
Interview with Jane Madell, Ph.D., Director, Hearing and Learning Center and Co-Director, Cochlear Implant Center, at the Ear Institute at The New York Eye and Ear Infirmary, NYC
 Carolyn Smaka: Today I'm visiting the Ear Institute at the New York Eye and Ear Infirmary and speaking with Dr. Jane Madell. Jane, thanks for having me today, your new center is amazing!
Carolyn Smaka: Today I'm visiting the Ear Institute at the New York Eye and Ear Infirmary and speaking with Dr. Jane Madell. Jane, thanks for having me today, your new center is amazing!Jane Madell: Thank you, it's my pleasure.
Smaka: Can you begin by giving an overview of the center?
Madell: Sure - When we developed the Center, our goal was to build a home for families affected by hearing loss. Most of the time when a child is diagnosed with hearing loss the family has to go to a number of different places to receive services - an otologist, an audiologist, a hearing aid dispenser, an auditory therapist etc. We are a full service agency where we provide all services in one location except school. We offer otology, ophthalmology and genetics here, and we can refer for all other medical services that a family may need since we are part of a major medical center. We have 14 audiologists who provide a full range of services including diagnostic audiology and rehabilitative audiology. We fit hearing aids and FM systems. We conduct auditory processing and other learning evaluations.
We have a cochlear implant center that does everything - from the initial intake to determine candidacy, to evaluating or changing a person's current hearing aids if needed, to performing cochlear implant evaluations and cochlear implant mapping. We also monitor performance with cochlear implants using speech perception so that we know what to change in the mapping process to improve performance.

We have speech language auditory therapists, who work with both children and adults to help them learn to maximize their auditory skills, from the time we identify them as newborns through adults who are getting cochlear implants. We have education services - we have three teachers of the deaf who provide services in the schools to assist classroom teachers in maximizing the mainstreaming performance of children with hearing loss.
We also have two educational audiologists who go into schools. They ensure that the FM systems are working, and that the teachers know how to use them and how to do troubleshooting if there are issues.
We have a social worker who works with families affected by hearing loss to help through all the crises, which you can't help but have, when you have a child with a hearing loss. Because we are part of an Eye and Ear hospital, The New York Eye and Ear Infirmary, we are also able to do very early evaluations for retinitis pigmentosa, and provide full vision services in order to plan for a child's future.
Then, we have the vestibular rehabilitation program. Some of our very little ones may have some balance issues that can be addressed through our vestibular program.
We have an auditory oral, auditory-verbal philosophy. Our philosophy is that we want children to talk and to learn language through listening. We do have people that sign, but the people who come for therapy here are people with the goal of maximizing auditory-aural performance.

Smaka: And you see the full age range, from birth through seniors?
Madell: Yes, we have the full range from birth, to a few people who are over 90.
Smaka: This is a beautiful new space and it looks like a very exciting place to work. How large is the staff?
Madell: We have about 40 staff here now. We have 14 audiologists, 3 auditory therapists, 2 teachers of the deaf, 2 educational audiologists, two social workers, 6 full-time otologists and a number of other part time physicians as well as clerical staff. It is a wonderful place. Everyone who is here has been working in the field for a while and is very passionate about what they do.
Smaka: Thanks for that overview. Next I wanted to talk with you about fitting amplification to babies.
Madell: Great, one of my favorite topics. We all know that the research very clearly demonstrates that you can't fit amplification early enough. We know from research done at the University of Colorado, for example, that if we don't have kids hearing by six months of age, they never really catch up. No matter how good a job we do afterwards, they don't catch up.
There is no question we have to fit children with amplification early and ensure they are hearing as close to normal levels as possible so that they can make use of incidental learning (overhearing conversations) the way their typically hearing peers do. I know that many people are really uncomfortable doing behavioral testing on babies. If a child can raise his hand or turn to the VRA reinforcer, everybody is perfectly comfortable with proceeding with amplification. But many audiologists don't feel comfortable evaluating hearing in very young infants and fitting them with hearing aids.
I have developed a behavioral evaluation technique for obtaining behavioral thresholds by looking at changes in sucking. Carol Flexer and I just published a pediatric audiology textbook that comes with a DVD on demonstrating this technique. (Madell & Flexer, Pediatric Audiology: Diagnosis, Technology and Management, Thieme 2008). We still begin testing babies using ABR. But ABR is not a measure of hearing. By using ABR along with behavioral responses we get a very good picture of what a baby is really hearing.
Once you put hearing aids on a baby, how do you know the hearing aids are doing what they are supposed to be doing? How do you know the child can hear with the hearing aids? Unless you can measure that behaviorally, you don't know.
Smaka: You are talking about behaviorally measuring hearing. Because you can verify the fitting using probe microphone measures and the RECD.
Madell: Right, but you don't know what is happening in the child's brain unless you have a behavioral measure. You can measure how much sound is going into the ear but we need to know what exactly the child is hearing. We can't wait until the child is 6 or 8 months old and then do VRA to find out whether or not the child is hearing sound at a soft enough level. So, we absolutely must have a method of finding that out before the child is old enough for VRA.
Behavioral observation has gotten a very bad reputation because people have looked at respiration changes and limb movement, which are not threshold responses;they are responses to loud sounds. So, these measurements have not been in agreement with threshold measures. I have demonstrated that by looking at changes in sucking as a response, you can obtain accurate threshold measures of how a child is hearing.
Smaka: As you mentioned, your textbook covers this in detail. We should also mention that you'll be presenting an upcoming course on AudiologyOnline in February on this topic. But, just briefly, can you describe this method?
Madell: We ask the parent to bring the child in hungry, and then the child can suck on whatever they typically use during the evaluation. If the mother is nursing, we ask the mother to nurse. If they use a bottle, we use a bottle. If prefer a pacifier, then they can use a pacifier during testing.

We bring them into the test room hungry. We then let them nurse for a few seconds just to get that initial starvation down. Then, we present a stimulus and have a video camera focus directly on the baby's mouth, which shows on a monitor on the audiologist's side of the test booth so the audiologist can easily see changes in sucking. Then we present sound (just as you would with any other hearing test) and we look for changes in sucking. If the baby has limb movements or eye movements, that is fine, but we are not considering them a response to the stimulus. We are only counting changes in sucking. The change in sucking has to be tied to the stimulus the same way that a wave V has to be tied to the stimulus with an ABR, or a head turn has to be tied to the stimulus when you do a VRA. What we find is that some children respond when the stimulus starts and some respond when the stimulus ends. Most kids respond very consistently.
Smaka: And they stop sucking?
Madell: They can either start sucking or stop sucking. I'll show you audiograms where I have used this method, and then followed children over time. And you can see that they are very consistent.
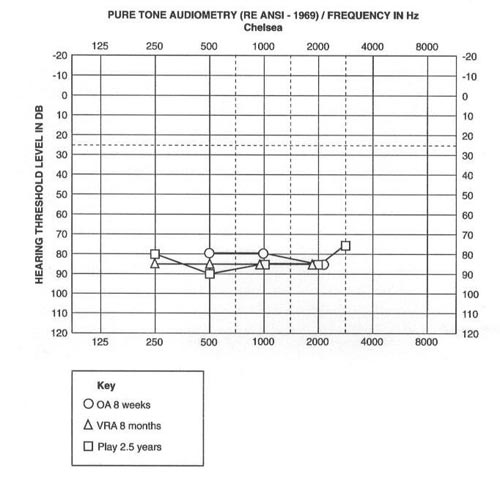
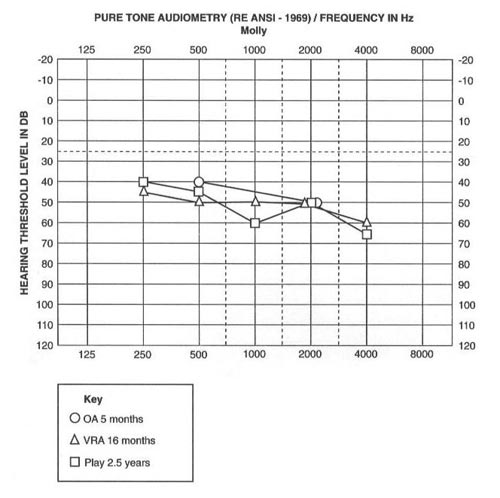
Madell: Here you can see the audiograms. The 0's represent the thresholds as measured through this behavioral observation method, the triangles are the thresholds that were measured with VRA when the children were older, and the squares are the thresholds measured with play audiometry.
Smaka: Wow, the thresholds with all three methods basically overlay each other.
Madell: Right. So we know it works. And it gives us the verification that we need to confirm what the baby is hearing with the amplification.
Now, you can do an ABR. You can fit a hearing aid with real ear measurements. And you can know that the baby's getting something from that hearing aid, but you have no way of knowing what the baby is hearing, or if he is hearing at normal conversational levels throughout the frequency range, including in the high frequencies, unless you have the behavioral measures to confirm it. We can't perform an ABR every three weeks to confirm what a child is hearing with the hearing aids. You just can't do it. So, we have to have a behavioral technique that accurately measures a child's performance.
Smaka: How do you get referrals on babies that are so young here, are you doing newborn hearing screening?
Madell: We get referrals from all over New York City for the babies that have failed newborn hearing screenings, because we have a very good follow up program here.
Smaka: Follow-up is an important component of newborn hearing screening. How do you achieve good follow-up?
Madell: I think hospitals have to take real responsibility for making sure that these failed babies don't get lost. The hospital has to make sure that all of their pediatricians understand the importance of follow-up to a newborn hearing screening and don't tell parents there is no need to follow-up.
When we started newborn hearings screenings at Beth Israel Medical Center, first we had to make sure that we reduced the number of false positives so that we sent very few kids for follow-up. If a baby failed the first screen, we re-tested them twice before they left the hospital. So, we didn't have the problem of an enormous number of children being referred. We also had to deal with the issue of failed babies where the pediatricians would tell the parents, "Don't worry about it, the child will be fine." They don't say that anymore because we then worked very hard to educate the pediatricians.
Smaka: Can you talk about the work you've done regarding amplification and speech perception?
Madell: Certainly. Everybody knows that the goal of fitting hearing technology is for people to be able to understand speech to be able to communicate. And we make the assumption that if we fit technology, then people will be able to understand speech. But that assumption may not be correct, and we won't know unless we go in and test and measure that.
It would not occur to any audiologist to do a diagnostic hearing evaluation and not conduct speech perception testing under earphones. But, how often is speech perception tested with the technology? Why is it more important to know how a person hears with earphones than it is to know how they hear with their technology?
What we need to know is how they hear with technology. So, what we do here at our center is assess both children and adults with their technology, whether it's hearing aids or cochlear implants. Our protocol is to test at normal conversational level (50 dBHL), at soft conversational levels (35 dBHL) and in competing noise (50 dBHL +5 SNR, because that's how they'll use their technology in the real world.
Classrooms noise levels are 0 SNR or +5 SNR. So we do not want to test at +10. We want to test a +5 because that is realistic noise. Then we can figure out what has to be done.
And if the person is wearing two hearing aids, then we've got to test that person with the right hearing aid alone, with the left hearing aid alone, and with the two hearing aids together.
You would be amazed how often we find that the speech perception with one hearing aid is much poorer than with the other hearing aid. That tells us something. Is that hearing aid doing something it shouldn't be doing? Is it distorted? Or, does that person need some therapy with the poor ear alone to build up the poorer ear skills? If you have two ears working together, you're binaural score should be better than one ear alone. And, if you don't test each ear separately, you will never find that out.
Smaka: And one ear could be doing the work the whole time. Or the hearing aid could be malfunctioning on one side.
Madell: Exactly. Unless you test each ear separately you don't have that information. So, we want to test both ears separately at normal conversational levels. We also want to test soft conversation, because we don't live in a quiet world, only talking with people who are within three feet of us. We want to know if the person wearing amplification is going to be able to hear people who are speaking to him or her from six, seven or eight feet away. It's important to know that. If they are not hearing soft speech at 35 dB, then something is wrong. We also want to know how they hear in noise. Classrooms are very noisy settings. Work situations are noisy. The dinner table is noisy. What are we, as clinicians, going to do to change that situation?
Does the person need an FM system just for the classroom? Is the person working and in meetings all day along? Is an FM system for meetings needed? Or, do they need an FM system for the dinner table so they're not stressed out when they're sitting with their family? If we don't test speech perception with their technology in lots of different situations, we are never going to find it out.
Smaka: What kinds of noise do you use for testing in noise?
Madell: That's an important question. We use four-talker babble. Speech noise from the audiometer is not appropriate;it's very easy to ignore and it doesn't really interfere with understanding. But, four-talker babble really interferes and is a good example of what it's like to hear in a noisy world.
Smaka: You probably could write a full textbook on my next question. How can you tell if a person is performing poorly because of their damaged auditory system, and when, if ever, do you tell them "this is the best you're going to do, and you're going to have to live with this".
Madell: The first answer is never, "You have to live with it." The first answer is, "Let me see what I can do." As an audiologist, you need to consider if this is someone who needs hearing aids with high end digital capacity because they have very poor auditory skills. Should the person be moving from a hearing aid to a cochlear implant? Do they need auditory therapy? Do we need to get that person some listening therapy and try to build up the skills that way?
Once you have done those things, then you know there's nothing more you can do. Then you can say, 'This is the best your ears can do." But, until you have really tried everything, you don't have any way of knowing that it's the best the person can do. We have so many people who come to this center for a second opinion. Their biggest complaint is that the people they were working with just said, "Learn to live with it," and didn't try everything else that could have been done first.
Smaka: You presented a course on AudiologyOnline entitled "When to change amplification technology in children" that touched on some of these issues (www.audiologyonline.com/ceus/).
I also wanted to ask you about your latest research with cochlear implants.
Madell: Sure. Everybody knows that cochlear implants are good for people with profound hearing loss. Nobody questions that. But, there are a lot of patients with severe hearing loss who are not doing well with their hearing aids, and we need to consider these situations carefully. If a person with a severe hearing loss is doing well with hearing aids, if they are hearing close to the normal range, if they have good high frequency speech perception and if they have good word recognition in most situations, then that person isn't a cochlear implant candidate.
But, there a lot of people with severe hearing losses who are doing really poorly with hearing aids. And as audiologists, we have to first try everything we know in order to help them become better performers. Do they need higher end digital hearing aids, which will provide much better quality for them? Do they need some auditory therapy to see if we can build up their skills? And if we have done those things and if they are still struggling, I think we need to think about cochlear implants.
Last year, we conducted a multi center study of patients with cochlear implants with the Children's Hospital of St. Louis and the Colorado Ear Institute. Allison Beiver at the Rocky Mountain Ear Center, Ruth Reeder at Washington University School of Medicine and Jillian Crosson at Cochlear Corporation collaborated with us. We looked at our patients who were fit with cochlear implants off label. These were children at the low end of the severe hearing loss range, but really didn't meet all of the FDA cochlear implant criteria because their hearing was a little bit better in some areas.
These kids were doing better than the criteria for normal conversation, but were struggling for soft conversation, were having trouble in competing noise, or weren't getting high frequencies with their technology. They missed the 's,' 'sh,' and thus the important grammatical markers for pluralization and possession etc. For a child, that's going to affect language, reading, and every aspect of academics. We looked at twenty-one children from age 3 to 17 who were implanted, and we reported on the pre- and post-implant data. The difference pre- and post-implant was absolutely breathtaking. Before their implants, these children were coming home exhausted. Kids who were previously getting 60% speech perception scores before their implant were all of a sudden in the 90th percentile on their speech perception scores after the implant. The differences were dramatic in their pre- and post-implant scores. And the difference it made in their lives was amazing. We're in the process of preparing the data for publication.

Smaka: What is your experience with steeply sloping hearing losses where there is no hearing in the high frequencies? Those were the patients I found most challenging when I was working clinically.
Madell: There are a lot of exciting new developments in this area. There are two cochlear implant devices in clinical trials now for these types of hearing losses. We have been involved in the trials and have found that people's ability to hear in the high frequencies is much, much better when they get implanted. They use short electrodes which only affect the high frequencies. What some people are doing is using a hearing aid for low frequency information with a cochlear implant for high frequencies.
Smaka: What is your experience with nonlinear frequency compression technology?
Madell: We've had very good experience with the Phonak Naida. We fit a few older children and teenagers. One who comes to mind was actually rejected for the cochlear implant study I mentioned earlier, because they thought her speech perception was too good. She was a college freshman, and although she was really struggling, she didn't meet the criteria for the research project. We fit her with the Naida, and she said it was like, "Waking up from the dead". Those were her words. She said she heard things that she just couldn't believe she was hearing.
Smaka: Jane, before we conclude the interview I wanted to mention the conference that you'll be having in February.
Madell: It is called Controversial Issues in Pediatric Audiology and will be held on February 26th and 27th, 2009. The conference is given by the Hearing and Learning Center and Cochlear Implant Center at New York Eye and Ear Infirmary, along with the Children's Hearing Institute (www.childrenshearing.org), which is our educational outreach and fundraising arm. It is the Children's Hearing Institute's 25th anniversary, so this is going to be a big bash for us.
The first day of the conference, February 26th, is Auditory Verbal Day, and John Niparko from the Cochlear Implant Center at Johns Hopkins is speaking about quality of life issues related to hearing loss and cochlear implants. Diane Brackett, from NECCHI in Connecticut is presenting about mainstreaming issues. Perri Hecht will be presenting about bi lingual issues for managing children with hearing loss.
On Friday, February 27th, which is Audiology day, we have Yvonne Sininger presenting on auditory neuropathy, Carol Flexer speaking about literacy and hearing loss, and Anne Marie Tharpe presenting on managing mild and unilateral hearing loss. And I am going to talk about selecting technology and how to know when to select which kind of technology for children with hearing loss.
Smaka: For more information or to register, audiologists can go to www.childrenshearing.org. Jane, thank you so much for your time today. I'll be back in February for the conference!
Madell: Thank you, Carolyn.
References
Madell, J., Flexer, C.A. (2008). Pediatric audiology: Diagnosis, technology, and management. NY: Thieme.


Jane Madell, PhD, CCC-A/SLP, ABA, LSLS Cert AVT
Director of Pediatric Audiology Consulting
Dr. Jane Madell is Director of Pediatric Audiology Consulting. She has been a pediatric audiologist for more than 40 years. Dr Madell is a certified audiologist, speech-language pathologist, LSLS and auditory verbal therapist. Dr Madell’s clinical and research interests have been in the area of evaluation of hearing in infants and young children, management of hearing loss in children with severe and profound hearing loss, selection and management of amplification including cochlear implants and FM systems, assessment of auditory function, and evaluation and management of auditory processing disorders. Dr Madell has published 3 books, 16 book chapters, and numerous journal articles and is completing a 4th book. She is a frequent presenter at professional meetings. none