
Introduction
The clinical utility of videonystagmography (VNG) rests upon the accuracy of eye-tracking data. Traditional VNG systems utilize Earth-fixed targets—stationary monitors or light bars—that require the patient to maintain a rigid head position throughout the test battery. However, vestibular patients often struggle with head stability due to physiological compensation strategies and musculoskeletal comorbidities. This article explores the mathematical foundations of video-based eye tracking, the specific challenges introduced by head movement, and the clinical implications of transitioning from Earth-fixed to head-mounted targets. By utilizing head-referenced stimuli, clinicians can mitigate measurement errors, improve patient compliance, and ensure data integrity even when head stability is compromised.
Learning Outcomes
By the end of the course, participants will be able to:
- Identify the mathematical foundations of video based eye tracking.
- Discuss the challenges of head movement in the context of VNG testing.
- Describe the clinical implications of Earth fixed targets versus Head mounted targets.
Mathematical Foundations of Video Based Eye Tracking
To appreciate the necessity of precision in VNG, one must first understand the underlying geometry of the eye. While we often conceptualize eye tracking as a simple camera recording a pupil, the actual calculation of gaze direction involves complex mathematical modeling. We must account for the fact that the human eye is essentially a sphere that rotates within the orbit.
The measurement of eye rotation depends on two primary factors. The first is the displacement of the pupil across the visible surface of the eye. The second is the radius of the eyeball itself. In our clinical modeling, we assume the eye to be roughly spherical. When an individual shifts their gaze, the pupil does not move in a straight line; rather, it traces an arc on the surface of the eyeball. Video eye trackers capture this movement in pixels or millimeters and then use these values to estimate the angular rotation.
A significant challenge in this process is that the camera cannot observe the entire sphere of the eye. Because the eye is encased in skin and orbital tissue, only a front portion is visible. This visibility limitation is why calibration is non-negotiable in the clinical setting. Calibration serves as the bridge between the raw pupil position captured by the camera and the actual gaze direction of the patient. It allows the system to map how specific eye rotations correspond to the visual stimuli presented, such as a light bar or a projected dot.
Rotation of the Eye
Understanding the rotation of the eye requires a deeper look at the relationship between pupil position and the geometry of the ocular sphere. As the eye moves from a primary position to a secondary or tertiary position, the center of the pupil shifts relative to the stationary camera. The system calculates the degree of rotation by analyzing the arc length that the pupil has traveled.
If we visualize the eye suspended in space, we can see that every degree of rotation corresponds to a specific pixel distance on the camera sensor. However, the exact ratio of pixels to degrees varies between individuals because no two eyes have the exact same radius. This is why a universal setting is insufficient for medical-grade diagnostics. The software must determine the unique "R value" for each patient during the initial setup. Without this specific radius calculation, any subsequent measurement of eye speed or position would be an estimate rather than a precise diagnostic metric.
Calibration and the R Value
The calibration process is effectively a four-step mathematical synchronization.
1. Image Capture
In the first step, the video camera captures real-time images of the eye. The frame rate of the camera is crucial here, as higher frame rates allow for the capture of rapid eye movements like saccades without losing data points. The system identifies and tracks the precise center of the pupil.
2. Reference Point Identification
In the second step, we establish the reference point. We ask the patient to look straight ahead at a zero-degree target. This becomes our baseline or neutral point.
3. Known Angle Measurement
In the third step, the patient is asked to look at a target at a known angle, such as twenty or thirty degrees to the left or right. The system records this new pupil position.
4. Calculation of Delta Values
The fourth and most critical step is the calculation of the delta values. By measuring the distance between the zero-degree pupil position and the thirty-degree pupil position, the system determines the delta, which represents the displacement in pixels. This delta is used to derive the R value, which is the radius of the eyeball measured in pixels. This R value acts as a conversion factor. Once the R value is established, any future pupil movement during the test battery is fed into an algorithm that instantly translates pixel shifts into precise degrees of eye rotation.
If the calibration is performed correctly, the system will show equal pixel distances for equal degrees of movement. For example, a thirty-degree shift to the right should mirror a thirty-degree shift to the left in terms of pixel displacement. This produces a balanced and accurate interpretation of gaze direction.
Challenges of Head Movement in VNG Testing
While the mathematical model is robust, it relies on one fundamental assumption: that the head remains perfectly still throughout the calibration and the subsequent testing. In a laboratory environment, this might be achievable, but in a clinical setting, it is rarely the case.
Head movement is perhaps the most significant source of error in traditional VNG testing. Even minor, unintended shifts can introduce measurement errors that skew the final data. When we perform calibration, we are essentially locking the eye’s position relative to a stationary external target. If the patient tilts their head or shifts their weight in the chair after calibration, the "zero point" is no longer accurate.
The challenges of head movement are amplified in the very population we are trying to test. Patients with peripheral vestibular disorders often have a natural tendency to move their head rather than their eyes. This is a compensatory strategy intended to prevent retinal slip and the resulting sensation of dizziness. For these pathological patients, keeping the head still is not just an instruction; it is a physical and psychological challenge. Consequently, the individuals who need the most accurate diagnostic data are often the ones most likely to inadvertently sabotage the calibration through head drift.
Earth Fixed Targets versus Head Mounted Targets
To address these challenges, we must compare the two primary methods of stimulus delivery: Earth-fixed targets and head-mounted targets. Earth-fixed targets include stationary monitors mounted on walls, light bars, or projectors that display a stimulus onto a screen. In these systems, the stimulus is linked to the room. The patient wears goggles with cameras, but the target they are looking at is stationary in space.
The requirement for an Earth-fixed setup is rigidity. The patient must be positioned at a precise distance—typically four feet—from the light bar or monitor. This distance is a variable in the mathematical equation used to calculate the gaze angle. If the patient slumps or moves closer to the screen, the angle of the stimulus relative to the eye changes, but the computer continues to calculate based on the original four-foot assumption. This leads to an immediate mismatch between reality and recorded data.
In contrast, head-mounted targets represent a modern innovation where the stimulus is projected from the goggles themselves. In this configuration, the stimulus is locked to the patient's head. If the patient moves their head to the left, the projected dot moves to the left in perfect synchrony. Because the relationship between the eye, the camera, and the stimulus remains constant, the "zero point" is always referenced from the head. This setup effectively eliminates the errors caused by head drift during the test battery.
Real World Scenarios and Clinical Implications
Consider a scenario where a calibration is performed, but the patient’s head is inadvertently shifted by fifteen degrees. In an Earth-fixed system, this shift is catastrophic for data integrity. The system will misinterpret the pupil’s position, leading the algorithm to report incorrect eye angles. For a thirty-degree stimulus, the system might report twenty-six degrees on one side and thirty-one degrees on the other. This results in a measurable asymmetry of approximately eight percent. In the context of vestibular diagnostics, where we are looking for subtle asymmetries to identify pathology, an eight percent error introduced by head movement could easily lead to a misdiagnosis.
In the real world, patients fidget. They talk with their hands, they tilt their heads when listening to instructions, and they get tired over the course of a long test battery. A VNG session can last thirty to sixty minutes, and expecting a dizzy patient to remain perfectly immobile for that duration is unrealistic. When using Earth-fixed targets, the clinician often has to spend significant time re-instructing the patient or even physically holding the patient’s head to ensure stability. This is not only time-consuming but can also increase patient anxiety.
Head-mounted targets offer a more flexible clinical approach. Because the target moves with the patient, the clinician does not need to worry about the patient shifting in their chair or tilting their head. The setup is more dynamic and allows for a more natural interaction. This is particularly beneficial for pediatric patients, the elderly, or patients with complex needs who may not be able to follow strict "hold still" instructions.
Comparison of Gaze Data and Trace Alignment
When we look at comparison data between world-referenced (Earth-fixed) and head-referenced targets, the difference in data quality is striking. In an ideal scenario where the head is perfectly still, both systems perform well, and the eye trace follows the target trace accurately. However, as soon as we introduce a head position error—even as small as three degrees—the Earth-fixed data begins to deviate.
In saccade and smooth pursuit testing, head position errors in Earth-fixed systems cause a clear offset between the target trace and the eye trace. The red line representing the eye movement and the black line representing the target movement no longer overlap. On the head-referenced side, these lines remain perfectly aligned because the reference moves with the head.
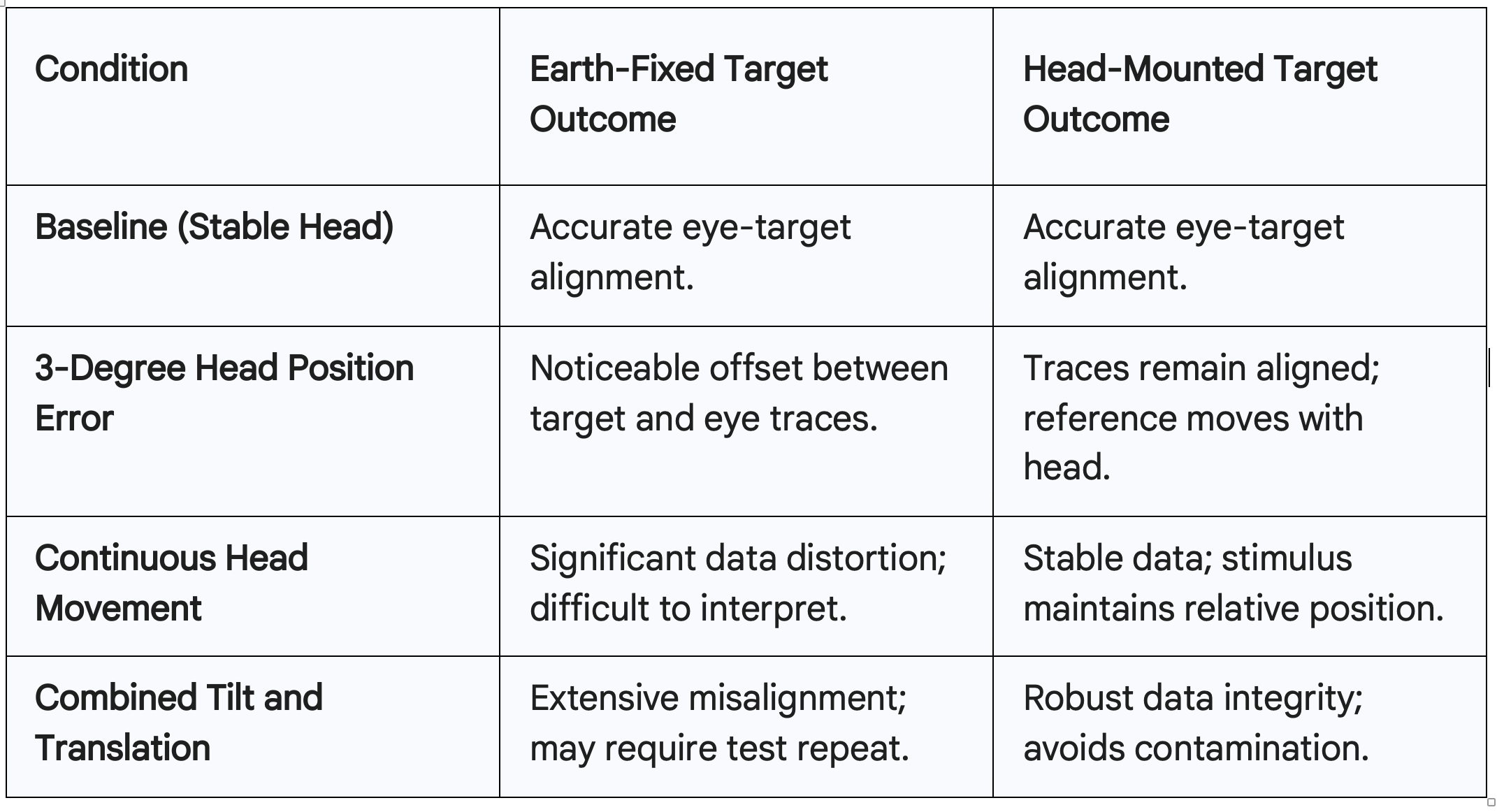
Figure 1. Clinical Data of Saccades vs Smooth Pursuit
When we combine multiple types of movement, such as tilting the head while also moving forwards or backwards, the Earth-fixed data becomes nearly unreadable. The traces show significant misalignment and distortions that could be misinterpreted as a central vestibular deficit or a lack of pursuit gain. A clinician looking at this "messy" data might mistakenly conclude that the patient has a neurological issue, when in reality, the data is simply contaminated by head movement. Head-mounted systems maintain stability and provide an accurate depiction of the eye's response, regardless of the patient’s postural shifts.
Clinical Efficiency and Patient Compliance
The transition to head-mounted technology significantly improves clinical efficiency. Traditional setups require a dedicated space with a fixed distance between the chair and the wall. The hardware is often bulky, consisting of light bars or large monitors that must be calibrated to the room. If a clinic needs to move the equipment, the entire spatial calibration must be redone.
A head-mounted system, such as the ICS Discovery, is much more portable. Because the stimulus is integrated into the goggles, the patient can be tested in various positions or even in different rooms without sacrificing accuracy. There is no need for a fixed four-foot distance to a wall. This "bedside" flexibility allows the clinician to bring the test to the patient, which is invaluable in acute care settings or for patients with mobility issues.
Furthermore, patient compliance increases when the testing environment feels less restrictive. Being clamped into a headrest or told repeatedly not to move can be an anxiety-provoking experience. By allowing the patient to move more naturally, the clinician can focus on the diagnostic results rather than the mechanics of the patient’s posture. This leads to faster testing times and a more pleasant experience for the patient.
Expert Demonstrations and Simulation Data
Professor Hamish McDougall’s research and simulations provide compelling evidence for the robustness of head-mounted targets. In virtual reality lab simulations, the impact of head movement on various test protocols is clearly visible. When performing horizontal smooth pursuit, a head-referenced stimulus ensures that the eye movements are recorded in relation to a stable, head-locked target.
In his demonstrations, Professor McDougall showed that even a conscious effort to keep the head still results in some degree of human error and micro-movements. In Earth-fixed systems, these micro-movements create noise in the data. When the head is intentionally moved to simulate a fidgeting patient, the Earth-fixed traces become a "mess," characterized by large offsets and unusable amplitude data. Conversely, the head-mounted data remains clean. The sinusoid of the eye movement perfectly matches the sinusoid of the stimulus.
These simulations prove that velocity analysis, while helpful, cannot fully compensate for the baseline offsets created by poor head positioning in Earth-fixed systems. To achieve true precision in VNG, the stimulus must be referenced to the same frame of reference as the eye-tracking cameras: the head.
Discussion and Clinical Considerations
The implementation of head-mounted VNG technology also raises practical questions regarding patient specificities. During the Q&A session, several important topics were addressed that further clarify the clinical application of this technology.
Torsional Eye Rotation and Nystagmus
A common question involves whether torsional eye rotation or spontaneous nystagmus interferes with calibration. While spontaneous nystagmus can pose a challenge, modern systems account for this by collecting data at a null point or using assumed averages to stabilize the calibration. Torsional rotation is also a factor, but the geometric algorithms are designed to prioritize the horizontal and vertical pupil centers, which are the primary metrics for standard VNG testing.
Published Norms and Algorithms
The "R value" calculation is not a proprietary or arbitrary number developed by a single manufacturer. It is based on universal geometric equations and published mathematical norms regarding the human eye. These algorithms are the standard for high-precision video eye trackers across the medical and scientific communities.
Musculoskeletal Issues
Clinicians often wonder if head-mounted systems are suitable for patients with musculoskeletal (MSK) issues, such as osteoporosis or neck stiffness. The consensus is that the choice between Earth-fixed and head-mounted targets does not change the clinical contraindications for the patient. If a patient cannot safely move their head for positional testing, that limitation applies regardless of the technology used. However, the head-mounted system is often easier for these patients because it does not require them to hold a specific, potentially uncomfortable posture relative to a wall-mounted monitor.
Slow Phase Velocity (SPV) Impacts
Accuracy in calibration directly impacts the calculation of slow phase velocity (SPV). If the calibration is poor due to head movement, the SPV values will be inaccurate. This is a critical point, as SPV is the primary metric used to determine the strength of a nystagmus response in caloric or positional testing. A systematic error in SPV could lead to an incorrect assessment of vestibular weakness.
Goggle Tension and Slippage
Finally, the physical setup of the goggles is essential. While VNG goggles do not need to be as tight as those used for video head impulse testing (vHIT)—because VNG does not involve rapid head thrusts—they must still be stable on the face. Proper positioning ensures that the cameras have a clear view of the pupil throughout the entire range of motion. Slippage can introduce "false" eye movements, so ensuring a secure fit is a fundamental step in any VNG protocol, whether head-fixed or Earth-fixed.
Conclusion
The evolution of VNG from Earth-fixed to head-mounted targets represents a significant step forward in vestibular diagnostics. By understanding the mathematical foundations of eye tracking—specifically the importance of the R value and the geometry of the eye sphere—clinicians can better appreciate how head movement compromises data.
While Earth-fixed targets have been the industry standard for decades, they are inherently sensitive to the realities of clinical practice, where patients move, fidget, and compensate for their dizziness. Head-mounted systems mitigate these challenges by ensuring that the visual stimulus and the eye-tracking cameras share the same reference frame. This leads to more robust data, fewer repeat tests, and a more efficient clinical workflow. As we move toward more dynamic and patient-centered diagnostic environments, the ability to navigate precision through head-referenced technology becomes an essential tool for the modern vestibular clinician.
References
Fazakeli, C. (2024). Global medical education manager perspectives on vestibular diagnostics. Natus Sensory.
McDougall, H. (2023). Head-referenced versus earth-fixed targets in vestibular diagnostics [Presentation]. Bahrani Society.
Morrow, S. (2024). ICS discovery VNG: Navigating precision in eye-tracking [Webinar transcript]. Audiology Online.
Natus Sensory. (2024). ICS discovery: Clinical user manual and technical specifications.

