Editor's Note: This text-based course is a transcript of the live seminar presented by Casie Keaton, Au.D. for Neuromonics. Please download supplemental course materials.
My name is Casie Keaton, and I am the Clinical Sales Manager with Neuromonics, Inc. Today, we will be reviewing the neurophysiological model of tinnitus, but from a different angle than what is usually presented. We are going to take a look from more of a practical, patient perspective. My hope is that you will come away with a better method of relating tinnitus to your patients, as well as ways in which to better understand what your tinnitus patients are going through. I feel that the best treatment for tinnitus is for patients to fully understand their condition so that they can recognize their role in the treatment process. Our ultimate goal is success with treatment, no matter the treatment modality.
Today we are going to begin with the pathogenesis of tinnitus. We will delve into the tinnitus cycle while relating each step to the patient experience. We will then look at some treatment considerations, not only in terms of the patient with tinnitus, but also concurrent issues facing patients with hearing loss and hyperacusis. Lastly, we will discuss a few patient case studies and review their specific presentations and characteristics.
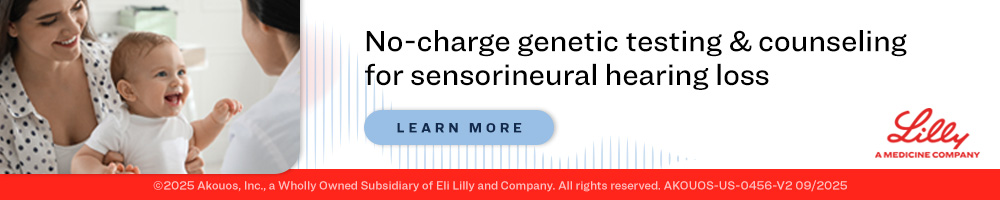
We will begin here with the neurophysiological model of tinnitus. Figure 1 shows a graphic of the tinnitus cycle. To reiterate, when we talk about the tinnitus cycle, we are referring to the tinnitus patient who is having significant quality-of-life issue as a result of his/her tinnitus. These would be patients who would say, "I am not sleeping. I may only get three or four hours a night, and that is interrupted sleep at best. I am missing deadlines at work. I am having a lot of difficulty concentrating. I cannot read for pleasure anymore. I sit and read the same page over and over again because I am not able to focus on the words on the page."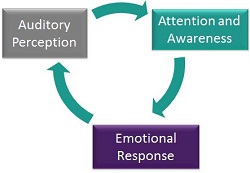
Figure 1. Tinnitus cycle.
You will see some relationship difficulties between spouses or with children because the patient spends so much time on edge. They do not always respond the way that they or their partner wishes they would. This can be life-altering, and something we need not take lightly, as I am sure none of you do.
With the severe tinnitus patient, there are three elements at work. One has to do with the auditory input, the second with attention or awareness, and the third being the emotional response. In my opinion, the emotional response can often be the heaviest-weighted aspect of the cycle and the one that has the most impact on the patient. I am sure those of you who see tinnitus patients would agree.
Auditory Input
We know that most of these patients do have evidence of damage to the auditory system, resulting in a hearing loss and the tinnitus. As part of your tinnitus evaluation, I recommend completing otoacoustic emissions (OAEs) as well, because there are a percentage of these patients who will not show hearing loss on the audiogram, but the damage will be evident by the OAEs. That can better help your patient to understand this aspect of the tinnitus cycle.
As you know, the hearing loss can range from very mild all the way to severe. Nonetheless, the brain, being the magnificent structure that it is, knows that it is not getting the input that it should. It is either getting a bad message or, in some cases, no message at all. The auditory centers are starving for input, and this triggers a compensation mechanism in the brain. This leads to over-excitation of neurons, and it is there that the tinnitus signal is generated (Shim, Kim, Park, Lee, Yoon, Ki, et al., 2009).
For your patients in the office, I think the best way to get this idea across is to help them understand the damage to the auditory system. You will be reviewing the audiogram with them, going over the OAEs, but then help them understand that the brain is merely trying to fix this problem, and, in so doing, the tinnitus signal is generated. Most patients are able to identify with that and understand.
I know the neurophysiological model can be such an abstract concept to learn for the first time, and the terminology that we use can be so detailed that the patient becomes lost and has that glazed-over look when you try to explain it. That is definitely not what we want! Much of the fear comes from not understanding the cause of tinnitus. If the patient can understand the mechanisms behind the tinnitus, it can go a long way in helping you increase your clinical outcomes.
I want to focus on the patient that is straining to hear, and how important that is in your clinical decision-making. A study published by Heller and Bergman (1953) took several college students with normal hearing, put them in an anechoic chamber, and then asked them what they heard. Almost 94 percent of them heard some kind of buzzing, ringing or hissing in the absence of sound. This is believed to be their own underlying hum. If you have a patient who is straining to hear or who has more significant demands on their day-to-day hearing, this can only serve to exacerbate their tinnitus. This point is important to drive home to your patients. You cannot overlook those demands on their hearing.
You will find that the net effect of this problem is compounded. Not only will there be an increased perception of tinnitus, but also it can lead to loudness tolerance issues and hyperacusis, because you are further starving the auditory system for input. The brain is searching for that input, and in doing so, the tinnitus is wound up. The individual's sensitivity to sound is heightened as well. That is why it is critical to address any communication needs when you are considering treatment for these patients. You cannot take a single-pronged approach. You have to look at these patients globally and make sure that you are addressing all of their needs for treatment.
Figure 2 shows the auditory compensation mechanism. This illustrates the increased central gain where a low-level sound comes in to the auditory system, and is perceived as a much louder sound neurologically. I find this condition can be extremely debilitating on its own, regardless of the impact of the tinnitus. It is definitely something that we need to address clinically when seeing these patients.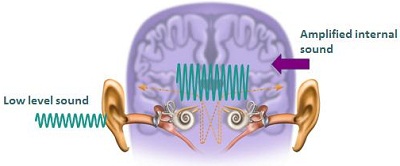
Figure 2. Auditory compensation mechanism.
Now is a phenomenal time in the world of tinnitus and tinnitus treatment, because there is more research being done today than ever before, and we know so much more about it than we have in years past. We now understand tinnitus to be more of a neurological phenomenon, with an auditory component. The auditory piece is an important player. However, the higher-processing neurological centers are more in control of a patient's tinnitus.
Many years ago as a treatment for tinnitus, the patient's eighth nerve was severed. Not only did the tinnitus not go away; in many cases it became much, much worse. Consider for a moment the lengths that these patients went to in order to achieve some relief. There are patients who are willing to sacrifice their hearing, saying, "I am willing to not hear any more if you can just help me with this tinnitus perception." Thankfully, this treatment of severing the nerve is no longer done, but we know from this that the auditory centers are not the sole generators of tinnitus. Neurological centers are largely the control centers for a patient's tinnitus perception.
Many of the tinnitus studies have been correlated to phantom limb pain studies. This is where a particular limb has been amputated, and the patient still perceives pain there, although the limb is missing. What is understood to occur is that the brain realizes there is no longer input from that particular limb, so it begins seeking for that input and trying to compensate for it. It is that compensatory mechanism in the brain where the pain is generated. Likewise, the brain views tinnitus as a phantom auditory perception. I think this example is a very good one to relate to patients. I think they can understand it; it helps take it out of the abstract terms and put it into more realistic terms that they can relate to.
Attention and Awareness
Attention and awareness is the second part of the tinnitus cycle (Figure 1). Figure 3 illustrates the subcortical awareness pathway of sound processing. This is a simplified way to view how our brain filters and categorizes all the sounds that we hear on a day-to-day basis. There are some sounds that make it straight up to our awareness centers. Then there are some sounds that require an action on our part or sounds we have to do something about, and then there are other sounds that never make it to our focus of attention. They get filtered out to other subconscious brain centers.
In the severe tinnitus patient, the brain has an incorrect label on their perception of tinnitus. Their brain is categorizing the tinnitus signal as something harmful, something threatening, which is incorrect. But in that labeling, the brain filters that tinnitus perception to their primary focus of attention. It is important that with treatment, we teach the brain to change that categorization of the tinnitus perception. How do we do that? Well, we have to eliminate the stress response, which we will address in a moment.
Figure 3. Schematic of sub-cortical awareness processing.
Dr. Jastreboff, the founder of Tinnitus Retraining Therapy (TRT), gives one example of a tiger. Let's say prior to this talk I visited your office, and I brought in a tiger and set him over in the corner of the room. I said, "Do not worry about this tiger. He has not eaten anyone in at least a couple weeks, so he should be fine. Just try to focus on this compelling wonderful talk that you are listening to on AudiologyOnline." Well, no matter how dynamic I am as a speaker, I would say that you are going to be largely focused on that tiger over in the corner. That is exactly what is happening with these tinnitus patients. They are trying so hard to push aside their tinnitus perception and focus on their day-to-day lives, and they are not doing very well. Rightly so, because that tiger is pretty threatening, and so is their tinnitus. That example helps them to understand what they are going through.
I think another great example is the fridge, especially if they are wearing hearing aids. Prior to wearing the hearing aids, a patient may have not heard the refrigerator noise, and then as soon as he or she was aided, heard the refrigerator, the computer fan, the squeak on the front door, the blinker in the car and all these "new" sounds. Their brain had to relearn what sounds are important and what sounds need to be filtered out to those other brain centers. Patients with hearing aids can absolutely identify with that.
Another important example is the train. This example can serve to give your patients hope in this whole process. Let's say that you purchase a new home not too far from a railroad track. A train comes through every few hours. For the first few weeks, you wake up three or four times a night, whenever that train comes through, because your brain is on alert. "Here's the train whistle. We haven't heard this before. We need to react. We need to do something." But what happens in week three or four? Maybe you only wake up once or twice. Before you know it, your brain has habituated to the train whistle. You no longer wake up. That is exactly what we need to help these patients do. This example can give them a lot of hope because it illustrates how that filtering process in the brain can change. Changing how the brain categorizes the tinnitus signal is what we are after.
Because a patient's brain incorrectly labels the tinnitus as important or threatening, it can be truly a phobic response. I always reassure patients this is not a conscious decision, because many of them say, "Why can I not just reason this away? Why can't I learn to not pay attention to it?" They have tried everything under the sun, and they do not understand why they cannot get in front of this. The reason is that you have to address it from a global perspective. You cannot just touch on the awareness or feed the auditory system or give the patient ability to relax. You have to look at it from all angles in order to treat the tinnitus effectively.
What I find interesting is that sometimes the patient can pinpoint a past traumatic event that started their tinnitus. That definitely is evidence of this incorrect labeling and the subsequent emotional response. I do find, though, that it is not always productive to spend a lot of time on what that event was. I definitely think acknowledging the event is important, but the bottom line is that we cannot change that event. It has happened. What we have to do is work on a plan to address it and move forward. I find that too many patients get hung up on what happened, and reality is we cannot change it. We have to do is work to change what we have in front of us. That is where you come in developing a treatment plan for them.
My favorite example - and I do not think you can have enough examples, because every patient is different - is to imagine you are lying in bed at night and you hear a scratching at the window. My husband would hear that scratching at the window and say, "You know what? I forgot to trim that bush. I guess I will get to it tomorrow. I am not going to worry about it tonight," then roll over, go back to sleep. I, on the other hand, hear the scratching at the window, and I definitely do not feel that way. I am up. "We are going to see what it is. Who is trying to come in? What are we going to do about it? Do we need to call the police?" That sound definitely gives me an auto action. It is interesting for patients to understand the difference in how we react to the same sound and how that relates to their tinnitus. That is what makes patients, especially these severe patients, different from that person who just hears their tinnitus occasionally. The brain of those who do not "suffer" from tinnitus does not sense the tinnitus as a threat and it moves on. However, the other person who hears that tinnitus sound definitely has a different reaction.
Emotional Response
I think the emotional response is one of the most important areas of the cycle (Figure 1) to focus on. Again, we have a brain that is starving for input generating this tinnitus signal. The brain has incorrectly labeled the sound as important, causing the focus of attention to be front and center. Unfortunately, due to this, there is activation of the autonomic nervous system as well as our limbic system. The autonomic nervous system is where the fight-or-flight response is housed, and this definitely can elicit that response in patients. The limbic system is where our emotions are housed, and that is where a lot of these negative feelings can come from. Those areas are very closely related to the centers in the brain that are generating the tinnitus.
Patients may not even realize it, but this response is often physiological. Their heart rate quickens, respiration quickens or they may start to perspire. This helps to illustrate the point that their reaction to tinnitus is not a conscious decision. They do not decide to feel this way about their tinnitus and get worked up about it. It is their body's and their brain's reaction to the sound.
A great question for these patients as part of your tinnitus assessment is, "What goes through your head when you hear the tinnitus? What feelings do you have?" We will get into some open-ended questions in just a minute, but responses to these opening questions can help you to understand what the patient is experiencing. Often, you hear words like hopelessness. "Nothing I do makes this any better. I am going to have to live with this for the rest of my life." Oftentimes that is what they have been told over and over again. Needless to say, they are very grateful to be in your office and to get some answers.
There is a sense of loss of control. Nothing they do makes this any better. They do not have control over it, and that can be a pretty helpless feeling, especially when the tinnitus personality tends to be in control of things. Having the tinnitus control their life impacts them even more negatively than someone else. Definitely do not discount that control piece.
Guilt is another big emotion. "What did I do to bring this on? What did I do to deserve this?" The guilt starts to manifest as, "Was it that medication I took? Was it that concert I went to?" Patients will try to pinpoint what caused the tinnitus. In reality, we will never know. Typically, it is not something important to focus on unless it is something that we can change. But guilt is a big issue, and people can devote a lot of time and energy to overanalyzing what will make it worse or better. A person can become consumed by that. I have seen that quite a bit, and it is definitely not productive in the treatment of tinnitus.
Fear and anxiety are two other very large components related to the emotional response of the tinnitus cycle. I know you see it time and time again in a patient who is wound up, on the edge of their seat, and will not let you get a word in edgewise. It can be hard to rein them in and get at the heart of the matter. But as you see these patients, you get better and better as time goes.
Treatment Considerations
Now you should have a good understanding of how to relate the tinnitus cycle to your patients and what specific experiences they may be having. The most important thing when you are considering any treatment is making a determination of the patient's quality of life. Where does the tinnitus bother them the most? Where is the tinnitus most disturbing? It is so important to hone in on those specific areas so that you can make changes in how they are able to manage and cope with their tinnitus. I cannot reiterate that enough. You need to understand specific areas of how their tinnitus is impacting them day-to-day so that you can help them to make changes and get better.
There are questionnaires that offer good questions for our patients, like the Tinnitus Reaction Questionnaire (TRQ). That is the questionnaire that Neuromonics uses. The Tinnitus Handicap Inventory (THI) is another one. However, these are not the best tools for every patient, and I think it is good to have a well-rounded approach to your interview so that you can get the most information from your patient as possible. The bottom line is that the TRQ and the THI just have you circle score numbers. In these cases, you have to make sure that the patient in front of you matches up with that score. I think these open-ended questions are a great way to do that.
The first question you might ask the patient is, "If you did not have your tinnitus, how would life be different?" Notice I do not qualify whether life would be better or worse. From that question, you will get things like, "I would be able to sleep at night. I do not think I would yell at my wife as much because I wouldn't be as on-edge." Responses like that can help you to understand what the patient is experiencing, and sometimes what the family is going through, which definitely compounds the tinnitus impact overall. That question helps me to get at the heart of the matter.
Next, "What are your goals for treatment?" This question allows you to do quite a few things. One, I find patients will often confuse their communication needs or hearing loss with their tinnitus. I have even seen where they filled out the whole TRQ, even though it says Tinnitus Reaction Questionnaire, in relation to their hearing. You may have a patient say, "Well, if I did not have my tinnitus, I would be able to hear better." This is a blatant red flag. Right there you know they are having some hearing issues. And actually the inverse of that is true. If they could hear better, in some cases, their tinnitus would not be as bothersome. That is definitely an opportunity for education as well as expectation management.
You will have patients who will also say, "I do not want to hear my tinnitus ever again." Well, that is not entirely realistic. If you will go back to the Heller and Bergman (1953) study, remind them that even normal-hearing college students could hear their tinnitus if it was quiet enough and they listened hard enough. Anyone can do that. It is important for them to understand that aspect. You may have to provide some education and revise expectations with whatever treatment that you choose. This question helps you to get a handle on what they are looking for and make this more of a black-and-white endeavor. Tinnitus treatment can become a huge, gray nebulous entity. You do not know where one thing begins and another thing ends, from hearing loss to hyperacusis. Setting these questions and expectations up at the beginning will help you be way ahead of the game as you progress through treatment.
Hyperacusis
Throughout the literature, the prevalence estimates of tinnitus are all over the board. I can tell you, anecdotally, that I see it a lot. What often happens is it that it comes in under the radar due to patients constructing their own sense of "normal." What I mean by that is that is the patient has altered their environment in such a way that they are not as affected by their sound sensitivity. At home, maybe they cannot be in the house when the dishwasher is unloaded, or the grandkids are not able to come over. They may not go out to a restaurant at all, or if they do, they go at 3 in the afternoon when there is nobody in the restaurant. They have altered their lifestyle based on their sensitivity to sound, and sometimes they have done it for so long they do not even realize that life does not have to be this way. It is important not to overlook this, yet I see it happen regularly. Rightly so, because the patient may not even bring it up.
I find that hyperacusis can be just as disturbing, sometimes even more so, than the tinnitus. It can be truly debilitating and limiting, but these patients are not doing anything as a result of their sensitivity to sound. In terms of quality of life, this is a big area that we can impact with treatment. On a side note, this is one of the things that Neuromonics does well. It is my favorite aspect of treatment. It happens quickly. Patients feel better and they get back to their lives. So, it can be a rewarding aspect of practice as well.
My open-ended question for hyperacusis, and one I ask every tinnitus patient whether they report an issue with sound sensitivity or not, is, "Is there anywhere that you do not go or activities that you avoid due to your sensitivity to sound?" Things start to come out. I cannot tell you how many times I have heard that dishwasher analogy; it is certainly a red flag. Sirens start to go off in my head and I know I need to follow up and see what is going on.
A follow-up question may be, "Are there any sounds in your everyday environment that are uncomfortably loud to you?" A frequent answer I get to this question is the microwave beeping. It helps you get a sense of the impact of sensitivity to sound and if it warrants treatment. A critical piece of treatment when tinnitus is concurrent with hyperacusis is that you have to target the hyperacusis first with treatment, before the tinnitus can be effectively addressed.
Let's think about that just a minute. Say you have a patient that needs "x" amount of sound to get any relief from their tinnitus. If his or her tinnitus is not covered until you apply greater amounts of sound, you are not going to get anywhere with the tinnitus relief until the sensitivity to sound is improved. In essence, you keep hitting the ceiling before you can effectively address the tinnitus, and you run into this Catch 22 situation. You are caught chasing your tail, so to speak, with these patients. I cannot emphasize enough to make sure that the hyperacusis is targeted prior to working on your tinnitus goals. Sometimes these issues can be handled simultaneously, but never the tinnitus before the hyperacusis due to this reason. I do see this all the time, and it is often due to the patient not reporting issue with sound sensitivity. Luckily, with Neuromonics, you have data logging. You can see the volume at which they are wearing the device, and it helps you to troubleshoot this issue and achieve treatment goals.
Another situation with which I am presented quite often is, "I have this patient who has only had tinnitus three months. Would you wait on treatment or move ahead? Would he be a good candidate?" And my question in return is, "What issues is he having? What is the full story?" If life has stopped, he has had to quit his job, he is not functioning or having major quality-of-life issues, then absolutely he is a candidate to move forward with treatment after you receive the proper medical clearance. If a patient's life is on hold, why would you not help them to get on top of the tinnitus get their life back?
By the same token, you can have a patient who had had their tinnitus for 30 years but has developed great coping strategies and management skills. I am always very careful to give patients credit for that, because it is not always easy. But at this point, they may hear their tinnitus occasionally, or it is there but it is no big deal. They are able to move on and do what they need to do. This patient is probably not a good candidate for treatment. He or she is doing okay. The duration of tinnitus as a determination of treatment may take a backseat to the emotional significance and the impact on the patient's life. Always consider that the impact on life should dictate your clinical decisions.
Let's spend a brief moment on what Neuromonics is and how it works. Neuromonics' treatment is about customized acoustic stimuli. We use music as the carrier for the treatment, and we spectrally modify the music based on the patient's audiogram, including extended high frequencies. The Oasis device (Figure 4) is an engineered treatment device, built to achieve these treatment objectives for patients with tinnitus. It allows you to do some unique things in order to achieve the outcomes that you are after.
Figure 4. Neuromonics Oasis device.
As important is the interactive counseling provided from a trained Neuromonics clinician. This is something that we do provide training on. We also have a new counseling handbook that will be coming out shortly that has a wealth of knowledge and different counseling concepts for specific patient issues to help to guide you in seeing these patients in the office.
Figure 5 is a screen shot of the Neuromonics data logging screen. It is extremely colorful, but it gives you a lot of great information when seeing your Neuromonics patient, because it makes them accountable for the recommendation that you give them. Are they following through or not? It also helps you with expectation management and making sure that the patient achieves the objectives that you set at the outset of treatment.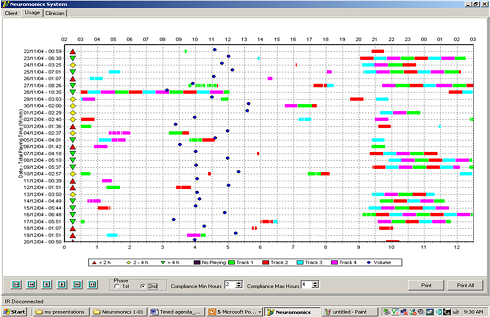
Figure 5. Neuromonics data logging screen. Click here to view larger version (PDF).
Recall the tinnitus cycle (Figure 1). How does Neuromonics address each of those aspects? First, there is stimulation to the auditory system. Again, the music is the carrier for the treatment, and we are providing a wide-frequency acoustic stimulus all the way out to 12,500 Hz. It is customized based on each patient's hearing profile, like a prescription for the individual's hearing. So we are giving that patient the stimulation that he needs in those areas. What we find is that it eliminates that compensatory mechanism that the brain activates due to that lack of input.
As a result, the tinnitus becomes softer, and we see objective evidence of that in the booth. There is a measure that is completed during the tinnitus evaluation called the Minimum Masking Level. That is the amount of noise needed to cover a patient's tinnitus. If Neuromonics is doing what it is designed to do, that masking level number will get lower as they progress through treatment.
I think it makes sense to touch on the emotional piece next. The music treatment with Neuromonics' treatment is designed to be pleasant and relaxing, and help the patient get a sense of control and relief from the tinnitus. That is huge. We have patients who have a sense of hopelessness, loss of control and anxiety. If you give them the ability to get relief when they want it, we have attained success. Eliminating the stress response and teaching the brain to lose that incorrect labeling of the tinnitus is the most desirable outcome. That is what we are achieving with the relaxing aspects of the music.
Next is habituation and desensitizing the system so that the tinnitus is no longer the focus of attention. If the emotional response can be removed, habituation will follow. That is the goal of the attention piece, and we use the music in order to achieve that.
In our third clinical trial, we conducted a survey looking specifically at patients who had reported a moderate or large benefit from the Neuromonics Oasis device (Davis, Paki, & Hanley, 2007). Of those patients, 97 percent were able to achieve relief from their tinnitus; 94 percent experienced an improved ability to fall asleep; 94 percent perceived a sense of control over their tinnitus; and 94 percent noted an improved ability to relax. The music is a pretty powerful aspect of this, and I think it is why we are able to achieve effective outcomes.
Advantages
One of the main advantages of Neuromonics' treatment is rapid relief and a sense of control. We all know those tinnitus patients that come in the office talking so fast, on the edge of their chair, anxious about life in general. You can see they are about to come out of their skin. What I love to do is demonstrate the device. Each Neuromonics clinic will get a demo unit. When you put the device on the patient, you get to see that relief happen. Many patients will sit back in their chair, close their eyes and stop talking. You can tell they are getting relief. Sometimes you have to pry it out of their hands before they leave the office because you have to get the treatment customized for their hearing profile.
The next advantage is improved relaxation and ability to sleep. This is extremely important. I do not know about you, but if I am not sleeping, I am not worth anything. Sleep is huge. To give a person the ability to get more sleep is definitely going to help improve their quality of life. The things we are after with Neuromonics are reduced awareness, reduced disturbance of tinnitus, and eliminating the emotional stress response, which then changes the way the brain categorizes the tinnitus so that patients are no longer filtering it to their focus of attention.
The Neuromonics Oasis device provides improved tolerance to loud sounds. I cannot emphasize the importance of this enough. That is something that we do well. We have a protocol for it, and I love to see clinicians take advantage of that. We have also shown a long-term benefit. This is a six-to-eight-month treatment, sometimes longer if there are concurrent issues with hyperacusis or psychological issues that need to be addressed. But after patients finish treatment, it is not something they will have to continue using every day. They then go to more of a maintenance phase. We definitely know stress is a trigger for tinnitus and it can creep back up again, but patients can use the device as a tool from that point. It is not anything that they have to use every day for the rest of their life.
Case #1
The first patient has a TRQ score of 11. In terms of Neuromonics candidacy, a score of at least 17 is determined to be significant. Below that, there is usually not a lot of impact on day-to-day activities from the tinnitus. This patient's loudness discomfort levels are between 65 and 75 dB. To provide some quick definitions here, hyperacusis is 70 dB and below, and decreased sound tolerance is 90 dB and below.
Their tinnitus awareness is 80 percent, meaning that they hear their tinnitus 80 percent of the time. They report disturbance as 5 percent. They have a mild high-frequency loss. This patient is a professional piano tuner, and he is changing careers because his tinnitus is exacerbated by his work. It is bad enough to make him change professions. He is also going back to school. He ranked the order of difficulty as tinnitus being first, sound sensitivity second, and hearing loss third.
First off, what sticks out in your mind? What are the red flags that you see? This sounds like a patient who does not recognize hyperacusis or sound sensitivity. I would bet that that is creeping up into other areas of his life and is something we definitely need to discuss in more detail.
A few other issues are that he is reporting only 5 percent listening disturbance, yet he is changing professions as a result. I do not know that the 5 percent is accurate. The TRQ is not always an accurate portrayal of the patient in front of you. So with a low TRQ score of 11, I would go back and look at his specific responses where he provided a 3 or 4. While the score may be low, you still need to consider that patient's quality-of-life impact.
Case #2
The next patient has a TRQ score of 88, loudness discomfort level around 80 dB, tinnitus awareness and disturbance of 100 percent. He scored a 2 on the suicidal ideation question on the TRQ. He is currently undergoing treatment for post-traumatic stress disorder, and likely anxiety and depression as well. He is having issues with sleep, and he is already using hearing aids for hearing loss. He is retired, and that is not always a good situation for a tinnitus patient because it often only gives them more time and energy devote to thinking about the tinnitus.
The main thing that jumps out at me here is the TRQ score. It is extremely high. The highest TRQ score is 104. He also reports extremely high awareness and disturbance. In these cases, sometimes you have to recommend volunteer activities, hobbies, and other things that will take away the time they spend thinking about their tinnitus. You definitely need to be prepared for psychological issues here. From a practical standpoint, it is a good idea to have a relationship with a behavioral health professional. You want to be comfortable with someone so you can make referrals with confidence.
This patient is a common scenario in the Veteran's Administration (VA) system. Although he has post-traumatic stress disorder, this patient is still a potential candidate. As long as he is aided with his hearing aids, he can still be a candidate for the device. This is a patient where you would definitely want to take advantage of the demo device in the office. You would also want to coordinate with his behavioral health professional so support can be provided consistently.
As a note of information, we can treat a patient with a dead ear as long as the better ear has a pure-tone average of 50 dB or better. If you have those patients and you are a Neuromonics clinician, definitely reach out to one of the clinical specialists. We are happy to help you with treatment considerations and the best way to go about treating that patient.
I hope that you feel more comfortable in talking to your patients about tinnitus, relating to them and displaying empathy, because it is so important. This is a huge issue for a lot of patients, and they need to know that you understand and are there to help them. I think a global approach is best. You cannot just look at the tinnitus. You have to look at their audiogram. You have to look at hyperacusis, which sometimes has to be pulled out a little bit to recognize that it is an issue. Patients often have psychological needs, which is a big part of this, as you well know. Being able to address those needs is a very important part of beginning a successful treatment program.
Lastly, I feel like patient education in addition to a treatment plan is imperative. This allows patients to know where they are going, like they have a game plan. It yields hope for your patients. That is what they need because this can be such a hopeless condition, and they have not been given a lot of hope by other health professionals. I think it is our job to do that now with all the information and treatment tools that are available to us. I definitely feel that it is an extremely important and rewarding aspect of clinical practice, and I hope you feel the same. If there is anything that we can do for you as a company, please feel free to reach out to us. Thank you for attending today.
References
Davis, P., Paki, B., & Hanley, P. (2007). Neuromonics tinnitus treatment: third clinical trial. Ear and Hearing, 28(2), 242-257.
Heller, M.F., & Bergman, M. (1953). Tinnitus aurium in normally hearing persons. Annals of Otology, Rhinology and Largyngology, 62, 73-83.
Shim, H.J., Kim, S.K., Park, C.H., Lee, S.H., Yoon, S.W., Ki, A.R., Chung, D.H., Yeo, S.G. (2009). Hearing abilities at ultra-high frequency in patients with tinnitus. Clinical and Experimental Otorhinolaryngology, 2(4), 169-174.

