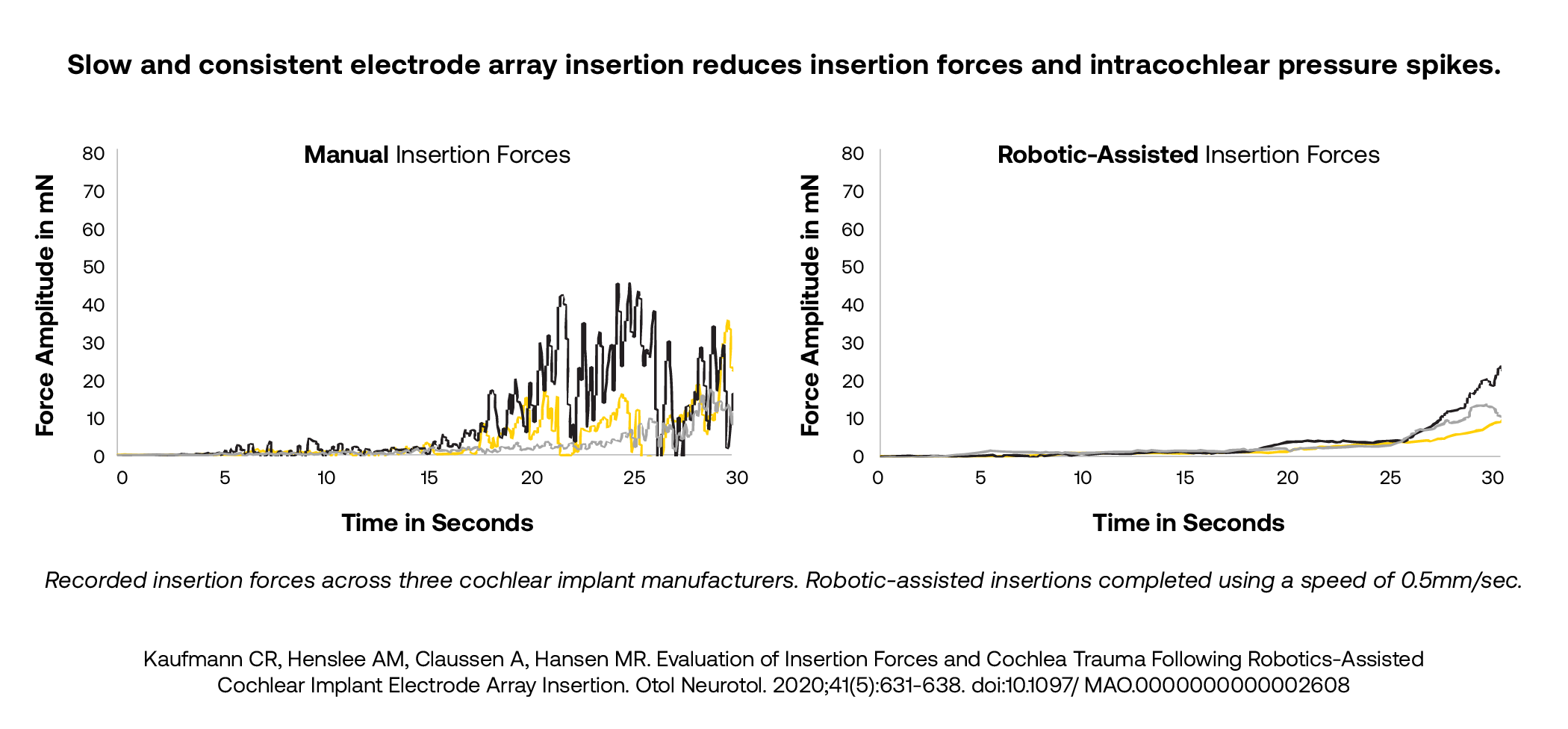
Figure 1. Comparison of insertion force profiles between manual and robotic-assisted cochlear implant electrode array insertions.
How the iotaSOFT® System Addresses Insertion Variability
The iotaSOFT® Robotic-Assisted Insertion System is the first and only FDA-cleared robotic-assisted technology for cochlear implantation.3 It is a thumb-sized, single-use robotic drive unit that integrates directly into the existing surgical field without altering the standard surgical approach. The surgeon maintains complete control throughout the procedure, activating insertion via a foot pedal and retaining the ability to switch to manual insertion at any time if needed. The system enables electrode array insertion at speeds as slow as 0.1 mm/sec—far slower than the human hand can achieve5—compared to an average manual insertion speed of approximately 1.6 mm/sec. By delivering slow and consistent electrode advancement, the iotaSOFT system can reduce force variation by up to 70% and maximum insertion forces by up to 51%, minimizing the large transient pressure events that can occur with faster, inconsistent manual insertions.1-3 Fast and inconsistent insertions have been shown to generate intracochlear pressure transients as high as 170 dB, which is the opposite of what clinicians and patients want for delicate cochlear structures.
The mechanical advantage of the iotaSOFT system’s slow insertion speed translates directly to a reduction in measurable intracochlear trauma. A comparative analysis by Claussen and colleagues evaluated trauma grades in cadaveric cochlear models and found that robotic-assisted insertions significantly decreased insertional intracochlear trauma scores compared with manual insertions.4
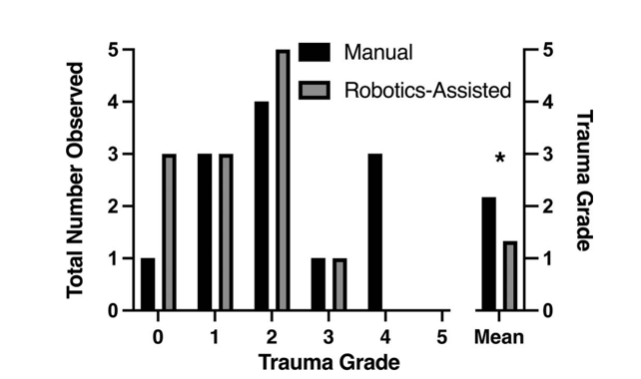
Figure 2. Distribution of intracochlear trauma grades in manual versus robotic-assisted cochlear implant electrode array insertions.
Clinical Evidence: Hearing Preservation and Long-Term Stability
The foundational mechanical science linking slower insertion to reduced intracochlear trauma is now being validated in published clinical outcomes data. Two recent studies published in The Laryngoscope by Khan and colleagues demonstrate that robotic-assisted electrode array insertion is associated with improved hearing preservation and greater stability of residual hearing over time.6 Importantly, the 2026 study found a statistically significant reduction in rates of delayed onset hearing loss (DOHL), defined as a drop in hearing thresholds of greater than 10 dB following implantation. In that study, 0% of patients in the robotic-assisted cohort experienced DOHL at one-year post-activation, compared to 29% of patients in the manual insertion group. The robotic cohort also demonstrated higher overall hearing preservation rates at one year: 85% for robotic-assisted versus 71% for manual insertion patients.7
Data from both studies illustrate that robotic-assisted patients maintained functional hearing across all post-operative time points, from initial activation through six months and one year, reflecting a pattern of cochlear health and structural preservation that manual insertion patients did not demonstrate at the same rate.
Clinical Implications for Audiologists
For audiologists counseling cochlear implant candidates, an understanding of the iotaSOFT system offers a practical tool for addressing some of the most common patient barriers to implantation—fear of surgery, uncertainty about outcomes, and concern about losing residual hearing. As Dr. Schapira noted, audiologists do not need to learn new programming software or a new family of devices to incorporate this knowledge into their practice. Rather, awareness of robotic assistance gives clinicians a concrete way to respond when patients express hesitation: by explaining that the surgical team has access to a physical tool specifically designed to go more slowly and more gently than the human hand, thereby reducing variability and supporting cochlear health. From a post-surgical care perspective, clinicians may observe lower electrode impedances and less impedance fluctuation following a robotic-assisted procedure, which can facilitate a more straightforward mapping process. Ultimately, this technology is applicable to all cochlear implant candidates—not only those with residual hearing to preserve—because a less traumatic insertion reduces scarring and supports better long-term cochlear implant outcomes for every patient.
This Ask the Expert is an edited excerpt from the course, Schapira, A. (2026, March 23). Robotic-Assisted Cochlear Implant (CI) Procedures Are Here. AudiologyOnline.
References:
1. Kaufmann CR, Henslee AM, Claussen A, Hansen MR. Evaluation of Insertion Forces and Cochlea Trauma Following Robotics-Assisted Cochlear Implant Electrode Array Insertion. Otol Neurotol. 2020;41(5):631-638. doi:10.1097/ MAO.0000000000002608
2. Banakis Hartl RM, Kaufmann C, Hansen MR, Tollin DJ. Intracochlear Pressure Transients During Cochlear Implant Electrode Insertion: Effect of Micro-mechanical Control on Limiting Pressure Trauma. Otol Neurotol. 2019;40(6):736- 744. doi:10.1097/MAO.0000000000002164
3. iotaMotion Data on File
4. Claussen AD, Shibata SB, Kaufmann CR, Henslee A, Hansen MR. Comparative Analysis of Robotics-Assisted and Manual Insertions of Cochlear Implant Electrode Arrays. Otol Neurotol. 2022;43(10):1155-1161. doi:10.1097/ MAO.0000000000003707
5. Kesler K, Dillon NP, Fichera L, Labadie RF. Human Kinematics of Cochlear Implant Surgery: An Investigation of Insertion Micro-Motions and Speed Limitations. Otolaryngol Neck Surg. 2017;157(3):493-498. doi:10.1177/0194599817704391
6. Khan UA, Dunn CC, Scheperle RA, et al. Robotic-Assisted Electrode Array Insertion Improves Rates of Hearing Preservation. Laryngoscope. Published online June 11, 2025. doi:10.1002/lary.32318
7. Khan UA, Scheperle RA, Podhajsky G, et al. Robotic-Assisted Electrode Array Insertion Improves Stability of Acoustic Hearing Thresholds. Laryngoscope. Published online January 21, 2026. doi: 10.1002/lary.70380
Continued and its subsidiaries provide professional education authored by qualified Subject Matter Experts for continuing education purposes. These materials are intended for educational purposes and do not constitute medical advice or a substitute for individual clinical judgment. Continued is not a clinical healthcare provider; the licensed professional is solely responsible for ensuring that the application of any techniques or information presented is within their legal scope of practice and jurisdictional requirements.

