
Learning Outcomes
After this course, participants will be able to:
- List individual factors influencing the benefit of a hearing aid fitting.
- Describe how the Hearing Profile fitting is realized in Connexx software.
- Describe the benefit offered by the Hearing Profile fitting.
Introduction
The usual practice when fitting a hearing aid (HA) is to adjust gain and output according to the patient’s audiogram. This is the most individualized part of the fitting process. Accordingly, the fitting software applies default settings of adaptive algorithms that are optimized to provide an ideal balance between speech understanding and sound quality. As a first fit, this works very well for many patients, but not for all. The term “hearing loss” describes a myriad of diagnoses and symptoms, not all of which are necessarily reflected in the audiogram (i.e. pure tone thresholds in quiet). Additionally, the adaptive parameters in the fitting software are optimized based on patient-averaged satisfaction ratings. These average settings are offered in the fitting software as the best starting point for the majority of patients, however they will not be suitable for all, as few people are precisely “average.”
It has long been known that pure tone audiogram (PTA) measurements cannot fully account for the variation in speech intelligibility scores measured from hearing impaired listeners (Smoorenburg, 1992). This implies that there are other patient-specific factors that influence speech understanding, and in particular speech understanding in background noise. The search for additional measures, which could enable us to move beyond audiogram-based fittings towards more individual fitting, have included research on age (Dubno, Dirks, & Morgan,1984, Gordon-Salant, 2005), audiogram type (Dubno, Eckert, Lee, Matthews, & Schmiedt, 2013), acceptable noise level and loudness tolerance (Nabelek, Freyaldenhoven, Tampas, Burchfield, & Muenchen, 2006; Mueller & Bentler, 2005), personality (Hutchinson, Duffy, & Kelly, 2005; Cox, 2006), cognition (Pichora‐Fuller, Schneider, & Daneman, 1995; Lunner, 2003; Lunner & Sundewall-Thorén, 2007) and various psychoacoustic measures such as frequency selectivity, temporal fine structure sensitivity and modulation thresholds (Hopkins & Moore, 2011; Bernstein et al., 2014).
The factors just listed serve to highlight the high complexity of hearing loss pathology. With regard to hearing aid fittings, it is clear that there is no simple solution that would allow us to perform a consistently perfect customized fitting by even adding one additional variable to audiogram data. Hearing loss is a dynamic process that changes with time, and how one hears depends on the hearing history of the individual. This hearing history depends on an interplay of many factors. If we want to understand the needs and wishes of an individual, we need to determine his individual experiences in different auditory situations.
A transition from the “average” patient fitting towards a more individual fitting requires several stages, which include:
- Identifying factors that describe an individual’s hearing problems and experiences, which are correlated with the amount of benefit provided by different hearing aid settings.
- Inferring relationships between these factors and hearing aid settings that maximize patient benefit from existing available subject database, and then making predictions of optimal HA settings for unseen patients, based on these inferred relationships.
- Designing a fitting software workflow based on factors listed in 1 and 2 (e.g., the Hearing Profile in the Connexx fitting software).
- Verification of the Hearing Profile fitting procedure.
In this paper, these stages are described and explained, based on data obtained from several clinical studies.
Individual Factors Influencing HA Benefit
The first stage in our individualized fitting investigation was to identify factors that significantly influence patient benefit with different hearing aid settings. For the hearing aid settings investigated, we identified nine such factors: PTA, age, tonal working memory, self-reported music listening habits, sensitivity to loud environments, outcome expectancy, hearing aid experience, conversation difficulty in challenging environments and attention difficulties.
Two groups of hearing aid parameter settings were investigated in the individualization studies, with each group ranging from moderate to strong settings.
1. Gain and Compression Settings (Figure 1)
- Setting A: relatively weak narrowband gain and compression.
- Setting B: moderate broadband gain and strong compression.
- Setting C: broadband gain and weak compression.
2. Adaptive Parameters Settings
- Setting D: mild noise reduction and weak adaptive directionality.
- Setting E: moderate noise reduction and adaptive directionality.
- Setting F: stronger noise reduction, moderate adaptive directionality and changes in compression parameters, in order to achieve stronger separation of target speaker and background.
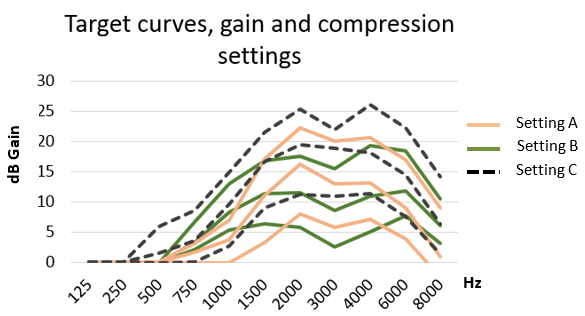
Figure 1. Connexx target gain curves for the three settings used in the Hearing Profile studies. The y axis shows gain (dB), the x axis shows frequency (Hz). Each setting is shown for three target gain curves for a 50, 65 and 80 dB input signal, for open acoustical couplings. The fitting was simulated for the N3 standard audiogram (Bisgaard, Vlaming, & Dahlquist, 2010).
It is important to note that none of the settings were extreme, since satisfaction was an important outcome measure from the start of our individualization investigations. Namely, the benefit of a hearing aid can be assessed through an objective measure (e.g. speech recognition performance) and through subjective satisfaction with the hearing aid. Often, we have found that the same individual factor influences both the performance and the satisfaction with the HA. The emphasis in this short overview is on hearing aid satisfaction.
PTA and Age
Pure tone audiogram and age are among the first factors that have been found to influence hearing aid benefit in hearing impaired adults (see Vestegaard Knudsen, Öberg, Nielsen, Naylor, & Kramer, 2010 for review). We found the PTA to be a significant predictor of HA satisfaction in terms of gain and compression settings.
Tonal Working Memory
The pitch between two talkers (e.g., a male voice and a female voice) allows the listener to separate the two voices (Darwin, 1997). It is this ability that allows us to single out someone’s voice from a group, thereby increasing the listener's probability of understanding this person. Equally important, the ability to memorize pitch may reflect aspects of verbal working memory, which has been shown to be an important factor in speech understanding in noise (Heinrich, Henshaw, & Ferguson, 2015). Finally, changes in pitch are an important factor in conveying speech information including prosody, emotion, speaker identification and meaning for tonal languages (Besson, Schön, Moreno, Santos, & Magneet, 2007). To assess the patient’s tonal working memory, we used a short tone test, which requires the patient to listen to up to six tones, and then compare whether the first and last tone are identical or not (Serman et al., 2017). This test was found to be a strong predictor of various important aspects of individual fittings, such as speech understanding in noise and the acceptance of frequency compression.
Music Listening
Musical activities can affect plastic changes in the auditory cortex in adulthood (Lappe, Herholz, Trainor, & Pantev, 2008; Pantev & Herholz, 2011), increase pitch discrimination (Spiegel & Watson, 1984; Micheyl, Delhommeau, Perrot, & Oxenham, 2006) and possibly give musicians an advantage in speech understanding in noise (Parbery-Clark, Skoe, Lam, & Kraus, 2009; Swaminathan et al., 2015; Lau, Ruggles, Katyal, Engel, & Oxenham, 2017). In our studies, music listening habits correlated significantly with preferences for gain and compression settings. We also found that frequent music listening positively influenced subjects’ speech in noise performance.
Sensitivity to Background Noise and Loud Environments
Loudness tolerance and noise sensitivity have the potential to influence hearing aid benefit both in terms of cognitive performance (Heinrich & Schneider, 2011) and HA satisfaction (Mueller & Bentler, 2005). Our investigations show that subjects sensitive to loudness had a significant drop in the acceptance of the mild adaptive parameters settings.
Outcome Expectancy
There is converging evidence that outcome expectancies and locus of control play an important role in predicting a hearing-impaired subject’s acceptance of hearing aids (Schum, Weile, & Behrens, 2011; Laplante-Lévesque, Hickson, & Worrall, 2012). Less research has been conducted regarding the role of expectations in satisfaction and performance benefit with different hearing aid settings. We investigated this aspect of HA-related expectations using the Health Action Process Approach (HAPA) model (Schwarzer, 1992; Fischer & Stromberger, 2016). The HAPA model divides health-oriented behavior into two consecutive phases: the motivation phase which then leads to the action (volition) phase. Applied to hearing aids, HAPA predicts that if there is a high self-efficacy and a positive estimation of the outcome of hearing aid use, an individual is more likely to wear and accept the hearing aids. We found a significant interaction between personality, outcome expectancy, and satisfaction with the adaptive parameter settings.
Hearing Aid Experience
Studies investigating the total lifetime use of hearing aids indicate a significant relationship exists between greater experience with hearing aids and higher satisfaction (Vestegaard Knudsen et al., 2010). In our studies, hearing aid experience was one of the factors that had a significant influence on gain and compression satisfaction.
Additionally, when comparing the results of the tonal working memory test in experienced and inexperienced hearing aid users across all of our individual studies, we observed that the outcome measures of the tonal working memory test for the inexperienced subjects significantly correlated with their age and with their hearing loss. Such correlation however was not observed for the experienced HA wearers. In other words, long-term hearing aid use assisted the patients in combating the effects of age and hearing loss on auditory cognitive processing (Serman et al., 2017).
Self-Reported Difficulties in Real-Life Communication Situations
Two questions in the questionnaire assessing self-reported hearing abilities in difficult listening situations were shown to be most important for determining hearing aid benefit: the ability to follow a conversation in a noisy restaurant; and, the ability to infer parts of the conversation that were not heard (glimpsing).
These questions are similar to the questions in the speech category of the SSQ self-report questionnaire (Gatehouse & Noble, 2004), which was shown to be significantly associated with speech perception performance in hearing impaired listeners (Heinrich, Henshaw, & Ferguson, 2016).
Our results show these two questions to be significantly and positively correlated with one another implying that people whose ability to follow and infer parts of conversation is more robust, will also have fewer problems in difficult, noisy situations. Regarding the acceptance of different settings, subjects preferring the stronger adaptive parameters setting over moderate settings were better at glimpsing than the subjects who preferred a moderate setting.
A summary of statistical correlations found for different individual factors and different hearing aid settings investigated is shown in Table 1.
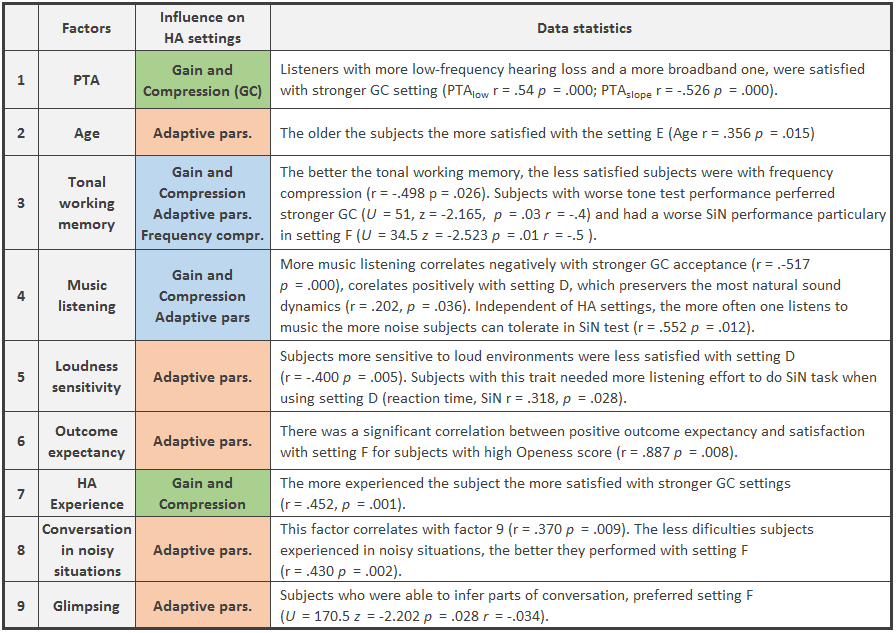
Table 1. Relations between Individual factors and hearing aid settings satisfaction. Reported are single correlations (r, p) and Mann-Whitney test results (U, z, p, r where r = z / √N is the size effect, N being the number of subjects).
The Matching Algorithm
The studies that we conducted showed that the interactions between the factors influencing hearing aid benefit and the hearing aid settings are numerous, complex and nonlinear, requiring a computational solution. The algorithm we determined to be best suited to learn these relationships from the data is the decision tree classifier, a type of machine-learning algorithm. On the basis of individual factors data and the associated hearing aid benefit, the classifier was trained to predict the hearing aid setting for a new patient. The result of this learning process is a set of rules that link the answers to individual questions and the hearing aid settings.
Connexx Hearing Profile Workflow
Traditionally, the design of hearing aid fitting software is heavily influenced by consideration of the time available to complete the fitting. The demands for both the hearing care professional and the patient require a simple but efficient procedure. Trends in the healthcare industry show a shift towards user-centered design, where the user and his experience becomes the focus of a successful intervention, even if such a workflow requires a longer time for completion (Gardien, Djajadiningrat, Hummels, & Brombacher, 2014). In fact, there is evidence that investing time in an activity results in greater emotional fulfillment (Mogilner, 2010), and greater feelings of personal connection to the product (Mogilner & Aaker, 2009), which may increase a patient’s motivation for wearing a hearing aid. Accordingly, the development of the Hearing Profile was guided by the complex factors that influence hearing pathology and the overall goal for a more patient-centered design.
The workflow was designed in such a way that the patient actively contributes to the fitting process. Since a hearing-impaired person’s experiences are shaped through a) the objective limits (inability to hear) and b) their subjective experience of these limits, the workflow engages the patient in assessing both. The patient is asked to complete a tonal working memory test (in a form of a short Sound Quiz), which together with the audiogram measurement and age data describes the objective hearing capacity of the patient. The Sound Quiz test was found to correlate significantly with self-reported problems in noise and with speech understanding in different types of noise. Since speech in noise problems are one of the most commonly reported problems for hearing impaired patients, such a test adds an important dimension to the assessment of the patient’s objective limitations.
The subjective experience and auditory history of the patient are assessed in the Hearing Profile by asking about experiences linked to individual factors, those which our background research revealed were most relevant for predicting hearing aid benefit with different settings. These questions are:
- Music listening: How often do you listen to music?
- Loudness sensitivity: Do you feel uncomfortable in loud environments?
- Outcome expectancy: Are you confident that newly fitted hearing aids will help you in your daily life?
- HA experience: How long have you been wearing hearing aids?
- Self-reported difficulties in real-life communication situations: When you sit together with a group of people in a busy environment (such as a crowded restaurant), can you follow the conversation? and, Is it difficult for you to concentrate on a conversation when you do not understand every single word?
We have strived to make the fitting workflow interesting and motivating, neither too easy nor too difficult, given the influence of age on the physiological and psychological abilities of the hearing impaired patients.
As mentioned earlier , two groups of settings were investigated; one group was related to gain and compression and the other was related to adaptive parameters. To make the workflow as short and efficient as possible, we designed five distinct hearing profiles out of the investigated settings. The hearing profiles differ with regard to a) the prescribed gain settings, and b) effective noise reduction and adaptive compression schemes (Figure 2).
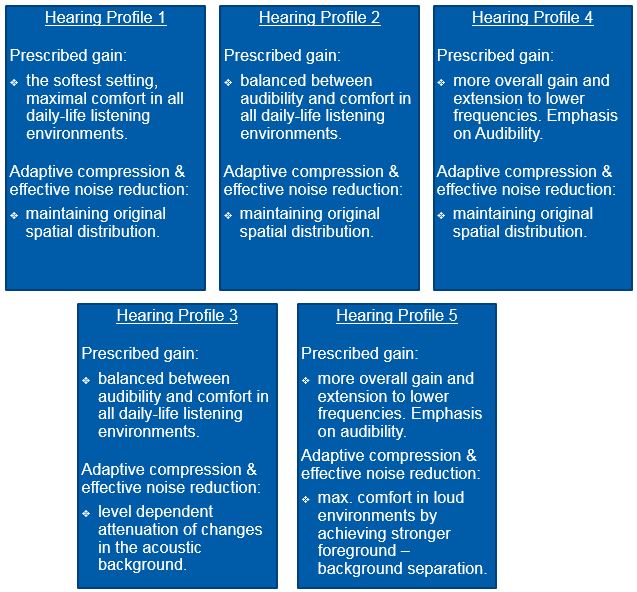
Figure 2. Five hearing aid settings used in the current Hearing Profile fitting.
Hearing Profile Verification
A series of studies were conducted during the development of the Hearing Profile First Fit. In one study with 78 subjects aged 28-87 years (M = 65.5) with an average hearing loss of 49.1 dB (125-4000 Hz), we compared satisfaction with the standard First Fit and the Hearing Profile Fit. Figure 3 shows the average satisfaction with the standard First Fit reaching “very good” satisfaction ratings. However, “hidden” in this average are 71% of subjects who are very satisfied with the standard fit, but there were 29% of subjects whose rating of the standard fitting was not very good. This latter subject group has different needs to the standard fitting parameterization optimized for “average” patients. Figure 4 shows a significant increase in satisfaction ratings of the 23 subjects who disliked the standard HA fit, when they were fitted using the Hearing Profile Fit (Wilcoxon signed-rank test: T = 18, p < .05, r = -.29).
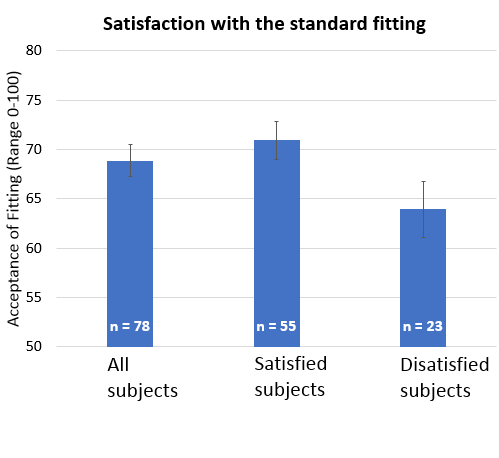
Figure 3. Analysis of satisfaction with the standard fitting.
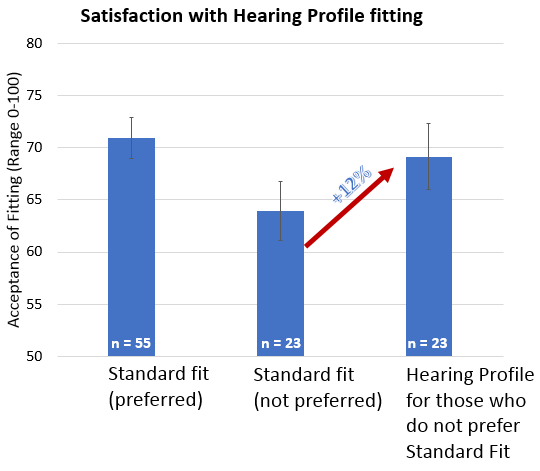
Figure 4. Comparison of satisfaction with the standard and Hearing Profile fitting. On average, subjects had a 12% increase in their hearing aid acceptance.
Apart from the subjective acceptance and satisfaction of a hearing aid setting, an important aspect of the fitting is speech understanding, especially speech understanding in background noise. In a separate study using thirty subjects, we measured speech in noise (SiN) performance with the standard fit and the individual fit suggested by the Hearing Profile. Additionally, electroencephalographic (EEG) measurements were performed on the subjects during speech in noise performance. The speech-in-noise test that was used was more cognitively demanding than traditional speech in noise tests: the subjects had to compare two digits and decide if the second digit was larger or smaller than the first one. The digits were embedded in audiobook snippets and cafeteria noise, with a positive signal to noise ratio.
There was no significant difference in the accuracy of speech in noise performance with the standard and the Hearing Profile Fit. However, we did observe changes in two additional SiN outcome measures.
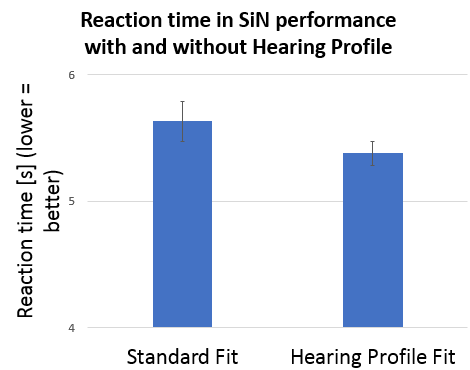
Figure 5. The reaction time outcome measure of the speech in noise test with standard and Hearing Profile fitting.
As shown in figure 5, the reaction time needed to perform each trial in the speech in noise (SiN) test dropped significantly when the SiN task was performed with the Hearing Profile fitting (paired samples t-test: t(29) = 2.141, p < .05). The reaction time in the cognitively demanding SiN setup can be interpreted as representing the cognitive effort needed to perform the task (McGarrigle et al., 2014). The faster reaction times indicate that while performing the SiN task with the hearing aid setting suggested by the Hearing Profile, the subjects had to invest less cognitive effort while maintaining the same performance accuracy. The implication of this finding for real-life communication situations is that these patients might be able to have an easier and possibly longer conversation in noisy environments.
Ongoing EEG recordings also were performed during the SiN task for both the standard and the Hearing Profile setting. The ongoing EEG can be recorded over a longer listening period so that it allows measurements of listening effort while the speech recognition task is being performed. The method we used for measuring listening effort assesses brain activity associated with early attention processes, which are relevant for orienting attention in noisy situations (OLEosc; see Bernarding, Strauss, Hannemann, Seidler, & Corona-Strauss, 2017). Figure 6 shows that the listening effort dropped when subjects were using the Hearing Profile Fit: the results are trend significant in the paired samples t-test: t (19) = 1.877, p = .076, with a medium-sized effect, r = 0.4. This result is consistent with the reaction time findings, and also has implications for real-life communication. Compared to the standard fitting, the Hearing Profile fit reduces the listening effort needed for attending to speech in a competing noise situation.
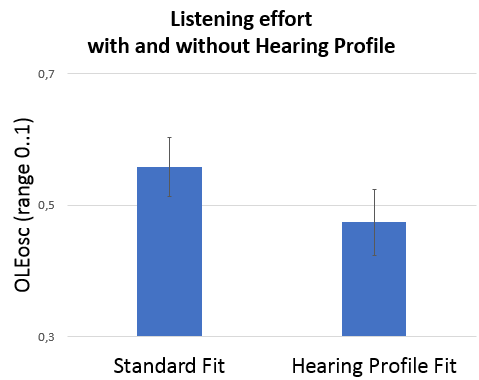
Figure 6. Listening effort during SiN performance, for two hearing aid fittings (x-axis). The y-axis shows the EEG-based measure of listening effort, OLEosc (Bernarding et al., 2017).
Conclusion
In this paper, we have outlined different stages that are necessary for the transition from a standard hearing aid fitting optimized for an “average” patient, towards an interactive, more individual fitting. In the first stage, individual factors influencing the benefit with different hearing aid settings were determined. The studies we conducted identified various factors, which interacted in a complex manner in relation to measurements of hearing aid benefit. The laws connecting the individual factors and hearing aid settings were therefore learned computationally, using the classification tree procedure. This algorithm learns to predict the preferred setting for any new set of individual data based on observed patterns it is trained with. The design of the fitting workflow in Connexx software was influenced by the overall goal to involve the patient in the fitting processes. This was achieved using an objective Sound Quiz and six questions related to subjective experiences of the patient’s hearing loss.
The verification studies show that the Hearing Profile Fit increased hearing aid acceptance for subjects originally dissatisfied with the standard fit. The study data also shows that the cognitive effort in a demanding speech in noise task and the listening effort measured by the ongoing EEG decreased when subjects were using hearing aids that were fitted with the Hearing Profile Fit in Connexx.
Acknowledgements
We are grateful to the subjects who participated in all studies leading to the Hearing Profile. Our thanks also go to Dunja Kunke, Steven Kalinke, Molly Henry and Jonas Obleser from the Max Planck Institute, Leipzig and to Daniel Strauss, Farah Corona-Strauss, Narsis Salafzoon, Corinna Bernarding, Patrick Schäfer and Philipp Flotho from the University of Saarbrücken. Without them all, this work would not have been possible.
References
Bernarding, C., Strauss, D.J., Hannemann, R., Seidler, H., & Corona-Strauss, F.I. (2017). Neurodynamic evaluation of hearing aid features using EEG correlates of listening effort. Cognitive Neurodynamics, 11(3), 203-215.
Bernstein, J.G., Mehraei, G., Shamma, S., Gallun, F.J., Theodoroff, S.M., & Leek, M.R. (2013). Spectrotemporal modulation sensitivity as a predictor of speech intelligibility for hearing-impaired listeners. Journal of the American Academy of Audiology, 24(4), 293-306.
Besson, M., Schön, D., Moreno, S., Santos, A., & Magne, C. (2007). Influence of musical expertise and musical training on pitch processing in music and language. Restorative Neurology and Neuroscience, 25(3-4), 399-410.
Bisgaard, N., Vlaming, M.S., & Dahlquist, M. (2010). Standard audiograms for the IEC 60118-15 measurement procedure. Trends in Amplification, 14(2), 113-120.
Cox, R. (2006, November). Personality of hearing aid patients: Be-fore, during and after the fitting. Hearing Care for Adults: An International Conference, Chicago, IL.
Darwin, C.J. (1997). Auditory grouping. Trends in Cognitive Sciences, 1(9), 327-333.
Dubno, J.R., Dirks, D.D., & Morgan, D.E. (1984). Effects of age and mild hearing loss on speech recognition in noise. The Journal of the Acoustical Society of America, 76(1), 87-96.
Dubno, J.R., Eckert, M.A., Lee, F.S., Matthews, L.J., & Schmiedt, R.A. (2013). Classifying human audiometric phenotypes of age-related hearing loss from animal models. Journal of the Association for Research in Otolaryngology, 14(5), 687-701.
Fischer R-L., & Stromberger, L. (2016, June). Social-cognitive predictors for hearing aid use. Poster presented at the HEAL conference, Cernobbio, Italy.
Gardien, P., Djajadiningrat, T., Hummels, C., & Brombacher, A. (2014). Changing your hammer: The implications of paradigmatic innovation for design practice. International Journal of Design, 8(2).
Gatehouse, S., & Noble, W. (2004). The speech, spatial and qualities of hearing scale (SSQ). International Journal of Audiology, 43(2), 85-99.
Gordon-Salant, S. (2005). Hearing loss and aging: new research findings and clinical implications. Journal of Rehabilitation Research and Development, 42(4), 9.
Heinrich, A., & Schneider, B.A. (2011). The effect of presentation level on memory performance. Ear and Hearing, 32(4), 524-532.
Heinrich, A., Henshaw, H., & Ferguson, M.A. (2015). The relationship of speech intelligibility with hearing sensitivity, cognition, and perceived hearing difficulties varies for different speech perception tests. Frontiers in Psychology, 6, 782.
Heinrich, A., Henshaw, H., & Ferguson, M.A. (2016). Only behavioral but not self-report measures of speech perception correlate with cognitive abilities. Frontiers in Psychology, 7.
Hopkins, K., & Moore, B.C. (2011). The effects of age and cochlear hearing loss on temporal fine structure sensitivity, frequency selectivity, and speech reception in noise. The Journal of the Acoustical Society of America, 130(1), 334-349.
Hutchinson, K.M., Duffy, T.L., & Kelly, L.J. (2005). How personality types correlate with hearing aid outcome measures. The Hearing Journal, 58(7), 28-30.
Laplante-Lévesque, A., Hickson, L., & Worrall, L. (2012). What makes adults with hearing impairment take up hearing aids or communication programs and achieve successful outcomes? Ear and Hearing, 33(1), 79-93.
Lappe, C., Herholz, S.C., Trainor, L.J., & Pantev, C. (2008). Cortical plasticity induced by short-term unimodal and multimodal musical training. Journal of Neuroscience, 28(39), 9632-9639.
Lau, B.K., Ruggles, D.R., Katyal, S., Engel, S.A., & Oxenham, A.J. (2017). Sustained cortical and subcortical measures of auditory and visual plasticity following short-term perceptual learning. PloS one, 12(1), e0168858.
Lunner, T. (2003). Cognitive function in relation to hearing aid use. International Journal of Audiology, 42, S49-S58.
Lunner, T., & Sundewall-Thorén, E. (2007). Interactions between cognition, compression, and listening conditions: Effects on speech-in-noise performance in a two-channel hearing aid. Journal of the American Academy of Audiology, 18(7), 604-617.
McGarrigle, R., Munro, K.J., Dawes, P., Stewart, A.J., Moore, D.R., Barry, J.G., & Amitay, S. (2014). Listening effort and fatigue: What exactly are we measuring? A British Society of Audiology Cognition in Hearing Special Interest Group ‘white paper’. International Journal of Audiology, 53(7), 433-440.
Micheyl, C., Delhommeau, K., Perrot, X., & Oxenham, A.J. (2006). Influence of musical and psychoacoustical training on pitch discrimination. Hearing Research, 219(1), 36-47.
Mogilner, C. (2010). The pursuit of happiness time, money, and social connection. Psychological Science, 21(9), 1348-1354.
Mogilner, C., & Aaker, J. (2009). “The time vs. money effect”: Shifting product attitudes and decisions through personal connection. Journal of Consumer Research, 36(2), 277-291.
Mueller, H.G., & Bentler, R.A. (2005). Fitting hearing aids using clinical measures of loudness discomfort levels: An evidence-based review of effectiveness. Journal of the American Academy of Audiology, 16(7), 461-472.
Nabelek, A.K., Freyaldenhoven, M.C., Tampas, J.W., Burchfield, S.B., & Muenchen, R.A. (2006). Acceptable noise level as a predictor of hearing aid use. Journal of the American Academy of Audiology, 17(9), 626-639.
Pantev, C., & Herholz, S.C. (2011). Plasticity of the human auditory cortex related to musical training. Neuroscience & Biobehavioral Reviews, 35(10), 2140-2154.
Parbery-Clark, A., Skoe, E., Lam, C., & Kraus, N. (2009). Musician enhancement for speech-in-noise. Ear and Hearing, 30(6), 653-661.
Pichora‐Fuller, M.K., Schneider, B.A., & Daneman, M. (1995). How young and old adults listen to and remember speech in noise. The Journal of the Acoustical Society of America, 97(1), 593-608.
Schum, D., Weile, J.N., & Behrens, T. (2011, March). New insights into first-time users. Presentation at annual meeting of the American Auditory Society, Scottsdale, AZ.
Schwarzer, R. (1992). Self-efficacy in the adoption and maintenance of health behaviors: Theoretical approaches and a new model. In R. Schwarzer (Hrsg.), Self-efficacy: Thought control of action (p. 217-243). New York, NY: Taylor & Francis.
Serman M., Kunke D., Fischer R-L., Obleser J., Kallisch K., & Hannemann, R. (2017, January) What can memory for tones tell us about hearing in noise? Poster presented at the SpiN workshop in Oldenburg, Germany.
Smoorenburg, G.F. (1992). Speech reception in quiet and in noisy conditions by individuals with noise‐induced hearing loss in relation to their tone audiogram. The Journal of the Acoustical Society of America, 91(1), 421-437.
Spiegel, M.F., & Watson, C.S. (1984). Performance on frequency‐discrimination tasks by musicians and nonmusicians. The Journal of the Acoustical Society of America, 76(6), 1690-1695.
Swaminathan, J., Mason, C. R., Streeter, T.M., Best, V., Kidd Jr, G., & Patel, A.D. (2015). Musical training, individual differences and the cocktail party problem. Scientific Reports, 5, 11628.
Vestergaard Knudsen, L., Öberg, M., Nielsen, C., Naylor, G., & Kramer, S.E. (2010). Factors influencing help seeking, hearing aid uptake, hearing aid use and satisfaction with hearing aids: A review of the literature. Trends in Amplification, 14(3), 127-154.
Citation
Serman, M., Fischer, R-L., Herbig, R., & Hannemann, R. (2017, July). Moving beyond the audiogram towards a patient-centered, interactive first fit. AudiologyOnline, Article 20493. Retrieved from www.audiologyonline.com




