The purpose of the course is to provide insights into the buying behaviors of consumers based on research findings in the fields of neuromarketing, which is a new field that has a lot of application to what we do in our clinics. Before we get into the topic today, I want to recommend a neuromarketing blog where scientists share their research findings and implications when it comes to buying and selling in a lot of different specialties, including hearing aids. Today's focus will be on some of the insights that come from the neuromarketing field and how they can be applied to clinical audiology practice. Today we will discuss buying behaviors of patients and customers, two terms that I will use interchangeably throughout this course. We will look at the differences in these behaviors both in theory and in practice.
We are going to look at this from two perspectives: the audiologist's point of view and the customer's point of view. We will first talk about the patient journey and what happens in the brain during the customer journey from the time that they think about coming to your office to the time they become a loyal customer. We'll look at what happens throughout that journey and some tools you can use to leverage those concepts. Toward the end of today's session we will talk about influence and some of the underlying behaviors involved with persuasiveness. There is an important caveat here when talking about the retail side of the business, and that is that we have to respect the psychological space of our patients. They have come a long way to get to the point of purchasing a hearing aid and have likely been through stages of denial or grief over their hearing loss. We need to use counseling techniques that are sensitive to our patients' varying situations.
Why Study Neuromarketing?
The first reason why it is important to study neuromarketing is that, in our profession, the majority of patients still have to pay out-of-pocket for services. Data from Kochkin (2009) tells us that, without contributions from the VA, only 30% of patients get some kind of third-party reimbursement. That means the other 70% are probably paying a significant amount out of their own pocket, and therefore have a choice as far as how they want to spend their money. This leads us to the second reason why it is important to study neuromarketing. Customers do have a choice of where they spend their hard-earned dollars. I am not talking so much about a choice between going to you or a competitor across town. Do they want to invest their money in better hearing or cosmetic surgery? Do they want to invest it in automobile or their grandchild's college tuition? We are hoping as hearing care professionals that they are going to raise their hand and decide to do business and spend their money with us rather than on some of the other options they have.
However unflattering it may be, many professionals equate selling with somewhat unsavory aspects of retail, such as the proverbial car salesman approach. We do not want to be connected with the negative characteristics of selling. There is a whole science to how people make a buying decision, and if we can embrace that, we can be more effective in our own clinics. Some of the typical behaviors of hearing care professionals are denial and avoidance. Some practitioners do not strongly embrace the retail side of our business, and some of this comes from just not having training in this area. We oftentimes do not want to embrace the fact that we do have to ask people to spend money out of their own pocket. One behavior that exemplifies this is lowering the price until someone buys. We know that in our type of business model, high margin, low volume oftentimes does not result in people agreeing to purchase from us. You also will see professionals over-talk on the technical details of what they offer. One of the side effects of over-talking is giving the patient too much information and not getting them involved in the process. They may need time and space to think it over instead of making a decision to purchase immediately with you. On the other end of the spectrum, it is easy for a smaller group of people to use high-pressure gimmicks to coerce people into buying, which we know is not good because those decisions are often regretted by patients, and that can lead to less-than-stellar satisfaction.
There are a lot of really interesting things that happen in the brain when someone walks into your clinic. Think about it from the perspective of someone who has had hearing loss for five to ten years and may have heard some negative things about how expensive hearing aids are and that they do not work. Maybe they read an article that was not very favorable towards hearing aids. That person carries all this stored information, and they walk into your clinic for the first time. Think about what happens at brain-chemistry level. The five senses are processing 11 million bits of information, which is 200 million billion neurological calculations per second. Only 3% of the body's weight is made up by the brain, yet it uses 20% of our body's energy. Keep in mind the brain is over 100,000 years old; rather, the way that it works is based on things that were happening over 100,000 years ago. There is as much emotional thinking going on as logical thinking when someone makes a buying decision. For much of human existence, the brain's primary focus has been to find food and shelter and avoid predators. My point is that some of those same thought processes from 100,000 years ago are still taking place today, and that is something we need to account for.
Lesson number one from neuromarketing is that any time you are reaching out to patients, any time you are trying to pull them in with your marketing, you want to make sure you are engage the primal brain and remember that attention spans are short. Those interactions with the primal brain need to be quick, concise and clear. Think about that caveman from 100,000 years ago trying to avoid the saber-tooth tiger. Some of the same instinctual qualities are taking place today when a customer walks into a clinic and they are somewhat suspicious and reluctant to do business with you. Therefore, you need to be interesting and engaging, and you need to find ways to appeal to positive emotions that activate the pleasure and reward zones of the brain.
Science of Neuromarketing
The science of neuromarketing includes looking at EEGs, functional MRIs (fMRI) and other biometric tools to measure what happens in the brain throughout the interaction between a customer and the vendor. One of the stories I have to tell about neuromarketing pertains to yogurt in the individual cups with a foil lid. There is a tremendous amount of neuromarketing science that has gone into where the pleasure zones of the brain are the most active throughout a customer's interaction with yogurt. Think about your interaction with yogurt as a consumer. You might see an ad on television. You might see a container in the store. You have some familiarity of the consistency, the taste and the creaminess of yogurt. From the time you pick up that container at the grocery store to the time you toss it in the trash after you have eaten it, what part of process activates the most brain activity? Believe it or not, neuroscience tells us that brain activity is heightened when a customer peels off the foil lid of the container. There is a reason why that lid is made of foil, because brain activity has been shown to be the most heightened with this medium. There is a whole science behind how tight that lid should be on the cup, how shiny it should be, how easy it should be for customer to peel it off. This is a nice example of how neuromarketing can be used to make very objective decisions about what you do in your interaction with customers. While specific neuroscience studies have not been performed in relation to hearing aids, there is a documented science behind customers' interactions with a product that we can use to guide us.
Another tip from the world of neuromarketing is the importance of a comfortable chair. Objective information collected with fMRI and EEG has shown that in the buying process people are much more likely to accept the recommendation and not haggle about price when they are in a comfortable chair. One study (Ackerman, Nocera, & Bargh, 2010) compared a group of customers who were put in very comfortable chairs to another group of customers that are put into a traditional hard wooden chair. They found that customers who were sitting in the comfortable chair were much more likely to agree with the seller's recommendation and not haggle on price as compared to the customers who were in the less comfortable chair. This same argument could likely have applications during hearing aid counseling and dispensing.
Ideas in Practice
For the remainder of the course, I want to focus on how we can apply neuromarketing ideas to an audiology practice. Let's first look at the customer's point of view and the journey into your office. An article by business professor David Edelman (2010) talks about the evolving customer journey in a digital era. He makes mention of the traditional marketing and sales funnel that is very passive in nature. In the traditional marketing and sales process, customers look at many brands through various mediums of advertising, narrow down the search to few choices based on a little research they have done, make a final choice and buy. The purchase transaction is the end of the journey or the interaction. What is happening more and more with the Internet, blogging, social networking and so forth, however, is what is referred to the customer decision journey, or loyalty loop (Edelman, 2010). In a loyalty loop, once a patient or customer decides to buy, it is not often the end of the relationship. Consumers today are extending their evaluation time as they consider or discard brands several times over. Once the customer has made a purchase, more times than not, they will go back to the Web site for more information or to share their experience. They may blog with other like minded customers, post on a forum, or write a review, and by so doing, they create a loyalty loop where the interaction begins with the buying process. What we do in hearing care is so much more than advertising. In the current landscape, you have to have tools in place to help you with the customer after the purchase transaction. Many of these tools are technology-based, but you should also take into account the demographic of your patients.
A slightly different variation of the customer journey is from a book called The Buying Brain (Pradeep, 2010). The author took his experience of working with several different businesses over a period of time to come up with seven different milestones along the customer journey. From beginning to end you have awareness, information, inquiry, consideration, purchase, enjoyment and advocacy. This model varies slightly from the Edelman (2010) model, yet there are many similarities. The main similarity is that once the patient purchases the product, they enjoy it until they ultimately become an advocate of the product. Let's look step-by-step at customer journey and talk about specific tools, tactics, and procedures we can use in the findings.
Customer Journey
Step number one of the journey is Awareness, and that is where the customer first encounters the service or product typically through advertising, exposure to articles or word of mouth. Step number two is Information, where you are pushing information to the customer. At this point, the customer is not asking for the information, but you are making it available. This is where you would use something like a Web site to push the information to the customer so that they can learn about what is available from your practice. The purpose of this stage is really to nudge the patient to want to learn more about you and how you might be able to help them.
Step number three is Inquiry, where you have now piqued the curiosity of the customer and he or she begins to ask a few more questions to learn more about you. This is where the customer is starting to become actively involved in the process of working with you. Keep in mind that the customer still has not come to your clinic yet, but is more active in engaging with you. Step four is Consideration. The customer is starting to consider purchasing a product or service from you, and so you are in the process now of indicating why the customer should work with you, rather than some other person who offers a similar service. This is where you might be able to create a sense of goodwill or obligation for the customer to do business with you rather than a competitor. Step number five is Purchase. This is really the first stage where the patient is interacting in a hands on fashion with your practice or physically coming in for an appointment. If you think about it, it is kind of interesting. Not until steps four and five does the patient come in to see you, but several steps prior to that the patient begins to form a relationship. Step five is the point where the patient makes a purchase. Another lesson from neuromarketing is that the process of parting with money is painful. In fact, some neuromarketing studies have shown through neuroimaging the same brain activity that you see from physical pain at the time when the physical transaction has occurred. With this in mind, what can you do to off set these feelings of painful payment?
Step number six is Enjoyment, or the act of finding pleasure from the product or service. That is very easy to realize in the world of sports cars. The enjoyment is almost immediate because, right off the lot they are fun to drive. Think about this in the perspective of hearing instruments, however, ask yourself: How can I make the process of interacting with the new purchase engaging, fun and pleasurable?
The final step in the consumer journey is Advocacy, where the patient is so enthralled with the product or service that he or she actually become an advocate for the practice and promotes your product and services to other people. Advocacy is a culmination of the successes through each of the previous six steps. The golden question is, "How can I use my knowledge of the seven steps of the customer journey to build a more effective clinical practice?" Let's look at that in more detail.
We are going to run through the seven steps of the customer journey again, but this time we are going to talk about specific tactics or tools you can use to make a more powerful journey for your patients.
Awareness
Again, awareness is where the patient first becomes cognizant of what you might have to offer. One of the tactics to share is that, from a customer journey perspective, it is probably dangerous to use price-point advertising. It is going to anchor a low price in the patient's mind, and instead you probably want to use advertising and marketing that focuses on the emotional impact of hearing loss. Concentrate on how the technology can transform a person from one who is struggling with communication to one who is an active participant in important communication situations.
Information
It is important to have an engaging Web site because, again, this is where you are pushing information to the customer. The use of short videos is a great way to engage the customer. Videos are also a personal way to get to know your practice. The take away message is if you have not updated your Web site in the last year or two, take advantage of some of the current tools that are easy to implement that will make your cyber-presence more interesting and engaging for your customer. Another way to draw some interest is by using a service like CounselEAR. CounselEAR creates easy tools for patients to help them understand and retain information pertaining to their hearing loss. Patients retain more information through the use of counseling reports and are more willing to follow up on the recommendations when they understand the importance of them. For more information, visit www.counselear.com
Inquiry
Inquiry is where the patient is beginning to ask questions to learn about you. One really interesting tool that is available to put in your waiting room would be digital marketing. Hearing News Network (www.hearingnewsnetwork.com) is a company that provides relevant information about your products and practice in the office. They feed information to a flat screen TV via the Internet (Figure 1). There is a ticker with current national news that that runs across the bottom. The margins broadcast local weather or news, while the main screen shows videos introducing your practice to the customer who is sitting in the waiting room. So rather than offering patients a four year old issue of a tabloid or even today's newspaper, now you have a video that interacts with the patient.
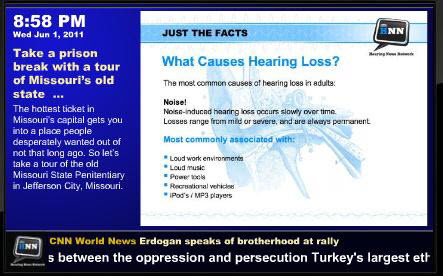
Figure 1. Sample screen of digital Hearing News Network feed.
Consideration
The customer is now actively considering purchasing your product or service. In your office, this may be a hearing aid evaluation appointment. One thing you can do to make that interesting to the patient would be to use what I call a memorable sales process that has two components: discovery and fulfillment. The purpose of the discovery process is to uncover the primary buying motivation of the patient and to have some tools to assess that motivation. If you have a 60 or 90 minute hearing aid consultation appointment, probably about 70% of that appointment needs to be the discovery phase where you are getting to know as much as you can about the patient. The other 30% of that is going to be the fulfillment stage where you are offering a recommendation.
The Discovery Phase
There is a study from our own profession talking about the science of selling. Catherine Palmer and colleagues (2009) published a paper about a tool to assess the motivation behind a hearing aid purchase. They asked one question to assess motivation: On a scale from 1 to 10, 1 being the worst and 10 being the best, how would awayou rate your overall hearing ability? If a patient gave herself a poor self-rating of one to five, that patient would have between an 80% and 100% chance of accepting the recommendation. The group that rated themselves in the middle at about a six or seven had about a 50% chance of agreeing to purchase hearing aids. If they said eight, nine or ten to that question, there was a pretty small chance that they considered themselves a candidate and were willing to accept your recommendation.
We can classify patients into three different categories. The patients who gave a rating of eight to ten are the patients in the first category to whom you probably need to provide educational information. They are not ready to make a purchase yet so you want to add them to a patient recall list that becomes part of your database. Schedule them for annual testing, and direct them to your Web site so that they have more information about hearing loss and hearing aids. The customer journey does not end with the patient saying, "I am not ready." Remember there are several more steps and the patient may stay in the Consideration phase for quite some time.
The patients who answered with a six or seven to the questionnaire probably need more information before they make a decision, so you could conduct a live demonstration and offer them a chance to test drive the hearing aids, perhaps for a trial period. These are the patients in category number two who can really be fence-sitters, so you want to utilize motivational interviewing techniques. Tap into that emotional side and activate the pleasure centers of the brain. An excellent reference regarding interviewing and the consultation process can be found on AudiologyOnline in the article Audiology and Motivational Interviewing: A Psychologist's Perspective by Michael Harvey (2003).
Lastly, in the third category are the patients who rated themselves from one to five and who you can likely move quickly into the hearing aid process. Give them information on performance, lifestyle, cosmetics, and cost. The take-home message is that we can help steer patients along that customer journey if we ask the questions that give us information about their own self-perception and readiness for help. The recommendations have to follow accordingly.
In today's world, it is easy to overwhelm patients with too much information. If you look at the science around this, there are actually studies that show that when you give a customer too much information it literally paralyzes the decision-making power of the brain. One thing that you can use to categorize priorities would be a buying habits matrix (Figure 2). Let's say that a patient coming into your office is in the third category and is motivated to move to the next step. In your own mind, assign that patient's buying habits or priorities to one of four quadrants.

Figure 2. Buying habits matrix.
They might love the way the device looks, or want something invisible like a mini CIC or open canal product. They might do business with you because they want the hearing aid that performs the best in challenging situations that they encounter every day. They are going to decide to do business with you based the best price point. Or they want a hearing aid that is easy to use or offers them a maximum amount of control. The buying habits matrix is nice way to realize that only a quarter of your patients truly make their decision primarily based on price. Your job as a clinician is to identify into which of the four quadrants does the patient fit, and then tailor the presentation accordingly. There is a nice tool that will help do you this called the COAT: Characteristics of Amplifications Tool (Sandridge & Newman, 2006). This was a questionnaire developed at the Cleveland Clinic five years ago. You can go to the article on AudioloyOnline and download and customize the questionnaire yourself.
The COAT asks nine questions about hearing aid preferences, ease of use, performance, cosmetics, even how much they are willing to spend. The authors of the COAT (Sandridge & Newman, 2006) say it is okay to modify the questionnaire so it fits in line with your practice, selection, and price points. The idea would be to administer the COAT while the patient is waiting to see you so you have an idea what the buying preferences might be ahead of time. In an era where we have so many different choices when it comes to hearing aids, the COAT is a nice way to narrow what is available to the patient. This is a tactic to use along with the buying matrix during the discovery phase of the appointment.
The Fulfillment Stage
There are seven stages to fulfillment that make for a very colorful sales acronym called RED DOOR: Review results, Educate, Demonstrate, Discuss options, Offer choices, Overcome any objections, Reassurance. We do not have time to go into the details, but there is a 60-page booklet that goes into detail if someone is interested, I would be glad to send you that booklet if you e mail me at [email protected]. Generally speaking, these are steps you can follow, sometimes out of order, to make sure the customer journey is fulfilling. One tip I wanted to share with you from the world of neuromarketing is that when fear is reduced, people are much more likely to make a clear choice. One thing we could do is review the consequences of untreated hearing loss and demonstrate to the patient how hearing aids can help. When we can reduce fear, it makes the buying process much more clear for patients. Show the patient in your office with a live hands-on demonstration how hearing aids can help, and when you do that, you are much more likely to reduce fear, and the patient is able to make a clear choice.
Purchase
Let's go back to stage number five where the patient actually makes a purchase. This is where they are actually going to have to agree to part with some money. What are some things that you can do to make this process as pain-free as possible for your patient? I have heard ideas about how you can make this into kind of a shopping spree for your patient where they can go and pick some of the sundry items that they need to use with the hearing aids. The point is you want to make this as pain free as possible for your patient.
Enjoyment
Point number six along the customer journey is Enjoyment. Again, we are not dispensing red sports cars so makes it a little more challenging for us to find ways to make it fun and pleasurable for our patients to interact with the product. I would leave it up to you to think of some creative ways to make the process of interacting with hearing aids fun and pleasurable for your patients in your own clinic setting.
Advocacy
The final stage, Advocacy, is where you want the patient to talk about and promote your practice. Sergei Kochkin was the lead author on an article in the April 2010 issue of the Hearing Review that discussed how the hearing professional can affect end-user success. One tool that has been proven to work is following a best-practices protocol and rewarding the patients who do promote your practice (Kochkin et al., 2010). The article documents how using a set protocol can drive word-of-mouth referrals and high levels of patient satisfaction.
The Professional Perspective
What kind of influence do you have in your practice? Being an influencer and persuasive in your clinic requires two things: communication skills and technical ability. To provide a visual representation of your own progress in each one of these two drivers, use a persuasiveness matrix. Both axes are labeled from zero to ten, with zero starting on the left and bottom sides of the matrix. The x-axis represents technical ability while the y-axis represents communication ability. Obviously, you would want to be in the upper right quadrant which corresponds to ten on both axes. You want to be eight or nine or ten on both technical ability and communication ability.
Let's look at the anatomy of consultative appointment. What happens during the consultative appointment? Figure 3 shows another matrix that is representative of what actually happens when you are in the office. On the horizontal axis you see intellect and emotion. Intellect in the appointment is very technically oriented. You talk a lot about technology and use terms and phrases that the patient may or may not understand. On the other end of that horizontal continuum is emotion. You are touching that primitive primal brain, trying to make the appointment more emotion-based through your dialogue while getting the patient involved. On the vertical axis you see at the bottom a passive appointment. That is kind of like a lecture where the patient is doing none of the talking and doing. Conversely, at the top of the vertical axis you see an active appointment where the patient may be very involved in the dialogue and conversation.
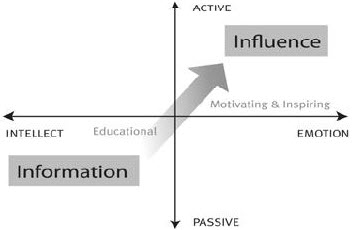
Figure 3. Appointment matrix to assess communication skills and technical ability.
In this matrix, the bottom left quadrant is very informational and educationally based, and is where most appointments fall. As you move towards the upper right quadrant, you motivate and inspire the patient in a way that makes them more actively involved. Allow the conversation to be more emotionally-based rather than intellectually-based. Ask the patient how they feel about the hearing loss or technology or about how they feel their hearing loss impacts their life as well as the lives of their loved ones. Talk about the emotions behind the motivation for seeing you.
The Six Weapons of Influence
The six weapons of influence is a concept that comes largely from the book Influence by Robert Cialdini (1984). Number one is Reciprocation: you scratch my back and I'll scratch yours. People do not like to be indebted to others and will often return favors. The second weapon of influence would be Commitment and Consistency. Once a person has made a formal commitment, they are more likely to follow through on it with their actions. It is the idea of a verbal contract. Number three is Social Proof. People are more likely to act when they see or hear about a similar person who likes or benefits from something. In everyday terms, these are testimonials. Weapon number four is Liking. People are more willing to accept a recommendation from people they genuinely like and feel comfortable with. Number five is Authority. People are more prone to act when influenced by the authority of others. Maybe this is reason why a lot of physicians and audiologists wear a lab coat. It projects the image of an authority figure, and we know that patients are much more willing to act if they view you as authority figure. The last weapon is something called Scarcity, which is really the idea of "act now while supplies last." This is where you attach a time limit to increase the value of something. One of the most popular scarcity tactics that people use are coupons that say you have until the end of the month to take advantage of a discount or service. There is a lot of great information in the book associated with these terms (Cialdini, 1984), and I encourage you to take a look if you get the chance.
Neuromarketing is an emerging science as it relates to our particular field, although there is documented validity in other specialties. There is a lot of carryover that can be applied positively in our profession.
Question & Answer
When allowing a patient to try the hearing aid out-of-office, do you believe there is more mental commitment if the patient leaves a deposit?
Yes. That goes back to the weapons of Influence and Commitment and Consistency. I think it makes all the sense in the world to have the patient leave deposit. Although it may be painful to offer up the deposit money, it is just a trial. But the mental seed has been planted, and they are much more willing to follow up with you if they have actually left the deposit.
Do you recommend moving from an informational to an influential discussion all during the first meeting or when they come back for the second visit?
That is a great question worthy of a lot of discussion. I do not think there is any solid answer on that. It really depends on the patient. No, you probably cannot always move somebody from information to influence over a one or two hour period of time. And, depending on where they are in the buying process, you may need a couple of visits.
At what point during the visit do you recommend administering the COAT?
I think the best time to administer the COAT would be when someone is coming in for a hearing aid consultation. You already know they are a fairly decent candidate, so you could have them complete it while they are waiting to see you. You can also administer it during the appointment face to face with the patient. Some people do it on a computer screen.
What other extra goodies would you offer as incentives?
Free batteries is a big one. Whatever you can afford to make the process engaging. Like I mentioned before, make it into a shopping spree. Since they may already be in a kind of "pain" from purchasing the hearing aids, let them pick out items to go in their bag when they leave. Instead of you providing everything in a bag, let them pick the items themselves. This makes it more interactive for the patient while still sending them home with necessities and extras for their hearing aids.
I want to thank everyone for their time. If there are any other questions, I would be glad to take those via e mail ([email protected]).
References
Ackerman, J.M., Nocera, C.C., & Bargh, J.A. (2010). Incidental hepatic sensations influence social judgments and decisions. Science, 328(5986), 1712-1715.
Cialdini, R.B. (1984). Influence: the psychology of persuasion. New York: William Morrow and Company.
Edelman, D.C. (December 2010). Branding in the digital age: you're spending your money in all the wrong places. Harvard Business Review. Retrieved June 1, 2011, from hbr.org/2010/12/branding-in-the-digital-age/ar/1
Harvey, M. (2003, October 20). Audiology and motivational interviewing: a psychologist's perspective. AudiologyOnline, Article 459. Direct URL: www.audiologyonline.com/articles/article_detail.asp?article_id=459
Retrieved June 2, 2011, from the Articles Archive on www.audiologyonline.com
Kochkin, S. (2009). MarkeTrak VIII: 25-year trends in the hearing health market. Hearing Review.16(11), 12-31.
Kochkin, S., Beck, D.L., Christensen, L.A., Compton-Conley, C., Fligor, B., Kricos, P.B., McSpaden, J.B., Mueller, H.G., Nilsson, M.J., Northern, J.L., Powers, T.A., Sweetow R.W., Taylor, B., & Turner, R.G. (2010). MarkeTrak VIII: The impact of the hearing healthcare professional on hearing aid user success. Hearing Review, 17(4), 12-34.
Palmer, C., Solodar, H.S., Hurley, W.R., Byrne, D.C., & Williams, K.O. (2009). Self-perception of hearing ability as a strong predictor of hearing aid purchase. Journal of the American Academy of Audiology, 20(6), 341-347.
Pradeep, K.A. (2010). The buying brain: secrets for selling to the subconscious mind. Hoboken: Wiley.
Sandridge, S.A. & Newman, C.W. (2006, March 6). Improving the efficiency and accountability of the hearing aid selection process - use of the COAT. AudiologyOnline, Article 1541. Direct URL: www.audiologyonline.com/articles/article_detail.asp?article_id=1541
Retrieved June 2, 2011, from the Articles Archive on www.audiologyonline.com