
As in an Indiana Jones adventure, we search for the lost art of tuning fork testing like that used before the advent of modern electronic audiometers, impedance audiometry, real-ear measurement systems, and electroacoustic analyzers.
Unearthed, our adventurer finds deep in the dusty bins of history a soft leather case containing six heavy-duty alloy tuning forks that resonate at the octaves of 128 Hz, 256 Hz, 512 Hz, 1024 Hz, 2048 Hz, and 4096 Hz (Figure 1). First proposed in 1550 A.D. by Italian physician Capivacci to determine the location of hearing disorders, it was not until Englishman John Shore developed a single tuning fork for tuning musical instruments at A423.5 cps that the modern tuning fork took shape. Thereafter, German physicist Chladni in 1800 developed a set of forks for testing human hearing (Feldmann, 1997).
Figure 1. Set of six heavy-duty tuning forks.
This rare artifact is accompanied with a tattered tutorial which speaks of skills and capabilities lost in the mad rush to modern technology: Weber, Rinne, Bing, and Schwabach, along with updated and unique approaches for troubleshooting and counseling hearing aid users, such as balancing binaural hearing aids, ear training for spatial skills, and contemporary skills for Transcranial CROS fittings (Chartrand, 2003). The forgotten manuscript speaks of a convenient, lightweight, and portable soundfield system that can be taken anywhere one serves the hearing impaired. It requires no electricity, set up, or maintenance. Illustrations for holding and striking the forks are shown in Figure 2.
Figure 2. Position for striking tuning forks.
In the hands of the skilled clinician, this compact system solves myriad problems that still exist even with today's digital technology. Coupled with recent scientific discoveries on the plasticity of the human brain, revival of an ancient practice promises to offer all hearing instrument specialists with a modality with which to extend their rehabilitative services.
Journey of Rediscovery
As our intrepid archeologist slogs through the manuscript in an attempt to decipher precious time-proven test methods, he pieces together the following lost tests for the mastery of contemporary enthusiasts:
The Weber Test was once an important tuning fork test that was then smugly replaced by the electric bone oscillator, only to fall out of favor in the face of bruised sinuses, poked-out eyes, and scraped foreheads. Its purpose was to detect possible unilateral conductive involvement in a hearing loss.
With these newly unearthed tuning forks, however, the test is quick and safe. We present a tone, usually 512 Hz and/or 1024 Hz, to the frontal sinuses of the forehead, while the recipient is asked to indicate in which ear they hear the tone the loudest (Figure 3). If the tone gravitates to the ear with the worst air-conduction thresholds, a unilateral conductive loss is indicated, and the exam form is marked "Weber Positive", indicating a conductive involvement in the loss. If the tone is heard in the ear with the best air-conduction thresholds or heard equally in the case of symmetrical thresholds, the form is marked "Weber Negative", meaning that there is no apparent conductive loss indicated.
As validation for video otoscopy and middle ear assessment, the Weber is a quick qualitative indication as to whether or not more investigation is needed, or perhaps, whether medical referral is indicated. 
Figure 3. Position for Weber test.
The Rinne Test, a qualitative test for sensorineural involvement, begins by informing the patient that a tuning fork will be struck and held about 2" from their ear (Figure 4). When they indicate that they no longer hear the tone, the tuning fork handle will be immediately placed over the prominence of the mastoid bone in back of their ear to see if the tone returns. If they hear the tone again, there is at least some conductive component, and the test form is marked "Rinne Negative". If the tone does not return, a sensorineural loss is indicated and the form marked "Rinne Positive".

Figure 4. Positions for the Rinne test.
An auxiliary test closely related to the Weber and Rinne tests is the Bing Test, which is a qualitative test of bilateral conductive involvement. It begins by striking the fork handle and placing it against the mastoid, then asking the patient to indicate when they no longer hear the tone. When they indicate the tone has stopped, the examiner closes the patient's tragus over the entrance to the external auditory canal (EAC) to see if the tone comes back. If it does, on either side, there is no indication of conductive component, marked "Bing Negative". Theoretically, the closure (or collapse) of the EAC should cause an increase of energy conducted to the cochlea by about 10-14 dB (Figure 5). 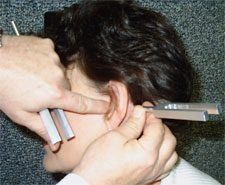
Figure 5. The Bing test begins with struck fork held against mastoid. When the tone is no longer heard, the examiner closes the canal entrance to see if tone is heard again.
Probably the most important of skills to be mastered in tuning fork testing is the Schwabach Test, which is actually a test of air-conduction thresholds that can be closely correlated onto a standard audiogram. It is given much like a pure-tone test, except that the instructions and procedure are slightly different. Since calibration is based on an ear with normal hearing, it is imperative to have one whose thresholds are normal (i.e., close to audiometric zero) standing beside the patient so that when the patient no longer hears the tone at two inches from the EAC, the fork is moved to a similar position to the calibrator ear and the number of seconds counted while the tone is still heard (Figure 6). 
Figure 6. Positions for Schwabach threshold testing, also used for unaided-aided soundfield frequency-specific testing.
Depending upon the fork's decay rate (shown in Figure 7), the number of seconds heard by the calibrator is multiplied by the rate of decay (i.e., 2.5 dB per second for the 1024 Hz fork) to determine the estimated threshold. If the calibrator ear heard the tone for 15 seconds, in our hypothetical example, the approximate air-conduction threshold would be 32.5 dBHL. 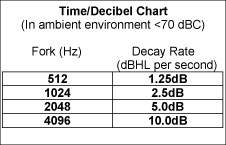
Figure 7. Relative tuning fork decay rates used for Schwabach and soundfield testing.
The test is begun by instructing the patient to listen to a struck fork at the distance of three feet from their ear, and indicate when they no longer hear the tone. Then, the fork is moved to within two inches of the EAC to see how long they hear it at that distance. When they no longer hear the tone, the fork is shifted over to the calibrator's ear, and the seconds are counted until they no longer hear the tone. The results are recorded, and the procedure is repeated for desired frequencies (generally 512 Hz, 1024 Hz, 2048 Hz, and 4096 Hz.)
If presented properly and ambient noise is sufficiently low (
Note: In case of soundfield testing, be sure to test unaided before measuring aided thresholds.
Special Tuning Fork Tests
Next, we find tuning fork tests that are important to auditory rehabilitation and hearing aid trouble-shooting. One test involves simply striking a fork at three feet to balance binaural hearing aid fittings, while others involve clicking tuning fork handles as a methodology in training of spatial functions and integration. More relevant to today's rehabilitative needs, these tests prove invaluable in the delivery of new hearing aids, regardless of how advanced the instruments are. Uses for these specialized tuning fork tests are:
- Balancing Binaural Fittings: There is no better way to balance the volume controls (VC), whether by user control or computer programming, than by using the discrete signal of a I024 Hz tuning fork tone (Chartrand, 2001; Chartrand, 2003a). First, set the VC of one side of a binaural fitting to a comfortable level with the user's voice at normal levels, not yours. Then, turn up the other side until it sounds about the same. Let the user know that you will be striking a 1024 Hz tuning fork and holding it about three feet away at zero degrees azimuth (directly in front of them). They are to note in which ear they hear the tone the loudest, then turn down the corresponding side slightly until the tone is heard the same in both ears (without any movement of their head). The reason for turning down the side that is loudest is due to the phenomena of binaural summation, attributing approximately 6 to 8 dB when the signal is heard binaurally (Chartrand, 1999). In high frequency (open ear) cases, the 2048 Hz fork may be a better choice. See Figure 8.

Figure 8. Use of the 1024 Hz or 2048 Hz tuning forks at three feet, zero degrees azimuth for balancing VCs in binaural fittings. - Ear-Training for Spatial Mapping: For many new hearing aid users, development of spatial ability is an automatic occurrence. The auditory cortex, through the central auditory apparatus, develops a unified spatial map utilizing two hemispheres of the brain. To train both depth perception and localization (only two dimensions of spatial mapping), you instruct the patient that you will be clicking the handles of two tuning forks and sweeping them from side to side at about three feet from their head. They are to close their eyes and, using only one hand, point toward the clicking. They are to stay right with the "clicks", regardless how lost they may become at first (see Figure 9).

Figure 9. Using tuning fork handle clicks, spatial mapping may be developed by sweeping from side to side until midline is transparent. A similar procedure is used also for adjusting and training for Transcranial fitting cases.
In cases where disparities exist between hearing thresholds, new users will typically have difficulty finding midline, or that point where one cortical hemisphere "lets go" of a signal and "hands it off" to the other hemisphere. In such cases they will hesitate at midline, and when the clicking has moved well toward the other ear they will "run to catch up". By sweeping steady clicks back and forth, they will eventually achieve binaural integration, in which case they will be able to stay with the clicking even at midline. This function is vitally important for users to enjoy the wider bandwidth responses in today's digital instruments, and to become more secure with their sound environment. Most cases will require ten or more sweeps before they develop a solid spatial map. - Ear-Training for Transcranial (Internal CROS) fittings: An effective alternative to traditional CROS fitting configuration is the Transcranial Method developed by this author and others over many years (Chartrand, 1999). It involves the fitting of an essentially "dead" ear so that the tactile perception of that ear will coincide with the auditory perception of the normal ear. Also, using an interaural attenuation chart, we can predict about how much sound from the amplified ear will reach the other (unamplified) cochlea via a common temporal bone. An important benefit of such a fitting is the elimination of the "head shadow effect" that typically plagues unilateral listeners, and also activation to some extent of their bilateral central auditory functions. A more complete protocol for this type of fitting may be found in a publication by Chartrand (1991). In short, tuning fork handle clicks are used much in the same way as the spatial mapping exercise described above (see Figure 9).
Admittedly, tuning forks are an every day part of the otolaryngological regimen. But these same skills plus some newer, more valuable ones, have been lost in everyday hearing instrument dispensing.
Unearthing and acquiring the skills of the lost art of tuning fork testing can serve a valuable purpose as a screening protocol. Such skills can inspire confidence in patients seeking answers to difficult-to-describe complaints. They can provide additional measurement and verification tools, and lay a foundation for more effective hearing instrument counseling.
This lost art can bring back into the armamentarium of the professional dispenser a measure of creativity, imagination, and resourcefulness to the art and science of hearing instrument dispensing. These skills, coupled with recent advancements in digital hearing aid technology, can go far in achieving greater fitting and post-fitting success for the recipient of our resurrected skills.
References
Chartrand, M.S. (1991). Transcranial or Internal CROS Fittings: Evaluation and Validation Protocol. The Hearing Journal, 44(9): 24-28.
Chartrand, M.S. (1999). Hearing Instrument Counseling: Practical Applications for Counseling the Hearing Impaired, 2nd Edition. Livonia, MI: international Institute for Hearing Instruments Studies, pp. 61-66, 144-145.
Chartrand, M.S. (2001). In Vigorous Defense of Volume Control. The Hearing Professional, May-June, 9-11.
Chartrand, M.S. (2003a). Another Elephant in the Living Room: To VC or Not to VC. The Hearing Review, March. Retrieved May 23, 2007, from www.hearingreview.com/issues/articles/2003-03_08.asp
Chartrand, M.S. (2003b). The Lost Art of Tuning Fork Testing. Colorado City, CO: DigiCare Hearing Research & Rehabilitation.
Feldmann, H. (1997). History of the Tuning Fork. Laryngorehinootologie, 76(2): 116-122.
