
Question
What is your protocol for fitting “low-gain” hearing instruments for slight and mild hearing losses (or for normal/near-normal hearing patients)?
Answer
Many clinicians are uncomfortable fitting slight and mild hearing losses with hearing aids. This may be because some clinicians feel that patients with borderline-normal hearing do not “need” hearing aids (or will not benefit from them), even if the patient has many perceived listening needs. However, I believe a large contributing factor is that some clinicians are not sure where to start when it comes to fitting patients who are in the near-normal range.
Since slight and mild hearing losses typically have only a very small negative effect on overall speech audibility, they require even greater attention than hearing losses that have more significant effects on speech audibility. The milder the loss, the more careful we need to be to ensure we are improving audibility and not inadvertently making it worse.
Of course, to maximize benefit and satisfaction from treatment with hearing instruments (for all degrees of hearing loss), it is necessary to use Real-Ear Measurements (REM) to measure the response of the hearing aid in the patient’s ear canal and make adjustments to match or approximate frequency-specific real-ear aided response (REAR) prescriptive targets.
But consider this: if a patient comes into your clinic with moderate sloping to moderately-severe hearing loss, you can safely “best-fit” any set of hearing aids (without running REM) and be pretty sure the patient is going to receive at least some benefit from them simply due to the drastic improvement in audibility they will receive, regardless of how well the devices are fit.
However, when fitting slight and mild losses, doing a “best-fit” without using REM to measure the response in the ear canal and make adjustments to improve the fitting, it is highly probable that you will be giving the patient a very expensive earplug, rather than a hearing aid. This likely contributes to why so many hearing aid fittings for mild losses end with a return-for-credit.
Often mild losses have a low-frequency component (see Figure 1); as such, we need to use a closed fitting to ensure benefit. But, closing off the ear disrupts the ear canal resonance (ECR). The ECR is extremely important with slight and mild loses because disrupting it can have a significant negative effect on audibility and perceived sound quality.
I have recently had a several colleagues reach out to me for help fitting slight and mild hearing losses and ask me about my process for these tricky fittings. Today I will share it with you.
Protocol for fitting slight/mild hearing losses (or for normal/near-normal hearing patients)
Goal
To provide a REAR for average speech, which exceeds (or minimally matches) the unaided response for the same speech signal (and does not fall below it) to ensure improved audibility, i.e. positive changes in the Speech Intelligibility Index (SII) values (aided-unaided).
Step 1: Measure unaided speech at an average level (65 dB SPL)
It is essential to know what the unaided speech response is if we want to know how the gain that the hearing aid provides causes the aided response to differ from it. The measured unaided speech response incorporates the patient’s ECR and should be run before anything else.
Step 2: Measure the aided speech response for average speech (65 dB SPL) and adjust the hearing aid gain to ensure the aided response surpasses (or at least matches) the unaided response for average speech across frequencies (see Figure 2).
Note: Prescriptive targets are a helpful guide to help understand what is “prescribed” for a mild hearing loss, but the milder the loss, the less relevant the targets are. For example, it is common for unaided responses to be over the aided targets, so use the measured unaided response for speech as your main reference for gain adjustments (while keeping an eye on the targets).
Tip 1: While autoREM is a great tool for more significant losses, a manual approach is necessary for fitting mild losses; autoREM will fit to target, which may create 0 % (or negative) improvements in SII values!
Tip 2: Do not blindly follow the manufacturer’s software recommendations for coupling / dome styles for slight/mild losses; often these models can recommend inappropriate coupling. For example, if you’re fitting a mild low-frequency loss, that rises to normal, the fitting software may suggest an open dome, but if you use an open dome, you will not be able to provide improved audibility in the low frequencies. Use your common sense.
Tip 3: In order to achieve the above outcome and obtain positive improvements in SII, it is very common for the simulated gain curves in the manufacturer’s software to be significantly over target after making the appropriate adjustments to the REM targets (see Figure 3). That’s OK; it’s the measured output in the real-ear that matters!
Step 3: Repeat the entire above process of soft speech (55 dB SPL).
Since soft speech is the most problematic for patients with slight and mild hearing losses, you should repeat the above process for soft speech. Note that SII change values will often be higher for soft speech, suggesting patients will notice more benefit for soft voices.
Conclusion
When you fit slight and mild hearing losses, you need to take even more care than you would when you are fitting hearing losses with more significant effects on audibility. While many clinicians may shy away from these fittings, with a clear understanding of your fitting goals and a protocol to follow, you can also assist individuals bothered by slight and mild hearing losses.
Case Example
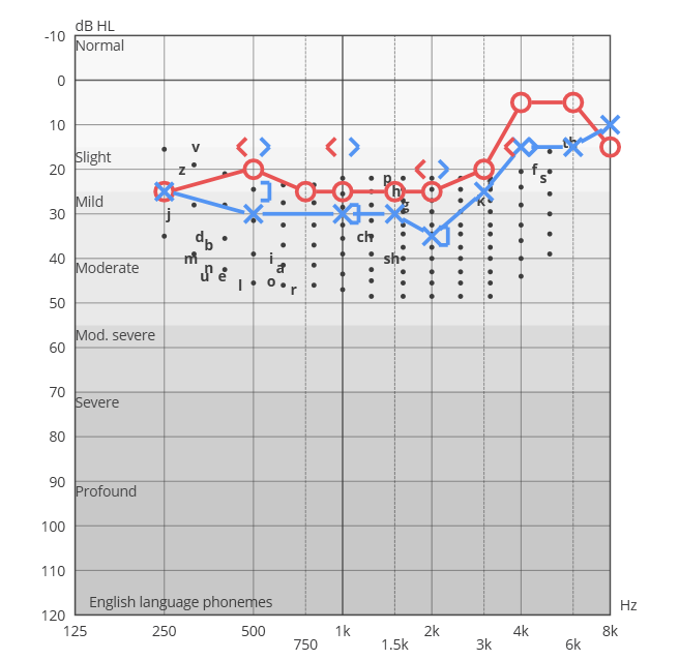
Figure 1. This image illustrates that mild losses exhibit a low-frequency component.
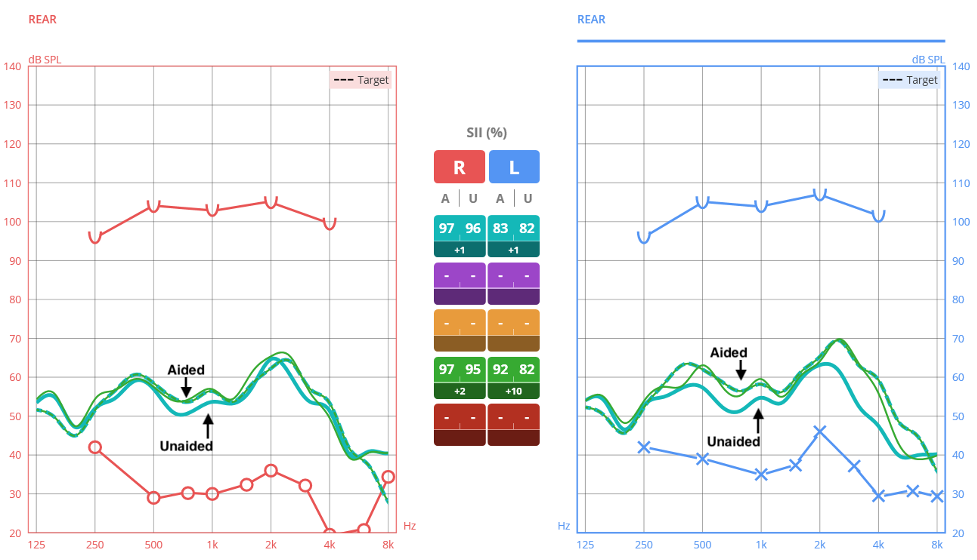
Figure 2. The image describes Step 2 of the protocol: it is necessary to measure the aided speech response for average speech (65 dB SPL) and adjust the hearing aid gain to ensure that the aided response surpasses (or at least matches) the unaided response for average speech across frequencies.
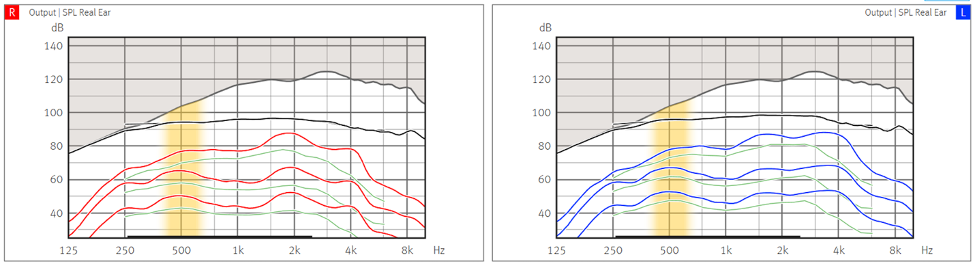
Figure 3. It is very common for the simulated gain curves in the manufacturer’s software to be significantly over target after making the appropriate adjustments to the REM targets.
Resources for More Information
For more information visit Inventis website https://www.inventis.it/en-na.
