
Upbeat Nystagmus: A Clinical and Pathophysiological Aid
Upbeat nystagmus is an important clinical sign that may provide valuable insight into central vestibular and brainstem–cerebellar dysfunction. Although it can sometimes be asymptomatic, it is often associated with oscillopsia, diplopia, postural instability, and balance disturbances. In this interview, Dr. Vincenzo Marcelli discusses the clinical presentation of upbeat nystagmus, the underlying pathophysiological mechanisms, and its relevance for lesion localization, diagnosis, and therapeutic decision-making.
DEFINITION AND CLINICAL CHARACTERISTICS
AudiologyOnline: Dr. Marcelli, what is upbeat nystagmus and how does it typically present clinically?
Dr. Marcelli: Upbeat nystagmus (UBN) is a form of central nystagmus characterized by a slow downward drift of the eyes followed by a corrective upward quick phase (Figures 1 and 2).
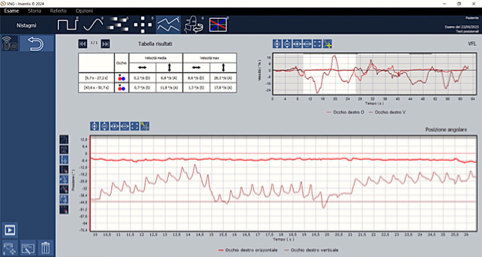
Figure 1. AT, 67-year-old male. Spontaneous upbeat nystagmus due to thiamine deficiency in patient with Wernicke encephalopathy.
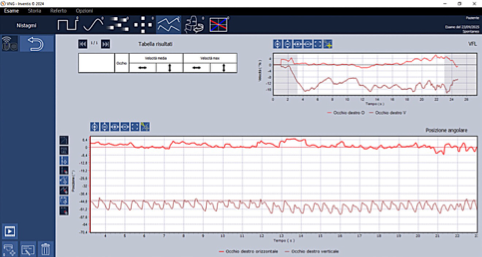
Figure 2. GDB, 61-year-old female. Very strong spontaneous upbeat nystagmus in acute medullar stroke.
UBN may occur spontaneously, be gaze-evoked, or be influenced by head or body position. Clinically, patients frequently report symptoms such as oscillopsia, meaning the illusory movement of the visual environment, vertical diplopia, postural unsteadiness, or balance disturbances. In some cases, however, UBN may remain asymptomatic and may be discovered incidentally during routine neurological or vestibular examination.
UBN is typically associated with lesions affecting the central vestibular pathways, particularly those located within the brainstem and cerebellum. Possible etiologies include ischemic or hemorrhagic stroke, demyelinating diseases such as multiple sclerosis, neoplasms, structural malformations such as Arnold–Chiari malformation, neurodegenerative conditions, and vestibular-cerebellar dysfunctions. The localization of the lesion often correlates with the specific circuitry involved in vertical gaze holding and vestibular integration.
The clinical hallmark of upbeat nystagmus syndrome is oscillopsia, perceived as vertical motion of the visual field due to involuntary eye movements. This occurs because the slow phase of the nystagmus shifts the retinal image downward without a corresponding motor command, known as an efference copy. This mismatch can create the illusion that the visual scene is moving. Interestingly, the perceived illusion is often less intense than the actual eye movement might suggest, possibly because of a central reduction in visual motion sensitivity acting as a compensatory mechanism to minimize visual discomfort.
A secondary consequence of oscillopsia is postural imbalance, particularly along the sagittal plane. The vestibulo-spinal reflex, activated to compensate for the perceived backward body tilt caused by the downward eye drift, may induce anterior–posterior sway or retropulsion. In other words, the body reacts as if it were tilting backward, even in the absence of actual motion, resulting in inappropriate forward leaning or instability. However, this compensatory pattern may vary, and some patients may paradoxically exhibit backward falls, similar to those observed in downbeat nystagmus.
PATHOPHYSIOLOGICAL MECHANISMS
AudiologyOnline: What are the main pathophysiological mechanisms underlying upbeat nystagmus?
Dr. Marcelli: Upbeat nystagmus arises from an imbalance between the neural systems that control upward and downward vertical eye movements. Since gravity naturally promotes a downward drift of the eyes, upward gaze requires tonic facilitatory activity from specific excitatory pathways. When these systems are disrupted, the gravity-facilitated downward drive becomes unmasked, resulting in the nystagmus observed clinically.
Several pathways and anatomical structures are particularly relevant.
1. Crossing Ventral Tegmental Tract - CVTT
The crossing ventral tegmental tract is a key excitatory pathway involved in upward eye movements. It originates in the superior vestibular nucleus, crosses in the pons and midbrain, and terminates in the oculomotor nucleus, cranial nerve III.
The superior vestibular nucleus receives afferent inputs from several structures, including the anterior semicircular canals, the otolith maculae, the flocculus, and caudal medullary structures such as the nucleus of Roller and the intercalated nucleus of Staderini.
Functionally, the CVTT acts as an anti-gravity system. It continuously modulates oculomotor output according to head orientation and gravitational input, particularly from the otolith organs. Lesions affecting the CVTT, or its upstream modulators, impair upward gaze facilitation. This leads to a relative dominance of downward drift and ultimately results in upbeat nystagmus.
Data from altered-gravity experiments, including spaceflight and parabolic flight studies, support the existence and functional importance of this pathway in vertical gaze stabilization.
2. SVN–RN/SIN–Flocculus Feedback Loop
Another important mechanism involves the feedback loop between the superior vestibular nucleus, the nucleus of Roller, the intercalated nucleus of Staderini, and the flocculus. This loop regulates tonic output from the superior vestibular nucleus through inhibitory and excitatory interactions.
The nucleus of Roller is located near the hypoglossal nucleus. It receives excitatory projections from the superior vestibular nucleus and sends inhibitory output to the flocculus. The flocculus, in turn, inhibits the superior vestibular nucleus. Lesions of the nucleus of Roller may therefore lead to floccular disinhibition, excessive suppression of the superior vestibular nucleus, and ultimately upbeat nystagmus due to impaired activity of the upward gaze muscles, particularly the superior rectus and inferior oblique.
The intercalated nucleus of Staderini is located adjacent to the dorsal vagal nucleus. It appears to function similarly to the nucleus of Roller, sharing inputs and outputs with the flocculus and possibly contributing to vertical gaze holding. Upbeat nystagmus has been documented in lesions involving this nucleus, secondary to stroke, multiple sclerosis, and brainstem cavernomas. However, some debate remains as to whether the intercalated nucleus of Staderini is directly involved in gaze holding or whether it primarily modulates tonic vestibular activity.
3. Paramedian Tract Cell Groups
The paramedian tract system consists of small nuclei located along the midline of the medulla and pons. These structures receive input from premotor gaze centers and project to the cerebellar flocculus, paraflocculus, and vermis.
They act as relay and integration hubs, transmitting efference copies and eye-position signals to the vestibulocerebellum. In particular, the nucleus pararaphales relays vertical gaze information from the interstitial nucleus of Cajal to the cerebellum. Lesions involving this nucleus may produce upbeat nystagmus or gaze-evoked vertical nystagmus.
4. Brachium Conjunctivum
The brachium conjunctivum has historically been considered part of the excitatory pathway for upward gaze, projecting from the superior vestibular nucleus to the oculomotor nucleus. However, its distinct role has been questioned, as it closely overlaps anatomically with the crossing ventral tegmental tract.
Lesions confined to the brachium conjunctivum tend to produce downbeat nystagmus or gaze-evoked downbeat nystagmus, rather than upbeat nystagmus. This suggests that the brachium conjunctivum may not be a primary facilitator of upward gaze.
In some cases, upbeat nystagmus associated with lesions in the brachium conjunctivum region is likely due to concurrent involvement of the cerebellar vermis, rather than to damage to the brachium conjunctivum itself.
5. Medial Longitudinal Fasciculus - MLF
The medial longitudinal fasciculus is a critical pathway for vestibulo-ocular signals, particularly in the vertical plane.
Clinical studies in patients with MLF lesions show that upward vestibulo-ocular reflex gain is often relatively preserved. This suggests the presence of extra-MLF pathways, such as the crossing ventral tegmental tract, involved in upward gaze control.
Patients with MLF lesions commonly exhibit upbeat gaze-evoked nystagmus. This supports the hypothesis that MLF damage deprives the interstitial nucleus of Cajal, which acts as a vertical neural integrator, of the vestibular input required for stable vertical gaze holding.
Upbeat nystagmus due to MLF lesions probably results from selective involvement of upward gaze fibers, with relative sparing of the downward vestibulo-ocular reflex circuitry.
TREATMENT OPTIONS
AudiologyOnline: What treatment options are currently available for patients with upbeat nystagmus?
Dr. Marcelli: Management strategies for upbeat nystagmus may be either etiology-driven, focusing on the treatment of the underlying condition, or symptomatic, with the aim of reducing nystagmus intensity and its visual consequences.
First-line pharmacological options include baclofen, 4-aminopyridine, also known as 4-AP, and memantine. These medications may be used individually or, when monotherapy is insufficient, in combination.
Carbamazepine, although less commonly used, has also shown occasional benefit in selected cases.
Ultimately, the choice of therapy should be tailored to the individual patient, taking into account the presumed lesion site, clinical tolerance, and response to treatment.
CONCLUSION
AudiologyOnline: Why is recognizing upbeat nystagmus clinically important?
Dr. Marcelli: Upbeat nystagmus serves as a distinctive clinical marker of dysfunction within the brainstem–cerebellar networks responsible for upward gaze control.
Most commonly, it reflects disruption of circuits such as the crossing ventral tegmental tract and the superior vestibular nucleus–nucleus of Roller/intercalated nucleus of Staderini–flocculus loop. These circuits normally integrate vestibular, visual, and gravitational inputs to maintain vertical ocular stability.
Recognizing the affected anatomical pathway is therefore essential not only for accurate lesion localization and diagnosis, but also for guiding appropriate therapeutic strategies aimed at restoring visual and postural stability in affected patients.
Resources for More Information
For clinicians interested in further exploring vertical nystagmus, Dr. Marcelli has also published a related AudiologyOnline interview on downbeat nystagmus, offering a complementary perspective on its clinical presentation, pathophysiological mechanisms, and diagnostic relevance. Access the interview here.
For more information about Inventis, visit https://www.inventis.it/en-na


V. Marcelli, MD
Dr. Marcelli holds the position of Professor at the Faculty of Medicine and Surgery, University of Naples "Federico II". For several years, he has been engaged in scientific activities as a speaker at conferences, courses, seminars, masterclasses, distance learning programs, lectures, and lessons. He is also an author of articles in scientific journals and serves as a reviewer for articles in the field of Audiology and Vestibular disorders at the local, national, and international levels.