
Question
What is the role of the Video Head Impulse Test (vHIT) in Menière’s Disease?
Answer
Meniere’s Disease (MD) is an idiopathic inner ear disorder characterized by a sense of spinning dizziness (lasting from 20 minutes to 24 hours), fluctuating hearing loss (HL), aural fullness, and tinnitus, typically occurring in episodic attacks. The natural history of the disease is characterized by variable periods of exacerbation and remission of symptoms. Although several studies have shown the effectiveness of conservative therapy (both medical and surgical), ablative therapy with low-dose intratympanic gentamicin (ITG) (Casani et al., 2014) proved to assure very good control over the spells of vertigo. Relevant differences between MD patients often occur, particularly regarding the natural history of the vertigo and its correlation with hearing damage: the tendency is to have, as the disease progresses, an increased HL (initially affecting the low frequencies) and a decreased number and severity of the vertigo attacks.
A comprehensive assessment of the peripheral vestibular function is essential to stage the disease, plan treatment, and provide prognostic information. Both Caloric Test (CT) and vHIT represent validated methods to assess the function of the peripheral vestibular system. We analyzed the vestibulo-ocular reflex (VOR) both in patients who have been treated with ITG and in patients who have not. The vHIT findings will be put in relation to other instrumental parameters, such as canal paresis (CP), hearing loss, and duration of MD. The main objective is to establish, in a large sample of patients, whether an instrumental profile of an MD patient can be denoted by particular instrumental outcomes. Using vHIT to evaluate the activity of HF-VOR gain, we found no differences in early and late MD. We demonstrated a highly significant lower HF-VOR gain and a higher percentage of pathological HF-VOR in patients treated with ITG. Since the Asymmetry Index (AI)—which expresses the relative right-left asymmetry of the VOR gain—was normal in all patients treated only with conservative therapy, no correlation was found with AI nor with CP (Figure 1).
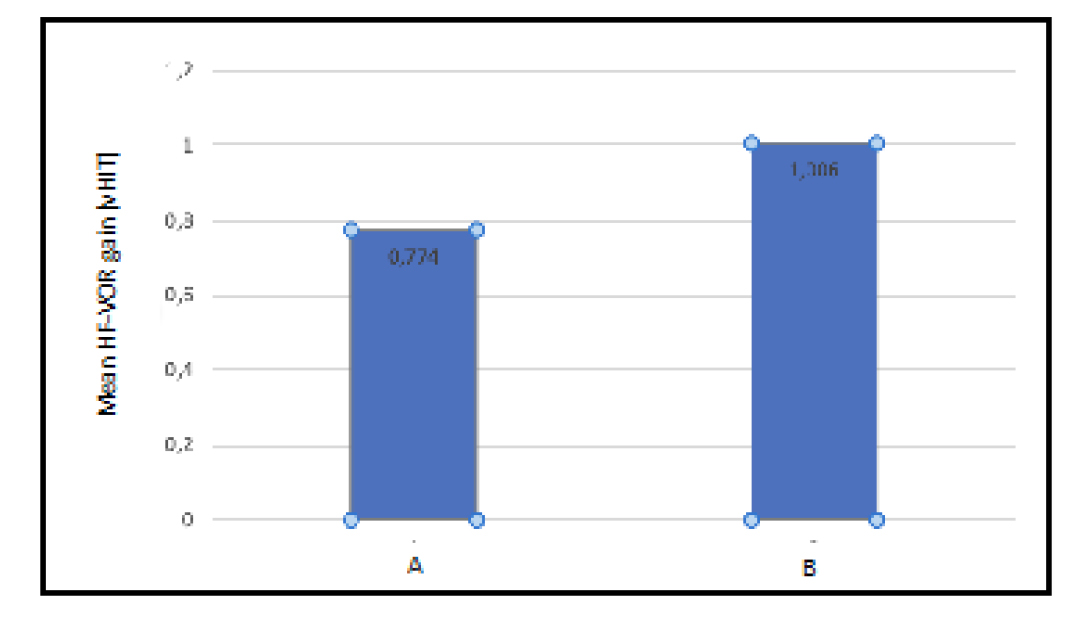
Figure 1. Mean HF-VOR evaluated using vHIT is significantly lower in patients treated with ITG (A) compared to values obtained in patients treated with conservative therapy (B).
On the other hand, a weak positive correlation between AI and CP was demonstrated in patients treated with ITG. To our knowledge, this is the first study to demonstrate the frequency-dependent behavior of the VOR using widely available devices such as CT and vHIT (it is well known that scleral magnetic search coils are invasive, expensive, and not available in most laboratories) in a larger sample of MD patients. Furthermore, our analysis is even able to assess important instrumental features related to different treatments of MD (conservative management vs employment of intratympanic ablative therapy), denoting a sort of instrumental profile of “untreated MD". The difference between patients treated with ITG and patients treated with conservative therapy in terms of HF-VOR gain was significant; vHIT findings were always normal if the patient didn’t undergo ITG (Figure 2).
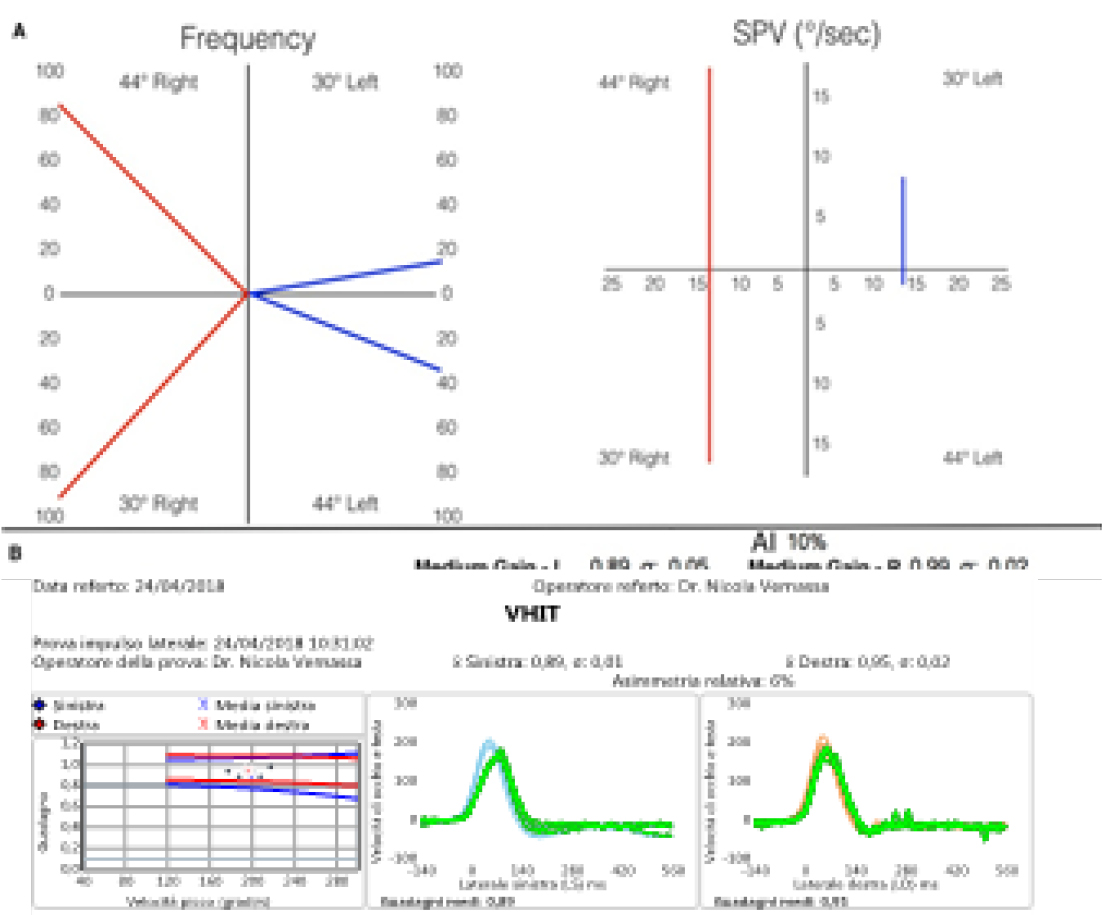
Figure 2. Results of caloric test and vHIT in a patient suffering from MD treated with conservative therapy. A: left canal paresis. B: bilaterally normal HF-VOR gain and no difference in terms of AI.
Therefore, our study suggests that the dissociation between CT and vHIT results can really represent, if patients undergoing ablative treatment are excluded, an instrumental hallmark of MD. On the contrary, A reduction of HF-VOR on vHIT in MD can represent a good indicator of an effective treatment with ITG (Cerchiai et al., 2016).
The preservation of VOR function on vHIT (Figure 3), despite diminished responses on CT, may have several possible explanations.
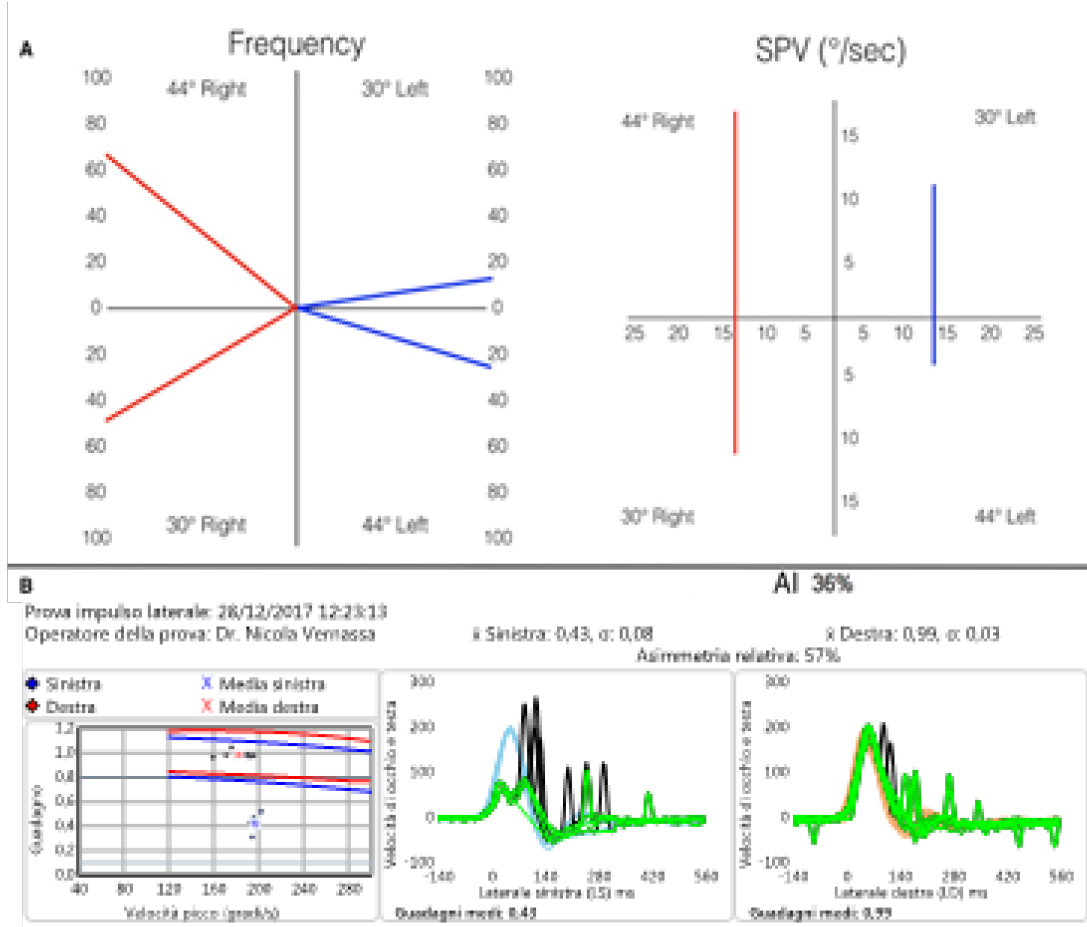
Figure 3. Results of caloric test and vHIT in a patient suffering from MD treated with ITG. Note the abnormal response of both CT (A) and vHIT (B) on the left side.
It is possible that MD preferentially impairs the ability of the vestibular apparatus to process low-frequency stimuli; perhaps the central adaptation mechanism to the damages induced by MD could be effective only for physiological high-frequency stimuli (vHIT) and not for unphysiological low-frequency ones (CT) (Agrawal e Minor, 2013).
Although it has been suggested that MD differentially affects various types of hair cells…CT predominantly stimulates regular afferents that respond to a sustained stimulus and will minimally stimulate irregular afferents that respond to a transient stimulus (McGarvie et al., 2015). Recent studies on human fresh tissue show that both type I and type II hair cells are affected about equally (McCall et al., 2009). A recent theory describes that a hydropic expansion of the HSC allows convective recirculation within the duct that causes dissipation of the hydrostatic force that would normally elicit nystagmus during CT (McGarvie et al., 2015).
References
Agrawal Y, Minor LB. Meniere’s disease and other causes of episodic vertigo. In: Bronstein AM, editor. Oxford Textbook of Vertigo and Imbalance. Oxford, UK: Oxford University Press; 2013. pp. 241 – 250.
Casani AP, Cerchiai N, Navari E, Dallan I et al. Intratympanic gentamicin for Meniere’s disease: Short- and long-term followup of two regimens of treatment. Otolaryngol Head Neck Surg 2014;150:847-852.
Cerchiai N, Navari E, Dallan I, Sellari-Franceschini S, Casani AP. Assessment of vestibulo-oculomotor reflex in Meniere’s disease: Defining an instrumental profile. Otol Neurotol 2016;37:380-384.
McCall AA, Ishiyama GP, Lopez IA, Bhuta S, et al. Histopathological and ultrastructural analysis of vestibular endorgans in Menière’s disease reveals basement membrane pathology. BMC Ear Nose Throat Disord 2009;9:4–17.
McGarvie LA, Curthoys IS, MacDougall HG, Halmagyi GM. What does the head impulse test versus caloric dissociation reveal about vestibular dysfunction in Meniere’s disease? Ann N Y Acad Sci 2015;1343:58-62.
Resources for More Information
To learn more about SYNAPSYS VHIT — our innovative goggle-free solution for vestibular assessment — visit our dedicated page: https://www.inventis.it/en-na/products/video-head-impulse-test-synapsys-vhit
Continued and its subsidiaries provide professional education authored by qualified Subject Matter Experts for continuing education purposes. These materials are intended for educational purposes and do not constitute medical advice or a substitute for individual clinical judgment. Continued is not a clinical healthcare provider; the licensed professional is solely responsible for ensuring that the application of any techniques or information presented is within their legal scope of practice and jurisdictional requirements.
