
Question
What do Audiologists need to know about supporting a Cochlear Implant Replacement Sound Processor?
Answer
The Shift Away from the Five-Year Useful Life Rule
The reimbursement landscape for cochlear implant sound processor replacements has changed significantly in recent years. With the exception of traditional Medicare, which applies a five-year end-of-useful-life standard, chart notes must demonstrate continued use and benefit (CUB) by documenting the diagnosis, ongoing use and benefit of the device, and a current order, while commercial insurance payers and Medicare Advantage plans require specific, measurable evidence that a replacement is medically necessary. A standalone letter of medical necessity is no longer sufficient. Instead, payers expect that medical necessity be established and clearly documented within the patient’s clinical chart note. This shift places the clinical documentation itself at the center of the authorization process.
The three payer categories — traditional Medicare, commercial/Medicare Advantage, and Medicaid — each carry distinct coverage frameworks, and clinicians should be familiar with how those differences affect documentation requirements.
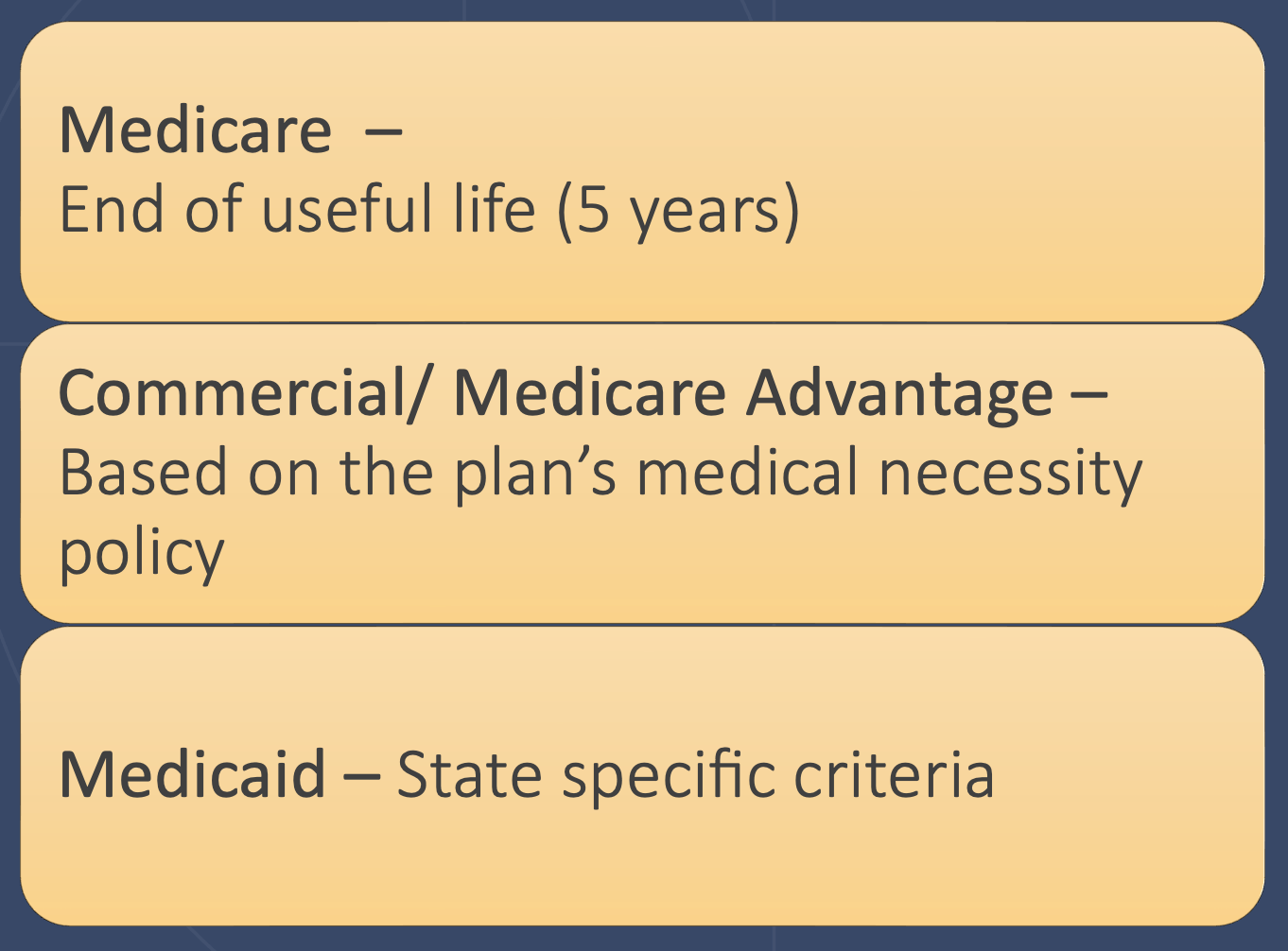
Figure 1. Coverage categories for cochlear implant replacement sound processors vary by payer type, with commercial payers and Medicare Advantage relying on individual plan medical necessity policies rather than a standardized time-based rule
Eligibility Criteria and Required Documentation
Eligibility for a medically necessary replacement sound processor is generally established once the current device is out of warranty - five years for a first processor, three years for an upgraded sound processor with Cochlear. Once that threshold is met, at least one of the following clinical criteria must also be satisfied: the sound processor no longer meets the patient’s needs, including support for activities of daily living (ADLs); the device is broken and no longer supported by Cochlear; or the device has been lost or stolen. Importantly, device retirement qualifies under the “broken and unsupported” criterion - a consideration particularly relevant now that the Cochlear™ Nucleus® 7 Sound Processor has been retired. In all cases, the specific situation must be clearly documented in the clinical chart note.
Clinical chart notes must include three essential elements. First, the reason for the replacement must be documented and tied to a functional or medical need - specifically, why the existing device no longer meets the patient’s clinical requirements. Second, the note must contain a written request to dispense the device due to medical necessity; vague language such as “recommended” or “discussed” does not establish intent to supply medically necessary equipment and can result in delays or denials. Third, the chart note must be authenticated with an electronic or ink signature and a date from the prescribing provider. A prescription signed by a physician, physician’s assistant, or nurse practitioner in accordance with applicable state requirements must also be submitted alongside the chart documentation.
The required documentation for initiating a replacement sound processor order encompasses not only chart notes and a prescription, but also an assignment of benefits, a completed order form, insurance plan details, and identifying information for the audiology team and managing physician.
Grounding Documentation in Functional Outcomes
The single most actionable principle from this course is that effective documentation ties hearing performance to functional outcomes. Insurance payers evaluate medical necessity based on functional impact, not device age or the availability of newer technology. Strong chart notes describe how processor limitations affect the patient’s ability to perform essential activities of daily living across three domains: safety and quality of life (e.g., operating a vehicle, responding to alert systems, participating in phone conversations); social and entertainment (e.g., communicating in noisy environments, attending social gatherings); and workplace or school (e.g., understanding instructions in noise, hearing peers across a classroom). Clinicians are encouraged to use the term “replacement sound processor” rather than “upgrade” in all payer-facing documentation, as payer claim systems apply keyword-based rules that can flag upgrade language as indicative of an elective request rather than a medical one.
Two additional cancellation triggers are worth noting in clinical practice. Reestablishment of care may be required if there has not been a recent documented interaction prior to a replacement request, and the nature of that interaction matters. Older notes (e.g., around 24 months) or documentation reflecting a previously stable patient must be updated to clearly support the current clinical status and rationale for the upgrade. Clinicians should also be aware that payers accept a range of encounter types to satisfy the engagement requirement, including in-person visits, telehealth appointments, phone calls, and documented electronic communications such as patient portal messages or email exchanges. Chart notes do not need to originate from in-person visits; what matters is that the documentation is clinically relevant, supports the reason for replacement, and includes the clinician’s own medical recommendation rather than simply relaying what the patient reported.
This Ask the Expert is an edited excerpt from the course, Noeller, S. (2026). Most Common Cancellation Reasons and How to Address Them. AudiologyOnline. https://www.audiologyonline.com/audiology-ceus/course/most-common-replacement-denial-reasons-41981
Continued and its subsidiaries provide professional education authored by qualified Subject Matter Experts for continuing education purposes. These materials are intended for educational purposes and do not constitute medical advice or a substitute for individual clinical judgment. Continued is not a clinical healthcare provider; the licensed professional is solely responsible for ensuring that the application of any techniques or information presented is within their legal scope of practice and jurisdictional requirements.