Learning Outcomes
- Readers will be able to describe current techniques and tools available to the clinicians when verifying frequency lowering (FL) hearing aid fittings.
- Readers will be able to interpret the measurements discussed in a way that will assist in determining whether to activate FL, on a case-by-case basis.
- Readers will be able to describe a series of steps that can be used to fine-tune FL fittings in clinical practice.
Background
Frequency lowering (FL) devices have been around for decades, offering signal processing designed to improve audibility of sounds for listeners with high-frequency hearing loss. Within the literature, several papers offer a review of the rationale and evidence on FL for managing high-frequency hearing loss (Alexander, 2013b; McCreery, Venediktoc, Coleman, & Leech, 2012; Simpson, 2009). In brief, listeners require access to a broad bandwidth of speech to detect and produce all phonemes. Access to the high-frequency components of speech in particular (e.g., the female /s/) can be limited via conventional hearing aid processing. When combined with an evidence-based fitting procedure, FL technology can help overcome device limitations and improve audibility for some listeners (Bohnert, Nyffeler, & Keilmann, 2010; Glista et al., 2009; Hopkins, Khanom, Dickinson, & Munro, 2014; Wolfe et al., 2010). Although the concept behind such technology has not changed, accessibility has. This relates to the fact that most manufacturers now offer some form of frequency lowering within the many devices available for clinical use. The provision of information to clinicians on how to fit and fine-tune frequency lowering devices is therefore an important topic. This article will focus on electroacoustic verification considerations for fitting frequency lowering hearing aids to children and adults in accordance with the American Academy of Audiology (AAA) guideline (AAA, 2013). The protocol presented includes specific stimuli and fitting steps designed to supplement the AAA fitting guideline (Scollie et al., 2016).
Understanding Frequency Lowering
FL technology can be classified according to type of signal processing used; each having a unique effect on the aided signal (Alexander, 2013a, 2013b; McDermott, 2011; Mueller, Alexander, & Scollie, 2013; Scollie, 2013). FL devices apply digital signal processing to select a high-frequency region of the hearing aid input to be presented at a lower frequency in the output. Types of FL include frequency compression, transposition, translation and composition, for example. These different types can vary according to how the lowering is achieved (e.g., linearly versus nonlinearly) and whether an adaptive versus static amount of lowering is applied to the output signal (this can depend on the presence or absence of a high-frequency weighted input signal, for example). In addition, the hearing aid output for some FL processors includes both the original signal along with the frequency lowered signal; whereas some present an output signal that is narrower in bandwidth than the original input signal. Refer to Scollie et al. (2016) for a more detailed summary of the different types of FL.
Factors to Consider when Addressing Frequency Lowering Candidacy
The protocol presented in this paper considers FL as a means to provide access to high-frequency sounds, when these cannot be provided via conventional amplification. As hearing aid technology advances, it may be possible to amplify a broader frequency response without the use of FL. Some candidacy factors for the application of individualized FL settings include [adopted from the Ontario Infant Hearing Program: Protocol for the Provision of Amplification (IHP, 2014)]:
- The configuration and degree of the hearing loss: Candidacy is more likely if the hearing loss is high-frequency or severe-profound.
- Hearing instrument factors: Ensure the hearing instrument provides an appropriate gain response for the hearing loss. Consider whether the device provides some form of frequency lowering. Candidacy is more likely if the bandwidth of the device is restricted in the high-frequencies.
- Electroacoustic verification (fit to targets): Candidacy is more likely if fit to targets cannot be met across all frequencies, according to a valid fitting approach, and audibility of high-frequency phonemes such as a female /s/ is not possible with conventional amplification.
- Other factors unique to the listener: Candidacy is more likely if the listener and/or caregiver reports difficulty hearing and/or discriminating between high-frequency phonemes such as /s/ and /ʃ/, with conventional amplification.
Verifying Hearing Instruments with Frequency Lowering
As with all hearing aid fittings, routine clinical verification is necessary to ensure that an appropriate amount of gain and output is provided across frequencies. This FL protocol recommends the use of a validated prescriptive formula as the starting point of all fittings. A few additional verification steps are recommended to ensure that an optimal amount of FL is provided. This can help ensure that each listener has access to important speech sounds needed when developing speech and language skills and for daily communication needs.
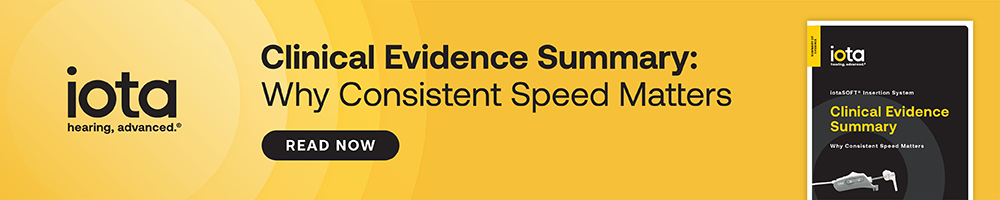
Current clinical guidelines recommend that the fitter maximize the output bandwidth available to the listener prior to activating FL through the use of validated prescriptive targets (AAA, 2013). The fitter can then determine the frequency at which the output of the hearing instrument falls below audibility for a given audiogram, or the MAOF: maximum audible output frequency (McCreery et al., 2014; McCreery, Brennan, Hoover, Kopun, & Stelmachowicz, 2013). In this protocol, we verify the hearing aid with a running speech signal, to determine the MAOF range. Specifically, the MAOF range spans from the point at which the long-term average speech spectrum (LTASS) crosses threshold to the point at which the peaks of speech cross threshold (Figure 1). This range can then be used as a target region in which to place the calibrated /s/ stimulus during verification and fine-tuning of FL (Scollie et al., 2016). A display of peak and valley measurements for the LTASS is needed when identifying the MAOF range.
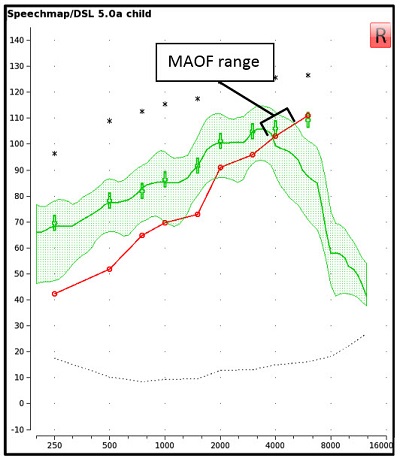
Figure 1. An Audioscan Verifit display of the hearing threshold line, together with the aided LTASS for a standard speech passage presented at 65 dB SPL allows for visualization of the MAOF range.
The aim of this article is to discuss recommended stimuli, a step-by-step verification protocol, and optional measures to assist in the verification of hearing aid fittings with FL. A case example will be used to illustrate each step of the recommended protocol.
Recommended Stimuli
Previously recommended protocols have included two types of frequency-specific speech sounds: Live voice productions of /s/ and /ʃ/ and filtered speech with high-frequency bands of energy (Glista & Scollie, 2009). Live voice productions of speech sounds can be easily measured on the Audioscan® Verifit system and allow for an estimation of audibility and approximation of bandwidth associated with each sound. With this information the fitter could estimate the sensation level and the approximate spectral separation between /s/ and /ʃ/. However, there are limitations to using live voice production of speech sounds. These include the inability to present sounds at a calibrated/known level and the variability associated with repeated measurement due to gender and talker differences. Alternatively, filtered speech signals have been used within the Verifit system which present 1/3 octave bands of energy centered around 3150, 4000, 5000 and 6300 Hz. These have allowed the fitter to use a calibrated level during measurement that is repeatable. These filtered signals are limited in two important ways:
- They may produce measurements that lead to a conservative estimate of audibility due to the 1/3 octave band being narrower than the frication band of naturally produced speech sounds (Scollie, 2013). The presentation level is slightly lower than the level of /s/ or /ʃ/ would be in running speech due to the presentation level being fixed to that of the LTASS at each frequency.
- Filtered bands only allow evaluation up to 6300 Hz, while a female /s/ is typically higher in frequency.
For the reasons discussed above, this article focuses on the use of pre-recorded, calibrated speech signals (/s/ and /ʃ/) that, at the time of writing, have been implemented in the Audioscan® Verifit2 system, and that can be downloaded for use with the Verifit1 or SL systems (https://www.dslio.com/?page_id=166). Note: the principles discussed in this article may also be applied to other verification systems. These signals were created by extracting phonemes from the International Speech Test Signal (Holube, Fredelake, Vlaming, & Kollmeier, 2010) and measuring each fricative’s average spectrum. Synthetic fricatives were created that matched the observed spectra. These fricatives fall close to the peaks of speech and represent an average female production of the fricatives /s/ and /ʃ/ (Scollie et al., 2016). Some advantages of using these new stimuli include the ability to present them at a calibrated level and to estimate hearing aid output of fricatives using an accurate representation of fricatives. This allows for an accurate assessment of the spectral separation of /s/ and /ʃ/ for a given fitting. These signals do not account for variability between talkers, nor do they represent male speech. It is recommended that all digital noise reduction features be disabled when verifying with the calibrated /s/ and /ʃ/ signals to ensure accurate representation of the aided level.
Recommended Protocol for Fitting Frequency Lowering
The following clinical protocol is designed to assist fitters in the verification and fine-tuning of FL hearing aid fittings. A case example has been used in this section to illustrate the recommended fitting protocol. This example is of a 14 year old child, presenting with a sloping, high-frequency hearing loss. A behind-the-ear (BTE) hearing instrument has been fitted to this child using the DSL v5.0 prescription. Test box measures have been completed using an RECD value measured with insert phones coupled to a personal earmold (Moodie et al., 2016). Audiometric thresholds were measured using insert phones coupled to a personal earmold and have been entered into the Verifit2 software. Although only one type of FL has been used in the examples provided, the protocol is intended for use across all types of FL and has been electroacoustically validated with three different types of FL (Scollie et al., 2016).
- Verify the shape and gain of the hearing aid fitting with FL turned off.
Begin by verifying and fine-tuning the hearing aid to optimize the conventional hearing aid fitting. Ensure that the aided speech spectrum meets targets for the chosen fitting prescription and provides a broad bandwidth of audibility (Figure 2).
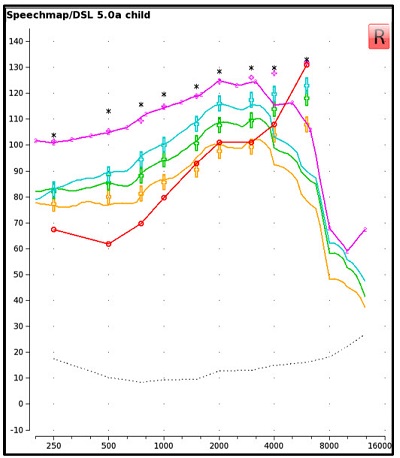
Figure 2. A screen capture of the aided verification results for a hearing instrument fitted to DSL v5.0 targets, without FL active. Measurements are displayed for the LTASS at soft (yellow curve), average (green curve) and loud (blue curve) presentation levels, as well as for the MPO (pink curve).
- Determine candidacy for FL.
In addition to considering the candidacy factors stated above, this step lets you determine if electroacoustic verification suggests that FL may improve audibility of high-frequency sounds, when these cannot be made audible via conventional amplification. Start by measuring the aided response of the /s/ at 65 dB SPL, without FL and with all noise reduction features turned off (Figure 3). Determine if the /s/, including the upper shoulder, is audible and falls within the MAOF range for an LTASS measured at 65 dB SPL. If the measured /s/ falls outside of this range, proceed to step 3 to determine an appropriate FL setting.
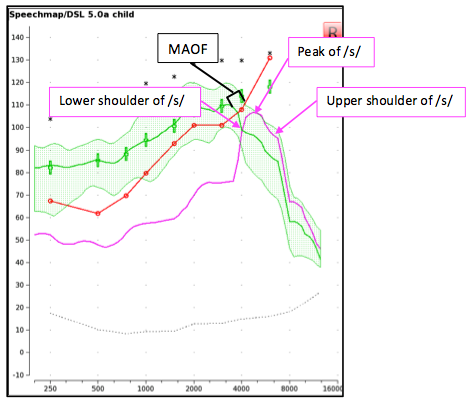
Figure 3. The aided LTASS measured using a presentation level of 65 dB SPL (green). For this case, the /s/ does not fall within the MAOF range and is not audible. This fitting would be deemed a candidate for FL.
For listeners presenting with milder degrees of hearing loss, it may be possible to measure an audible /s/ within the MAOF range without enabling FL. This relates to recent technological advancements resulting in improved high-frequency gain and audible bandwidth via conventional hearing aids. This highlights the need to assess candidacy on a case-by-case basis when FL is first being considered, and to reassess candidacy when providing a new hearing aid fitting. Refer to Scollie et al. (2013) for a case example of a borderline candidate for FL (Scollie, Glista, & Richert, 2013). For this case, outcome measures were used to help determine FL candidacy, together with electroacoustic measurements, while factoring in the candidacy factors discussed above.
- Enable and fine-tune FL.
Start by enabling the default FL setting in the hearing instrument. Measure the aided response for /s/ to determine if the upper shoulder is audible and within the MAOF range of the LTASS presented at 65 dB SPL. Fine-tune the strength of the FL setting until the /s/ is audible and falls within the MAOF range using the weakest possible setting (Figure 4); this setting will likely be associated with the best possible sound quality when considering stronger FL settings in comparison (Parsa, Scollie, Glista, & Seelisch, 2013; Souza, Arehart, Kates, Croghan, & Gehani, 2013). Note: the fitter can leave the /s/ stimulus running when exploring different settings. It is recommended that the fitter choose a setting that allows the upper shoulder of /s/ to reside close to the upper limit of the MAOF range. For hearing losses of greater severity, it may not be possible to achieve full audibility of /s/, especially if the maximum FL setting has been reached.
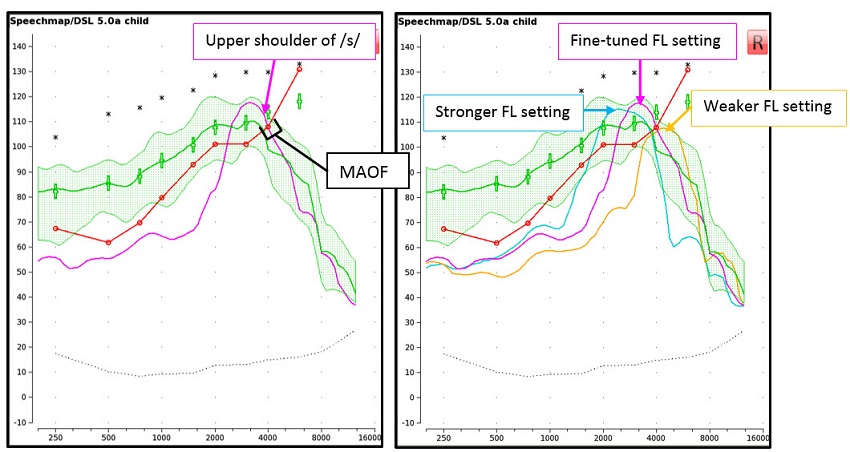
Figure 4. Both screen captures display the aided LTASS measured using a presentation level of 65 dB SPL (green). The LEFT screen capture displays the /s/ (pink) after fine-tuning the FL setting. The /s/ has been made audible and the upper shoulder falls within the MAOF range. The RIGHT screen capture depicts a setting that was considered too strong (blue /s/), the fine-tuned setting (pink /s/) and a setting that was considered too weak (yellow /s/).
- Provide post-fitting support.
Provision of counselling to caregivers and therapists may be important in the event that they are performing listening checks on fittings employing FL, for example. This is because the sound quality of FL fittings may differ from that of conventional hearing aid fittings; this will depend on the hearing loss of the listener and the strength and type of the FL setting used in the fitting (Parsa et al., 2013; Souza et al., 2013). The fitter may choose to alert the person performing the listening check of possible sound quality differences due to the nature of FL technology. As always, it is important to incorporate feedback into follow-up appointments; this may come in the form of feedback from the listener (adults and older children) or from therapists of children enrolled in a program of oral language development. For example, if the listener cannot functionally detect /s/, it may be the case that the fitting needs to be adjusted to provide more gain or output and/or the FL setting may need to be strengthened. Feedback related to /s-ʃ/ discrimination difficulty is discussed below.
Optional Verification Measures
It is possible to make descriptive measures of /s-ʃ/ separation to help with counselling or troubleshooting around feedback concerning “lisping” or “slushy” sound quality, or difficulty with /s-ʃ/ discrimination. In such cases, it may be that too much FL has been applied to a given fitting. To explore this further, it is recommended that the fitter electroacoustically evaluate /s-ʃ/ separation. Start by taking measurements of the /s/ and /ʃ/ for the chosen FL setting and compare the measured responses (Figure 5). In the case where the fine-tuning steps outlined above have been followed, it is likely that the separation between /s/ and /ʃ/ is already maximized. This is because the protocol recommends using the weakest possible FL setting, while maintaining audibility of /s/. In the case where the fitter has fine-tuned to include a stronger FL setting based on user preference, for example, greater /s-ʃ/ overlap can occur (Figure 6). In an example such as this one, it may be possible to provide a weaker setting with greater /s-ʃ/ separation.
This fitting protocol illustrates a method for providing full audibility of /s/. In some cases, the fitter may decide to provide a weaker FL setting (other than what would be recommended by this protocol) in the case where the sound quality associated with a FL fitting is unacceptable to the listener, for example. This may result in reduced audibility of high-frequency phonemes (refer to Figure 4); this compromise between audibility and sound quality can be assessed through the use of the optional measures discussed above, combined with a listening check and feedback from the hearing aid wearer. Consideration should also be given to the idea that some listeners require time to acclimatize to FL fittings in order to achieve maximal benefit (Glista, Scollie, & Sulkers, 2012; Wolfe et al., 2011). Further research is needed to determine if acclimatization time relates to perceived sound quality of FL fittings.
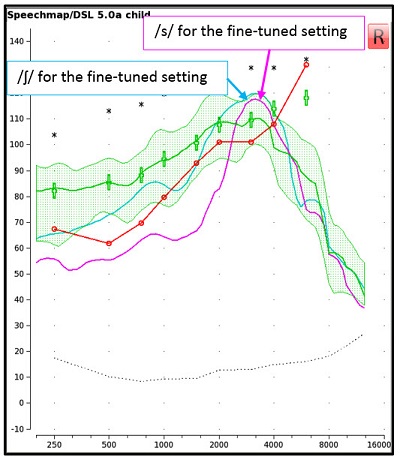
Figure 5. A screen capture of the aided response of /s/ (pink) and /ʃ/ (blue) for a presentation level of 65 dB SPL for the fine-tuned FL setting. The spectrum of /s/ and /ʃ/ are separated in terms of peak levels and in frequency locations at the lower shoulders.
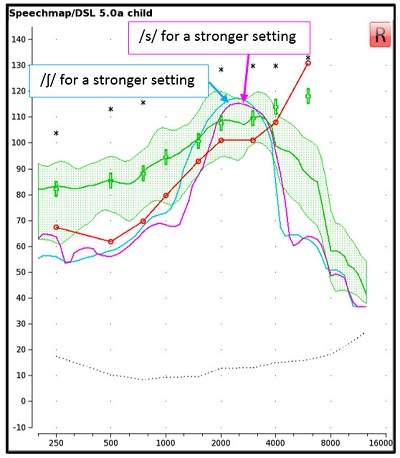
Figure 6. A screen capture of the aided response of /s/ (pink) and /ʃ/ (blue) for a stronger FL setting. The spectrum of /s/ and /ʃ/ for this setting appear more similar in terms of bandwidth and there is less separation of frequency location of the lower shoulder of /s/ versus /ʃ/, compared to the fitting shown in Figure 5.
Summary of Verification Considerations for Frequency Lowering Fittings
This article provides an update on electroacoustic verification considerations for fitting FL hearing aids to children and adults in accordance with the AAA guideline (AAA, 2013). Candidacy factors, verification stimuli and fitting steps are recommended to assist fitters in choosing appropriate FL settings. The overall goal of the outlined protocol is to provide FL fittings employing the weakest possible setting, while improving audibility of high-frequency sounds, in comparison to the conventional setting. Here is a summary of the steps that have been discussed in the article:
- Verify the shape and gain of the hearing aid fitting with FL technology turned off.
- Determine candidacy for FL using a pre-recorded, calibrated /s/ signal.
- Enable and fine-tune FL to the weakest possible setting, providing audibility of /s/.
- Provide post-fitting support.
Pre-recorded and calibrated stimuli available for use with hearing aid test systems such as the Audioscan® Verifit and are suitable in determining candidacy for FL technology. The stimuli discussed in this article (calibrated /s/ and /ʃ/) have been developed and evaluated for use in hearing aid verification using clinically available equipment for fine-tuning of FL technology (Scollie et al., 2016). The fitting protocol presented in this article can provide guidance when deciding whether to activate FL and when judging whether the overall strength of a setting is appropriate.
References
American Academy of Audiology. (2013). American Academy of Audiology clinical practice guidelines: Pediatric amplification. Retrieved from https://audiology-web.s3.amazonaws.com/migrated/PediatricAmplificationGuidelines.pdf_539975b3e7e9f1.74471798.pdf
Alexander, J.M. (2013a). 20Q: The highs and lows of frequency lowering amplificaiton. AudiologyOnline, Article 11772. Retrieved from www.audiologyonline.com
Alexander, J.M. (2013b). Individual variability in recognition of frequency-lowered speech. Seminars in Hearing, 34(2), 86-109.
Bohnert, A., Nyffeler, M., & Keilmann, A. (2010). Advantages of a non-linear frequency compression algorithm in noise. European Archives of Oto-Rhino-Laryngology, 267(7), 1045-1053.
Glista, D., & Scollie, S. (2009). Modified verification approaches for frequency lowering devices. AudiologyOnline, Article 871. Retrieved from www.audiologyonline.com
Glista, D., Scollie, S., Bagatto, M., Seewald, R., Parsa, V., & Johnson, A. (2009). Evaluation of nonlinear frequency compression: Clinical outcomes. International Journal of Audiology, 48(9), 632-644.
Glista, D., Scollie, S., & Sulkers, J. (2012). Perceptual acclimatization post nonlinear frequency compression hearing aid fitting in older children. Journal of Speech, Language, and Hearing Research, advanced online publication.
Holube, I., Fredelake, S., Vlaming, M., & Kollmeier, B. (2010). Development and analysis of an International Speech Test Signal (ISTS). International Journal of Audiology, 49, 891-903.
Hopkins, K., Khanom, M., Dickinson, A.M., & Munro, K.J. (2014). Benefit from non-linear frequency compression hearing aids in a clinical setting: The effects of duration of experience and severity of high-frequency hearing loss. International Journal of Audiology, 53, 219-228.
IHP (Ontario Infant Hearing Program). (2014). Ontario Infant Hearing Program: Protocol for the provision of amplification. Retrieved from https://www.mountsinai.on.ca/care/infant-hearing-program/documents/ihp_amplification-protocol_nov_2014_final-aoda.pdf
McCreery, R.W., Alexander, J., Brennan, M.A., Hoover, B., Kopun, J., & Stelmachowicz, P.G. (2014). The influence of audibility on speech recognition with nonlinear frequency compression for children and adults with hearing loss. Ear and Hearing, 35(4), 440-447.
McCreery, R.W., Brennan, M.A., Hoover, B., Kopun, J., & Stelmachowicz, P.G. (2013). Maximizing audibility and speech recognition with nonlinear frequency compression by estimating audible bandwidth. Ear and Hearing, 34(2), e24-e27.
McCreery, R.W., Venediktoc, R.A., Coleman, J.J., & Leech, H.M. (2012). An evidence-based systematic review of frequency lowering in hearing aids fo school-age children with hearing loss. American Journal of Audiology, 21, 313-328.
McDermott, H.J. (2011). A technical comparison of digital frequency-lowering algorithms available in two current hearing aids. PLoS ONE, 6(7), e22358.
Moodie, S., Pietrobon, J., Rall, E., Lindley, G., Eiten, L., Gordey, D., . . . Scollie, S. (2016). Using the real-ear-to-coupler difference within the American Academy of Audiology pediatric amplification guideline: Protocols for applying and predicting earmold RECDs. Journal of the American Academy of Audiology, 27(3), 264-275.
Mueller, H.G., Alexander, J.M., & Scollie, S. (2013). 20Q: Frequency lowering - The whole shebang. AudiologyOnline, Article 11913. Retrieved from www.audiologyonline.com
Parsa, V., Scollie, S., Glista, D., & Seelisch, A. (2013). Nonlinear frequency compression: Effects on sound quality ratings of speech and music. Trends in Amplification, 17(1), 54-68.
Scollie, S. (2013). 20Q: The ins and outs of frequency lowering amplification. AudiologyOnline, Article 11863. Retrieved from www.audiologyonline.com
Scollie, S., Glista, D., & Richert, F. (2013, December). Frequency lowering hearing aids: Procedures for assessing candidacy and fine tuning. Paper presented at the A Sound Foundation Through Early Amplification conference. Chicago, Illinois.
Scollie, S., Glista, D., Seto, J., Dunn, A., Schuett, B., Hawkins, M., . . . Parsa, V. (2016). Fitting frequency-lowering signal processing applying the AAA pediatric amplification guideline: Updates and protocols. Journal of the American Academy of Audiology, 27(3), 219-236.
Simpson, A. (2009). Frequency-lowering devices for managing high-frequency hearing loss: A review. Trends in Amplification, 13(2), 87-106.
Souza, P.E., Arehart, K.H., Kates, J.M., Croghan, N.B.H., & Gehani, N. (2013). Exploring the limits of frequency lowering. Journal of Speech, Language and Hearing Research, 56, 1349-1363.
Wolfe, J., John, A., Schafer, E., Nyffeler, M., Boretzki, M., & Caraway, T. (2010). Evaluation of non-linear frequency compression for school-age children with moderate to moderately-severe hearing loss. Journal of the American Academy of Audiology, 21(10), 618-628.
Wolfe, J., John, A., Schafer, E., Nyffeler, M., Boretzki, M., Caraway, T., & Hudson, M. (2011). Long-term effects of non-linear frequency compression for children with moderate hearing loss. International Journal of Audiology, 50(6), 396-404.
Citation
Glista, D., Hawkins, M., & Scollie, S. (2016, April). An update on modified verification approaches for frequency lowering devices. AudiologyOnline, Article 16932. Retrieved from www.audiologyonline.com



