Welcome to today's seminar on Oticon Medical's Ponto Bone Anchored System. Some of this information may be new to you, and some may be a review if you are an experienced bone anchored system audiologist. Either way, it is nice to refresh some of the concepts and science behind these devices, so I hope you find this information useful.
Today we will talk about some concepts of osseointegration plus an overview of the surgical procedure. I want to also introduce Oticon Medical, and talk about who we are and how we came about entering the bone-anchored hearing aid world. We will also discuss an overview of the Ponto System.
As I said, many of you may already know this but let's review because I think it is very important to have a solid understanding of how bone osseointegrated implants came into existence. Professor Brånemark has been in the field since the inception bone implants of any kind. He was the one who first introduced the term osseointegration, which was based on his work with animals and orthopedics. Andres Tjellstrom was the medical physician who first described the surgery more than 30 years ago. Much of the bone-anchored technology originated in the dental field. The first bone-anchored patient was a dental patient in 1965. The first Baha patient was implanted 25 years ago in 1977. This procedure became academically accepted in 1983 and became the standard of care in 2005. Oticon Medical's first Ponto patient was implanted in 2006.
Bone anchored implants are very safe and effective. We have seen a 94% success rate, which translates to all the people who are able to use the system and do not have any type of system malfunction, or in more descriptive terms, when devices perhaps fall out. This is a true possibility and that is described in the literature. The literature also explains that there is about a 4% failure rate due to trauma to the implant or abutment site. Even though the equipment is well inside the bone, if you hit the percutaneous abutment hard enough, you could potentially dislodge it from the skull. There is another 3% failure rate due to infection or possibly a skin overgrowth. A skin overgrowth can often be corrected through a surgical procedure. In these cases, it is not technically a system "failure," but those are things that can happen. In essence, we have proven that auditory bone anchored hearing systems are both safe and effective.
What Influences Osseointegration?
The most important factor by which osseointegration is achieved is the biocompatibility with titanium metal. Titanium is actually very compatible with bone. Professor Brånemark was instrumental in determining this many years ago. The implant design is a macrostructure. Figure 1 shows a close-up picture of the bone integrating with the surface of an implant. The angular structure is such that the bone grows into the grooves of the implant. The microstructure is the implant surface as well as any oxidation that is put on the titanium.
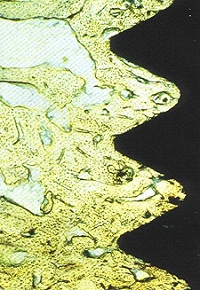
Figure 1. Bone integrating with the surface of an implant.
Titanium has certain oxidation properties that allow osseointegration with the bone. When I help support surgeons in training for these systems, I try to emphasize that whether or not an implant will fail is highly dependent on the surgery itself. If the surgeon is not using certain techniques, one of which is using copious amounts of fluid during the surgery, there is a potential of heating up the bone so much that it will kill the osteocytes in the bone. So the surgical technique is very important. Additionally, we cannot load the abutment and surgical site with pressure before it is ready. We will talk about this in more detail.
While there are other concepts of osseointegration, we use a certain surface that has been well proven and shown to be effective. There are other implant systems that have new services but no control tests that show that any other surface is more beneficial than what we are currently using (Palmquist, Omar, Esposito, Lausmaa, & Thomsen, 2010). We do know that rougher surfaces could possibly cause peri-implantitis, which is an infection. When that happens, you might have what we call bone resorption, where the bone is actually growing away from the titanium implant itself. When this occurs, you are not going to get osteointegration. Rougher surfaces have shown a potential increase of bacterial growth. These rougher surfaces need to be kept away from the upper portion of the implant so there is not an infection at this site. At Oticon Medical, we use micro threads in the hope that we can reduce that bone resorption so the bone does not come away from the implant itself.
Figure 2 is a picture of our implant and abutment. You can see that the upper part of the implant is very smooth. Then beneath are the micro threads. We use the micro threads to try to increase titanium contact to the bone.

Figure 2. Oticon Medical bone conduction hearing system implant.
We have increased the length of the shaft on the abutment so it is a smoother surface. By using a smoother surface and a longer shaft, we are hoping to support the skin itself if it is growing. We have a 6 mm and a 4 mm implant (Figure 3). If the skin does start growing up, we help to support it by the smooth shaft on the abutment itself. We still obviously advocate that the subcutaneous tissue is reduced to decrease any type of movement of the skin against the abutment which can cause irritation. The 9 mm abutments are becoming more popular for some doctors who are not taking as much subcutaneous tissue out as they used to. Thickening of the skin around the abutment can occur in some patients. We have seen that over time, although I will tell you I have seen it less and less. As surgeons become more experienced in the field, they seem to have learned from past surgical approaches.
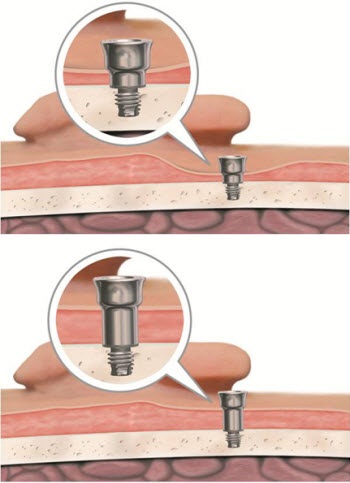
Figure 3. 6 mm abutment with extended collar (top) and 9 mm abutment with extended collar (bottom).
Surgical Aspects
The surgical procedure is an important aspect for audiologists to know, because when patients start having problems with their implant site, oftentimes, as the audiologist, you might be the first one to see them, especially if it is beyond their post-surgical healing time. A dermatome and flap surgery is the more popular procedure where doctors are using what we call a linear incision (Figure 4). The linear incision goes either vertically or horizontally almost like a box. Then the skin is retracted outwards and the soft tissue is taken out. The incision is made at about 55 mm posterior to the opening of the external auditory canal, which is at about 10:00 or 2:00 relative to a clock, for right and left ears, respectively. Sometimes doctors will put it almost to the tip of the pinna depending on the patient.
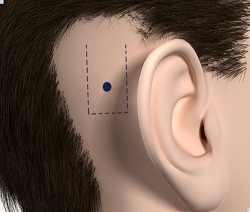
Figure 4. Linear incision site behind right pinna.
In this case (Figure 5) we have used the dermatome and the skin flap has been retracted. When surgeons take out the subcutaneous tissue, it is removed down to the periosteum. The periosteum is a membrane that covers the skull surface, and it provides blood and nourishment to the skin flap. It is very important that the periosteum is not taken off, except where the implant is actually going to be implanted. The subcutaneous tissue is removed at an angle so that the skin flap will rest down in the recess on the bone without any restraint.
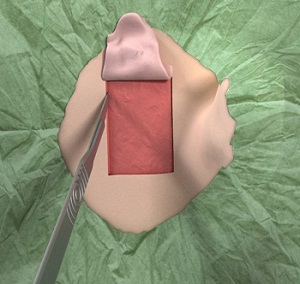
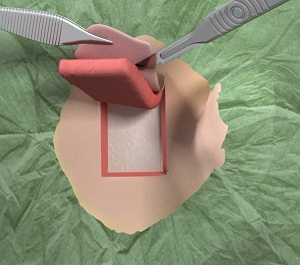
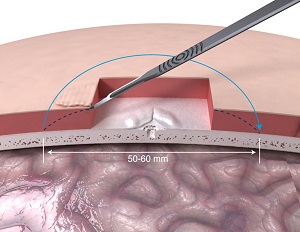
Figure 5. Skin flap incision (top) and subcutaneous removal (middle) down to the periosteum. Subcutaneous is cut at an angle to allow the skin to rest smoothly over incision (bottom).
Once the skin flap is prepared, the surgeon takes a guide drill and drills 3 or 4 mm in depth (Figure 6). In most situations, you are going to use a 4 mm implant for adults and for older children. The guide drill tells us how deep we can go. Once the length is drilled, the surgeon uses the same length but then widens the hole with a countersink (Figure 6). Copious amounts of irrigation are used during the drilling.
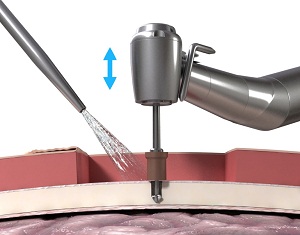
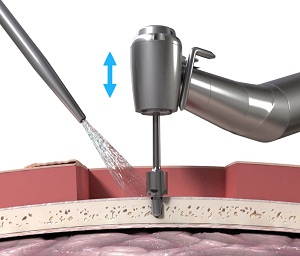
Figure 6. Drilling with guide drill (top) and the countersink (bottom).
The next step is using the abutment inserter. It is very important from this stage that no one makes physical contact with the implant itself. Titanium is what we call a scavenger metal. Scavenger metals pick up dust and debris from other surfaces, so it is very important that the abutment itself does not come in to contact with anything other than bone. If it is contaminated, there is a possibility that it will not integrate appropriately.
On a torque setting of somewhere around 35 N/cm2 we are going to insert the fixture into the prepared bone at a much slower speed (Figure 7). Once it gets to the appropriate torque then it will stop automatically, and then this is lifted right off the abutment. A biopsy punch is then made in the skin flap, and, if you are using a linear incision, you are going to suture the incision around the abutment itself.
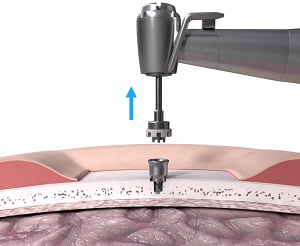
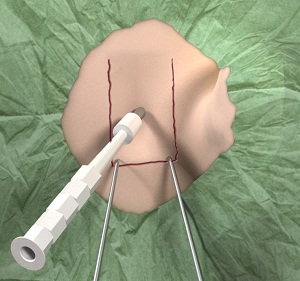
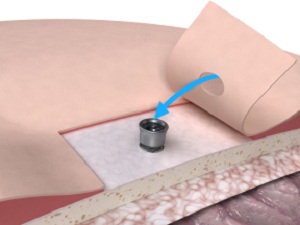
Figure 7. Attachment of the abutment (top) and biopsy punch (middle/bottom).
Once the incision has been sutured, a healing cap is placed over the visible abutment (Figure 8). The healing cap is important. Then Xeroform or Allevyn is placed over the surgical site, which acts as a wound patch. This wound screen allows the skin to stay on the periosteum; we do not want any hematomas. That patch usually stays on about 7 to10 days. After that time period, the patch and healing cap are taken off and the site is left open.
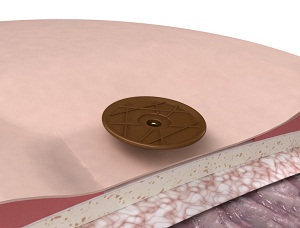

Figure 8. Healing cap and Allevyn patch placed over surgical site during the healing period.
A one-stage procedure, as I just described, is the placement of the implant, the abutment and closure of the skin flap in adults and older children, maybe 10 years of age or older. A two-stage procedure would be used on pediatric patients who are at least five years of age. The first stage consists of the placement of the implant, and then a cover screw is placed, all under the skin, and the site is sutured. About six months later in the second stage, the implant is exposed. The skin flap and periosteum are prepared as we talked about in the one-stage procedure. You let it heal for another two weeks before fitting the sound processor. For many years, doctors were very cautious in implanting young children, but I think surgeons are now finding they can do this successfully. Even with children as young as ten years of age they may do a one-stage procedure.
As an audiologist, we may be involved in the post-operative care, especially if that patient comes to you for fitting or follow-up and they are having problems with the surgical site. Obviously, you will refer them back to the doctor, but your role may be to help them explain what they need to do post-operatively, although usually nurses take care of this and provide the instructions. To reduce any possibility of skin infection, you need to clean the area on a daily basis. Each sound processor includes an extra soft toothbrush that will clean around the abutment as well as in the abutment itself. The sound processor is cleaned with a dry cloth or baby wipe to remove any potential dirt or debris that can accumulate.
Oticon Medical Overview
If you are familiar with Oticon hearing aids, you are going to be very pleased with your ability to program the Oticon Medical devices because the software is Genie Medical and is very similar to Genie. Oticon Medical uses state-of-the-art product development. I think Oticon has always been well known for its leadership in developing sound strategies and processes that work very well. The Ponto Pro uses the RISE platform. The design itself has been well thought out. We use a right and left processor because we believe that is the best way for directionality. We have very innovative improvements. Oticon itself has been in the business for more than 100 years and we have a very dedicated team of scientists and engineers who manufacture the systems.
Oticon Medical is a separate company in the William Demant Holding family. So although we share a family name, we maintain a separate business from Oticon, Inc. Jes Olson is our CEO, and he is based in Denmark. Our headquarters are in Götenburg, Sweden, which is the place for osteointegrated implants. We also have subsidiaries in London, Sweden, the United States, Netherlands, Germany, France, Canada, and Latin America. As we continue to grow we will be bringing a headquarters to Latin America.
The history of temporal bone implants started back with Nobel Pharma/Nobel Biocare, which manufactured dental implant systems. They spun off that portion of their business and opened their own bone anchored and cranial-facial division called Entific Medical Systems. Entific was acquired by Cochlear Limited in 2005. We acquired the bone-anchored technology from Patrick Westerkull of Otorix, who left Entific to develop his own system. He actually developed the Baha System with the implant years ago. So we have a really good history in this space. The first patient was implanted in 2006 with our implant, and in 2007 we had the first use of our coupling system, which is unique. The Ponto sound processors were four years in development before they came to market. In September of 2009 we then launched the Ponto System.
We got clearance in November of 2008 for the implant and the abutment. And then in 2009 we got clearance from the FDA for the Ponto Pro sound processor. Just last year we got clearance for the Ponto Pro Power sound processor, which is indicated for patients equal to five years of age or older when they are implanted. Obviously, a child younger than five years of age can use our system on a headband, but not be implanted. The Ponto Pro sound processor is indicated for patients with mixed or conductive hearing loss as well as for patients with single-sided deafness.
The Ponto System is an osteointegrated bone conduction implant. It is a direct competitor to the Baha System. We have full audiology and surgical support and a dedicated customer service team.
Oticon felt, based on the hearing aid technologies that they have developed over the years, that we could bring in new technologies to bone anchored systems. Like cochlear implants, the determining factor if the patient is going to hear well is really in the sound processing of the external sound device. It is very important to have a well-proven abutment and implant system, but the electrical processing is taking place in the sound processor itself. That is where Oticon has brought quite a bit of exciting technology to the field of osteointegrated implants. We also believe that we can bring aesthetics to the bone-anchored system. I do not think has been as important as it is now.
Of course, we have integrated the RISE platform, which improves performance in difficult listening situations. The sound processor has nano-coating for people who lead active lifestyles and need the moisture protection. We knew it needed to be durable, reliable, discrete and easy to use. The Ponto is ergonomic. I visited Denmark last year where they perform all the quality control testing for our products and processors. This includes drop tests, impact durability, wear and tear and temperature testing. That is why it took four years to create a reliable processor. It had to be durable before we actually released it into the market.
The abutment design is very important to us. Cochlear's abutment design is one where the processor fits inside the abutment itself (Figure 9). Our processor goes around the outer edge of the abutment (Figure 10). We felt the snap-on around the outside improved the durability, sound transmission and safety tension. Many patients have also said that it is much easier for them to put on than the snap coupling. We also feel our coupling system protects the mechanical transducer on the underside of the sound processor. Because of changes to Cochlear's system, we no longer are able to snap or couple to devices each other's abutments since September of 2009.

Figure 9. Cochlear abutment and processor configuration.

Figure 10. Oticon Ponto abutment and processor configuration.
Many patients have a hard time putting the processor on at an angle. If you do not put this on at an angle you have a real possibility of this damaging the transducer on the other side. With Oticon's coupling design, we have eliminated that potential problem of damaging the transducer when the patient is putting the processor on, even if they put it on directly. We still advocate that you put it on at an angle, but even if the patient decides to put it on directly the coupling system will protect the transducer by hitting up against the body of the sound processor instead of the mechanical transducer.
Ponto Pro
The features of Oticon Medical's Ponto Pro include a split directional system, tri-state noise management, speech guard, feedback management, wind noise reduction, 10 channels, and the Genie Medical Fitting Software. The implant comes in two sizes in length: 3 mm and 4 mm. The determination of whether the surgeon uses 3 mm or 4 mm has to do with skull thickness. A 5-year-old child has a skull thickness of about 2 mm, maybe 3 mm. Most doctors try to put in at least a 4 mm implant because 4 mm is the preferred length for optimal osteointegration. I know 1 mm does not seem like much, but it does make a difference when you talk about temporal bone implants.
The diameter of our implant is 3.75 mm. Cochlear has a wider one now, but if you look at the literature, this diameter has been maintained to be safe and effective in long-term studies. Our abutment has micro grooves to increase the titanium to bone contact. The shaft tries to keep the skin from growing up along the sides of the abutment. The smooth surface supports that skin. The abutment is designed to make sure that moisture or fluids that come from the top of the abutment are not going to be released onto the skin surface around the implant and the abutment connection. We have what is called a conical seal. This has been tested to about 6 meters where, when fluid is forced down in, it does not release onto the surface of the skin. By doing that, we reduce leakage and minimize the growth of bacteria around the abutment seal.
Our coupling system is spring loaded, so the abutment will actually widen as you put it onto the head of the abutment and then tighten around the abutment. It is a very tight connection, but you can easily take it on and off without difficulty.
We have several surgical implants (Figure 11). We have a 6mm abutment that can be ordered separately from the implant. Additionally, the same 6mm abutment can be placed on a 3mm implant or 4mm implant. The latter is probably the most widely used one. As I said previously, some doctors now have made the determination that they do not want to take out a lot of subcutaneous tissue. With that being said, we needed to somehow try to support these patients so we developed a 9mm abutment which is longer than the other system. In this case, you can potentially take out a minimal amount of subcutaneous tissue, but still have this area exposed through the skin. The 9mm abutment only comes on a 4mm implant. We cannot put it on a 3mm implant. The torque of the extended length on a 3 mm implant has the potential to make the implant fail.
We also have an angulated abutment. This would be for the case where the implant does not or cannot sit perpendicularly with the skull. If the implant is not in perpendicularly, you have the potential for the sound processor to sit at an angle, which causes the processor to come in contact with the head and cause feedback. In these cases, you can unscrew the traditional abutment and use the angulated abutment which gives about a 10-degree angle to keep the abutment off the skull surface. For children, you can put in the implant during the first stage and then screw the abutment on after the second stage when ready.

Figure 11. Array of abutments offered in the Oticon Medical bone anchored system.
Ponto, Ponto Pro, and Ponto Pro Power Sound Processors
Oticon Medical has a complete family of sound processors. All Ponto processors come in white silver, chroma beige, mocca brown, and diamond black (Figure 12). The Ponto Pro Power is a bit thicker than the Ponto and Ponto Pro. Our power transducer obviously is going to be a little bit bigger, so to make it a little bigger we had to make it a little bit thicker. It is still a very ergonomic design. Our processors are also specifically designed for left and right directionality.

Figure 12. Ponto line; Ponto and Ponto Pro case design (top) and Ponto Pro Power (bottom).
Who is a Candidate?
Patient indications and fitting ranges are going to be very similar to what is out there already. Conductive and mixed components were the first indication ever explored by bone conduction devises. Single-sided deafness became approved in 2002. For patients with conductive or mixed hearing loss who are not appropriate candidates for surgical correction of the loss, are unable to use conventional air conduction hearing aids or bone conduction hearing aids on a tight headband, a bone anchored hearing system might be appropriate. We certainly have seen many patients with old bone conduction headbands that cause an indentation of the head up against the mastoid bone. It can cause irritation to the point where some patients have a breakdown of the ski, which is a potential of any transcutaneous system.
The audiologic indication for our system is either older than or equal to five years of age when they are implanted. If the child is less than five years of age, they can use the processor on a soft band that we have available. It can be unilateral or bilateral. For the standard Ponto or Ponto Pro, the audiological criteria is equal to or better than 45 dB bone conduction. The indication for the Ponto Pro Power is equal to or better than 55 dB bone conduction pure-tone average at 500, 1000, 2000 and 4000 Hz. We are not as concerned with air conduction as we are with bone conduction for these devices. The Ponto Power has about another 15 dB of head room, which translates to more gain for patients.
For bilateral conductive or mixed configurations, the criteria are essentially the same, but the bone conduction thresholds need to be symmetrical. That is defined as less than a 10 dB difference between ears in the pure-tone average or less than 15dB at individual frequencies of 500, 1000, 2000 and 4000 Hz. We have found if you have an air-bone gap of more than 30 dB the Ponto system is probably a better solution that a traditional hearing aid (Snik, Mylanus, Proops, Wolfaardt, Hodgetts, et al., 2005).
Bone-anchored hearing systems are also indicated for patients with single-sided deafness. Entific Medical Systems brought it to market in 2002. It is implantable, again, for patients who are at least five years of age or older. It is intended to improve speech recognition by overcoming the head shadow effect. These would be patients with single-sided deafness who have normal hearing in the contralateral ear. Normal hearing is defined as 20dB or better air-conduction thresholds. We have to ensure the patient has one completely normal hearing ear. The bone conduction system in this case is for patients who cannot or will not use air conduction CROS hearing aids.
Possible causes of single-sided deafness include acoustic neuromas, poor outcome from stapedectomy, sudden deafness, neurological degenerative disease, trauma, genetics, or Meniere's disease. At Oticon Medical, we have different prescription gain for single-sided deafness patients. Because low frequencies are not affected by the head shadow effect, we have to increase the high frequencies for single-sided deafness in the prescription gain, and that is done automatically through the software.
With Ponto Pro, you are going to get a little more high-frequency emphasis. In some cases, even though patients have a bone line at 20 dB in the good ear, they may prefer the Ponto Pro Power over the Ponto. They may have worn the Ponto and after about a year's time they realize they want a louder sound and more power. The Ponto processor is placed on the side of the head with the dead ear, which gathers sound from this side of the head and then routes it to the good cochlea through bone conduction.
Processor Features
I am not going to spend too much time on features because there will be future sessions covering these in depth. Standard features on all processors include nano-coating for weather resistance against moisture and dirt, smart battery management to optimize battery life, and mobile compatibility.
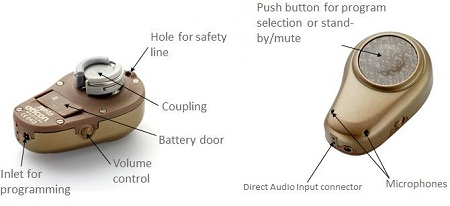
Figure 13. Ponto tactile features.
The picture of the front and back of our processor is in Figure 13. There is no on/off switch; the battery door is used as the on/off control. We have now a tamper-resistant battery door (Figure 14) designed for pediatric patients. It is available on all current Ponto Sound Processors. We cannot retrofit any previous systems that did not have the tamper resistant battery door on it before, unfortunately. It has a raised volume control wheel and inlet for the programming cable. The push button is used for program selection and standby or mute just by pressing this button once. You can use up to four programs in this device. You also have direct audio input connection for external audio devices or FM system inputs.

Figure 14. Tamper-resistant battery door with screw.
The breakdown of programming features can be found in Figure 15. The key features which we will touch on are automatic directionality, tri-state noise management, wind noise reduction, speech guard, and two-stage feedback management. The automatic multiband directionality is unique in that we use three modes in four frequency bands. What is unique is that the program either has no directionality which is omni-directional, split directionality where there is no directionality below 1000 Hz but directionality above 1000 Hz, and then there is full directionality.
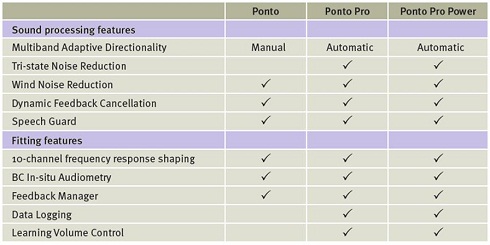
Figure 15. Sound processing features available in three Ponto processors.
We think this split directionality is better for speech understanding. The sound processor is going to be in directionality more frequently. We have determined that most patients will be omnidirectional most of the time. It is going to be in split directionality 20% of the time, full directionality 8% of the time, and omni directionality 72% of the time. By having this split-directionality option, we are allowing patients to have more directionality in more listening situations. We expect improved speech understanding when it is in directionality more frequently rather than having it in omni or full directionality.
Tri-state noise management is the way to control for speech in background noise. The tri-state noise management looks at the speech signal. If there is no speech or noise, the noise management system is going to be inactive. If it recognizes some speech in the presence of noise it will activate the noise management system and will preserve the speech cues and reduce the background noise. Noise without speech is going to reduce the overall sound to improve listening conditions. The advantages of this are that you are going to have less noise in noise-only environments. It will not sound quite as noisy to the patient when they are in traffic or noisy restaurants. The other important feature in the tri-state noise management is that it reduces wind noise, which we have found to be the number one reason for patients to remove the hearing device. In this situation, it forces the instrument into the omni mode. Then as the wind increases it reduces the gain more and more. This helps the patient keep the processor on even as the wind increases.
Speech guard is something that was introduced last July. It is unique to Oticon and Oticon Medical. It is a way to preserve the signal integrity and minimize distortion. I think the best way to look at this is in a graph (Figure16).
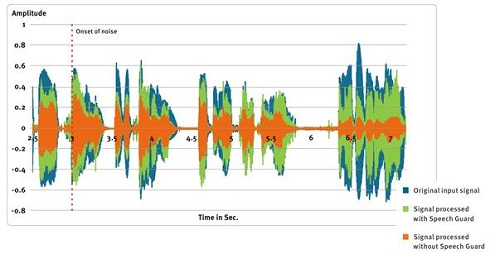
Figure 16. Spectrogram of speech processed with and without Speech Guard.
The unfiltered speech envelope without any type of compression applied is the blue (Figure 16). The orange is with wide dynamic range compression, and the green is with Speech Guard. We use a linear system, so in most situations we do not apply output compression all the time because it will distort the signal. By using Speech Guard, it looks at the speech envelope and is activated based on the presence of very loud transient sounds. It reduces the speech signal instantaneously and then it comes back. When you look at wide dynamic range compression (Figure 16, orange) you can see it takes some time to come out of compression. In this case, we have a much more similar speech envelope compared to what the actual speech envelope is when Speech Guard is activated. It provides improved speech intelligibility when there are sudden loud sounds.
The other feature we have in this system is feedback management. When we introduced the Power Pro device we needed to have some sort of feedback management system. It automatically manages feedback in two ways. It looks at both static conditions and dynamic conditions that can cause feedback. Static conditions are things like vibrations that come off the skull, the angle of the abutment or the placement of the processor. This will be individual for each person. Dynamic conditions can include when a person moves their head, when they get hugged or place their hand near the processor. Each patient has individual feedback curves. We measure these feedback curves and that upper limit is as loud as the sound processor will be allowed to go. We will optimize the volume control without feedback so the patient is able to increase the volume until it reaches that patient's maximum feedback limit, and then it reduces as you turn the volume control down. So it will never go beyond the maximum feedback control curve. By allowing patients to use their volume control all the way, they have optimal listening conditions. However, in some situations there are some things we cannot control, like a spontaneous hug or brush with something close. Dynamic feedback will occur in these situations, so we put in out-of-phase signal which cancels out that feedback whistle. We will talk a little bit more about this in future presentations.
The Ponto is pediatric friendly. We have stickers that children can use to decorate the processor (Figure 17). More importantly, we have a very nice soft band (Figure 18). It is not Velcro, but attaches with a snap fixture and is adjustable. It comes in both unilateral and bilateral configurations. It comes in red, light blue, navy blue, pink, beige, and black. There may even be some adults who may not want to have surgery, and the soft band is a nice option for them. It is very comfortable and latex free. Audiologists love our soft band. We also have the safety line that can attach from the processor to the child's shirt.

Figure 17. Oticon pediatric sticker covers for Ponto processors.

Figure 18. Oticon Medical soft band; unilateral (top) and bilateral (bottom).
As far as accessories go, we have audio adapters, FM receivers as part of the Amigo system, the soft band, demo test rod, headbands, abutment covers and an external telecoil. The telecoil can be used as needed if your patients want to use loop systems or inductive magnetic coupling. To connect to anything like an audio adapter, we use the older three pin system that Cochlear used to use, so that any patients who are able to use our system and already had these devices are still able to use them with our Ponto.
Thank you for joining us today and we hope you have found the information useful. Please contact us at Oticon Medical if you would like more information and visit our course library on AudiologyOnline for other courses on the Ponto system.
References
Palmquist, A., Omar, O.M., Esposito, M., Lausmaa, J., & Thomsen, P. (30 June 2010). Titanium oral implants: surface characteristics, interface biology and clinical outcome. Journal of the Royal Society Interface. Retrieved February 20, 2012, from rsif.royalsocietypublishing.org/content/early/2010/06/26/rsif.2010.0118.focus.full.pdf+html
Snik, A.F., Mylanus, E.A., Proops, D.W., Wolfaardt, J.F., Hodgetts, W.E., Somers, T., et al. (2005). Consensus statements on the BAHA system: where do we stand? Annals of Otology, Rhinology and Laryngology, (S195), 2-12.