
From the Desk of Gus Mueller
It’s been a while since Todd Ricketts and I have sat down and wrote an article together regarding probe-mic measures. It was back in 2006 when we discussed the importance of using stored equalization when conducting real-ear verification for open fittings (Open-canal fittings: Ten take-home tips). And then, three years later we reported on the probability of obtaining the same match to prescriptive targets when using four different probe-mic systems (Whose NAL-NL fitting method are you using?). So, after a decade’s hiatus, what prompted us to write something now?
Although it’s not really new, there has been increased interest in recent years regarding the automatic communication between the hearing aid fitting software and the probe-mic equipment during the hearing aid fitting. The notion is that if this communication is handled properly, the net result is a “fit-to-target” that is as good, or nearly as good, as what could be achieved manually by a clinician. We are calling this process autoREMfit. While this approach was once limited to only a couple hearing aid brands and one or two probe systems, it is now available from most major hearing aid and probe-microphone equipment manufacturers.
Fitting software that will fit your hearing aids for you? Almost sounds too good to be true, which is exactly why we wanted to look into it. We discuss a few issues that may need to be resolved but also present some findings that look promising.
As mentioned, Todd Ricketts, PhD, has joined me this month at 20Q. Todd is a professor at Vanderbilt Medical Center, Vice Chair in the Department of Hearing and Speech Sciences, and Director of the Dan Maddox Hearing Aid Research Laboratory. He is internationally known for his research regarding hearing aid technology and fitting applications, has served as editor of major audiology journals, and has been instrumental in the development of best practice guidelines for the fitting of hearing aids. Todd has been particularly busy the past five years, co-authoring four textbooks, the most recent of which is the comprehensive text, Essentials of Modern Hearing Aids - something every AuD student would want under their pillow (although it is 900 pages)!
We all know that real-ear hearing aid verification is essential. Yet, many audiologists are still reluctant to embrace this procedure. Will autoREMfit help to move the sticks? We hope so.
Gus Mueller, PhD
Contributing Editor
Browse the complete collection of 20Q with Gus Mueller CEU articles at www.audiologyonline.com/20Q
20Q: Hearing Aid Verification - Will AutoREMfit Move the Sticks?
Learning Outcomes
After this course, readers will be able to:
- Define autoREMfit and explain its purpose in hearing aid fitting
- Compare autoREMfit to hearing aid verification using other procedures such as speechmapping and in situ fit
- List and explain suggestions for maximizing accuracy when using autoREMfit for verifying hearing aids

Gus Mueller
1. I am not entirely sure what autoREMfit is?
Reasonable question. There is not a standard term for this procedure, so we pasted this one together. For starters, REM (pronounced “rhem”), stands for Real Ear Measure - essentially what we have been doing in the clinic since 1983. The “auto” part of it is that the probe-mic equipment and the hearing aid fitting software talk to each other. The hearing aid fitting software collects on-going real-ear information from the probe-mic system, and then makes changes in the hearing aid output, based on some preliminary measures, and measured ear canal SPL at the moment. The notion is that these automatic adjustments will make the fitting closer to a pre-selected prescribed target output, such as that of the NAL-NL2 or the DSLv5.0. The “fit” part of the term is that in theory, the resulting fit-to-target should be about as good as that which could be obtained manually by an experienced audiologist using the programming software. The assumed advantage is that you would get the job done faster, especially when conducting simultaneous bilateral fittings. Preliminary research suggests that this is true (Folkeard, Pumford, Kabirrah & Scollie, 2018).
We could just call it auto-fit, but that sounds like what the software does when you do “first-fit.” And we could just call it REM-fit, but that sounds like what is done when we fit to target using traditional probe-microphone measures. Now, if we find out it doesn’t really fit to the prescriptive targets we selected, we might have to change the name to autoREM-tried-to-fit.

Todd Ricketts
2. Do all hearing aid manufacturers use the same term?
Similar, but all somewhat different. The probe-mic manufacturers also have their own terms, but here is what we collected from four of the Big Six hearing aid companies that have this feature:
- Oticon: REM Auto-Fit
- Phonak: TargetMatch
- ReSound: AutoREM
- Signia: AutoFit
3. Is this the same as what some manufacturers call in-situ fit?
No, although some of the underlying goals are similar. With what is commonly called in-situ fit, the test signals are delivered by the hearing aid and measured by the hearing aid. The primary goal of this approach is to account for the real ear to coupler difference (RECD), and then apply these measured values to improve the accuracy of the fitting. One challenge regarding in-situ fitting techniques is that the signal level in the ear usually is estimated further away from TM than when we use probe-mic measures. With autoREMfit, all test signals are delivered and measured by the probe-mic equipment. You just need to place a probe-tip near the ear drum as you would for any other probe-mic measure.
4. I’m still looking at your title, what exactly does “move the sticks” mean?
We thought we’d toss out a popular football term that has carried over to general conversation (at least in our world). In football, whenever you get a new 1st down, the ten-yard-long chain that is along the sideline needs to be moved. Both ends of the chain are attached to sticks, so moving the sticks is an important sign of progress.
For the past 30 years or so, we have seen only minimal growth in the use of probe-microphone measures for hearing aid verification (Mueller, 2015). We’ve talked about all the reasons why this is true in other publications, so we won’t get into it here (Rickets, Bentler & Mueller, 2019; Mueller, Ricketts & Bentler, 2017; Mueller, 2014). Our thoughts are that maybe, this new feature will move the needle (or sticks) and get more audiologists excited enough to take a step forward, and start conducting real-ear hearing aid verification.
5. Is autoREMfit something new?
Not really - it has been around since the early 2000s. Originally, however, it only was available with the Siemens instruments/software, which had to be paired with the Unity probe-microphone equipment. That tended to limit widespread use. This fitting approach was somewhat popular in the UK, but never really caught on in the US. Other proprietary partnerships, for example, Med-Rx and Persona Medical hearing aids, were also introduced a little later. However, we’ve only seen relatively widespread implementation across manufacturers in the last few years.
The renewed interest mostly relates to the recent development by HIMSA of inter-module communication (IMC), protocol 2, commonly referred to as IMC2. This allows direct communication between Noah fitting software and Noah real ear measurement software. IMC2 allows the fitting software to control the communication process and data needed for these tasks can be transferred using the IMC2 protocol. This opens up cross-manufacturer communication so that now, a given probe-mic system could be compatible with the fitting software of most all hearing aid manufacturers. At the HIMSA website you can find a table which provides a listing of Noah certified modules, for both REM and manufacturer’s fitting software. We should mention, however, that it is possible to have an autoREMfit solution without IMC2; at least one hearing aid manufacturer and one probe-mic manufacturer are using a somewhat different approach.
6. Is this something that only is being promoted by the probe-mic companies, or are hearing aid manufacturers on-board with this fitting approach too?
Judging from the trade journal articles that we have seen, it certainly appears that the major hearing aid companies are encouraging the use of this verification process (e.g., Koehler & Kulkarni, 2014; Latzel et al., 2017; Beck & Crowe, 2017). Now, you probably know that in general, the word from most manufacturers is to use their proprietary fitting. So you might ask . . . why then would they encourage audiologists to verify? Well, with autoREMfit, you not only can fit to validated prescriptive methods (e.g., NAL and DSL), but, with some implementations, you also can fit to a given manufacturer’s proprietary fitting. This was not something that was easily possible in the past, as the proprietary targets were not available on probe-mic equipment. This could be one reason the procedure is being promoted by hearing aid manufacturers.
7. This all sounds great. Does this automatic procedure really work?
Maybe - it depends somewhat on what you mean by “work.” To us, that means that you would get the same fitting outcome as if the hearing aid had been programmed manually. So, let’s assume that you are an audiologist who follows best practice and for adults, your starting point is verified NAL-NL2 prescriptive method. You routinely conduct your verification using a calibrated speech input signal, such as the ISTS, with the real ear aided response (REAR) prescriptive targets as the fitting goal. You typically use inputs of 55, 65 and 75 dB SPL, and make adjustments so that the output is a close match to the real-ear targets - an approach often called “speechmapping.” To save a little time, you select NAL-NL2 in the manufacturer’s fitting software and do an autoREMfit. Will the results be the same? Or is fitting accuracy compromised?
8. Real-ear SPL is real-ear SPL. Why wouldn’t the findings be the same?
We can think of a least five reasons why they might not be, and there might be some other factors we haven’t thought of. Factors that could be in play include:
- Some autoREMfit procedures fit to the REIG, not the REAR. Additionally, they measure and use the individual’s REUG. Typically, we would fit to REAR targets that either do not consider REUG, or are based on an average REUG.
- Some of the autoREMfit procedures turn off all hearing aid features (e.g., digital noise reduction) during the fittings process; we verify with all special features “on.”
- This may not be true for the DSL, but for the NAL, we know that the manufacturer’s NAL-NL2 targets are not always the same as those generated by probe-mic equipment. Does the automatic procedure fit to the “manufacturer’s NAL” or to the “probe-mic NAL,” the latter of which we believe is the closest representation to the true NAL.
- Some of the autoREMfit methods only fit to a 65 dB input signal. Will there be a reasonable fit-to-target for soft and loud inputs using these methods?
- There of course always are possibilities of operator-error. When setting up autoREMfit, it is important that the audiologist select patient factors such as experience level, gender, etc, that then correspond to the parameters used to generate targets for traditional probe-mic verification.
9. That’s quite a list. I have time, how about some details?
Let’s start by going back to the example that we gave earlier. The protocol that most all audiologists (at least in the U.S.) use for real-ear verification is delivering shaped real speech and matching the output for REAR targets. When fitting to NAL-NL2, however, some of the autoREMfit procedures that we have seen, either use REIG targets or use REAR targets that are calculated based on REIG targets. In both cases, these systems measure the individual REUG (rather than using average), and these values are used in the fitting process.
In other words, you are forced to fit using a target that is calculated based on the REIG and individual REUGs. We all abandoned the REIG fitting method years ago. One of the reasons for abandoning it is because we know that if a person has an unusual REUG, and you use this to fit to REIG, you can end up with a very bizarre REAR/REAG. Since many autoREMfit procedures have no option for fitting using an average REUG, you could end up with a fit that is quite a bit different than what you get using the common speech mapping REAR approach.
10. Makes sense. On a related topic, I didn’t follow one of the things you said earlier. Did you imply that the manufacturer’s NAL-NL2 might not be the true NAL-NL2?
Yes, and there is research to support this going back many years (see Mueller et al., 2017 and Mueller, 2015 for review). Recently, this has been pointed out by Sanders, Stoody, Weber & Mueller (2015) and Amlani, Pumford, & Gessling (2017). For example, the Sanders et al. (2015) study examined the accuracy of the NAL-NL2 fitting for the premier hearing aids of the top five leading major manufacturers. When the simulated output in the fitting software was an exact match to NAL-NL2 target, individual speechmapping data for the 55 dB SPL input revealed that, in 59 of the 80 cases (74%), the measured output varied from the NAL-NL2 target by 10 dB or more for at least one frequency (250-4000 Hz). The largest error nearly always was at 3000 or 4000 Hz. Obtaining this amount of measurement error to REAR targets when the fitting software indicates a near-perfect match leads us to suspect that hearing aid manufacturers have tweaked the NAL-NL2 prescription. Note that we are only talking about the NAL-NL2 targets; the match might be better for DSLv5.
This is why it is important to know if autoREMfit is using the hearing aid software NAL-NL2 targets or the targets generated by the probe-microphone equipment. For this reason, one probe-mic manufacturer requires the use of their NAL-NL2/DSLv5 targets when autoREMfit is conducted.
11. Got it. Speaking of targets, I believe you said that autoREMfit can be used to fit to the manufacturer’s proprietary targets. Do you see this as a good thing?
Not really. There is considerable research showing that these proprietary fittings result in outcomes that are worse than those obtained with validated methods (see Ricketts et al., 2019; Mueller et al., 2017, for review). Why verify to something that does not result in an optimum outcome? One of the primary shortcomings of these algorithms is not providing enough gain for soft speech (Sanders et al., 2015; Valente, Oeding, Brockmeyer, Smith, & Kallogjeri, 2017), yet we know that appropriate gain for soft inputs is one of the significant factors driving success with hearing aids (Hickson, Meyer, Lovelock, Lampert, & Khan, 2014). We should mention that not all probe systems will allow for autoREMfit to proprietary fittings.
12. What about some of the other factors affecting accuracy?
In general, the remaining factors we mentioned probably do not lead to very different fittings compared to the use of standard techniques. In at least two cases we are aware of, the autoREMfit only matches targets to a 65 dB input. This, of course, is not desirable if you really want to fit to NAL-NL2 or DSLv5. However, we need to point out that even when using a careful manual approach, it is not always possible to match the REAR to soft, average and loud targets in some hearing aids due to compression architecture, including the use of slow release times (see Mueller et al., 2017 for a discussion). Consequently, in these products, attempting autoREMfit to soft and loud targets may not significantly improve the fitting accuracy. In addition, it is possible to calculate the relative change in output for soft and loud targets from the targets for a 65 dB SPL input. If a manufacturer does this very carefully as part of the fitting process, a good fit to 65 dB SPL targets might also result in a good fit to 55 and 75 dB SPL targets. We would want to verify that this really works on a couple of patients before relying on it clinically, though.
13. I’m not quite understanding why the “compression architecture” affects my ability to fit to target for multiple inputs?
The AGCi kneepoint can be a factor, but even if the kneepoint is low, compression release time may prevent you from obtaining a target match for a wide range of inputs. Consider that for a typical downward sloping hearing loss, for the NAL-NL2 prescription, REAR targets usually are separated by about 8 dB or so in the higher frequencies for 55 dB SPL vs. 75 dB SPL inputs. This means that if we first fit to our 55 dB SPL target, we would need an effective compression of the speech signal that was greater than 2:1 to match the target for the 75 dB SPL input. This isn’t going to happen with a long compression release (for review see Henning & Bentler, 2008). A compromise then would be to fit to average inputs, to minimize the overshoot for the 75 dB input, also knowing that then, soft inputs likely will be under-amplified.
Mueller (2018) discusses this in detail, and Figure 1 is an example taken from his article, which shows the effect we’re describing. This is the hearing aid output for a 75 dB real-speech input. A 50 dB compression kneepoint and a 3:1 compression ratio were used for all frequencies. This product has the option of selecting either a short (60 msec) or long (1800 msec) release time. The amplitude range of the input signal (30th to 99th percentile) was ~30 dB. Note that for the long release time, the range of the amplified signal is only minimally reduced from the 30 dB input range. With the short release time we see a greater “squash effect,” and the amplified LTASS drops by about 4 dB. From a practical standpoint, this illustrates that if the prescriptive target had been 87 dB at 3000 Hz, and there was initially an output 4 dB over target (green LTASS), a fit-to-target could be obtained by switching to a faster release time (red LTASS). Now, we do recognize that there are other factors that could prompt an audiologist to choose a slow release time, but for fitting to targets for multiple input levels, the best match typically will be achieved with a faster compression release.
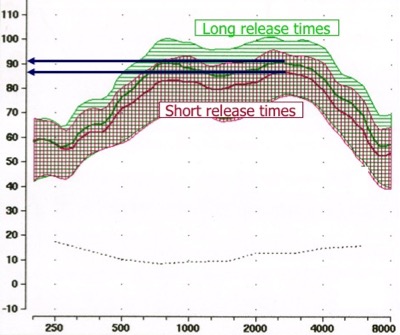
Figure 1. Illustration of the effects of changing the compression release time from 1800 msec (green shading) to 60 msec (red shading). For this example, the input signal was real speech at 75 dB SPL, the compression kneepoint was set at 50 dB SPL, and compression ratios were set at 3:1 for all frequencies. From Mueller (2018), used with permission.
14. You mentioned the importance of entering the correct patient experience level and gender. Does that really matter?
Yes. We’ll use an example provided by Earl Johnson in a 20Q article that he wrote back in 2012. There are two different patients: a woman obtaining her first set of hearing aids, and an experienced male user, obtaining a new set of hearing aids. They have the same hearing loss; 20-30 dB HL in the low frequencies sloping down to 70 dB HL at 2000 Hz and above. While their hearing loss is the same, the prescribed gain (output) in the high frequencies would differ by 6 dB. That’s probably big enough to make a difference. If we also include unilateral vs. bilateral fittings (another factor to be selected), then the differences could be even greater (for example, if the hearing aid was programmed for a bilateral fitting, but the probe-mic equipment is showing targets for a unilateral fitting). It’s the old apples to apples thing - it’s critical that all the parameters in the fitting software agree with the parameters used to generate the targets that appear on the probe-mic monitor.
15. Overall, listening to all the things that could affect autoREMfit, you still have me wondering if it really works? You haven’t really answered that question.
There is very little independent research on the topic. A recent paper from the University of Western Ontario, verifying to the DSL5.0, did report encouraging findings for one implementation (Folkeard et al., 2018). We have yet to complete a formal study, but we recently did collect some pilot data with a limited number of subjects. We used the same probe-mic equipment for all the testing (Otometrics Aurical) and conducted autoREMfit for the four different major manufacturers that have software integration with the Aurical: Oticon, Phonak, ReSound and Signia. We used the same “easy-to-fit” audiogram for all participants - a gradually downward sloping loss going from 30 dB in the low frequencies to 60 dB in the highs. We selected the NAL-NL2 for an experienced user, bilateral fitting, in the fitting software.
Using the step-by-step method provided by each manufacturer, we first did the autoREMfit. Once this was completed, leaving the hearing aid and probe tube untouched, we conducted REAR speechmapping using the ISTS for inputs of 55, 65 and 75 dB SPL. Our interest was in observing how close the autoREMfit was to the NAL-NL2 fitting targets generated by the probe-mic equipment. If the fit was similar to what an audiologist could obtain through manual programming, then indeed autoREMfit would be a more efficient way of getting the job done.
16. What did you find?
For three of the four manufacturers, the findings were encouraging. As we mentioned, we only conducted testing on a limited number of subjects, but for these manufacturers, the results were quite consistent. Illustrative examples are shown in Figure 1. What you see in Figure 1 are the findings for three different manufacturers for one ear of a single subject. Each individual panel shows the findings for all three manufacturers. The findings for the 55 dB input are shown in the top panel, 65 dB input is the middle panel, and the 75 dB input is the bottom panel. Shown are difference curves, that is, the deviation from NAL-NL2 targets. Above the horizontal center line means more gain than targets, and below the center line is less gain than the targets. As you can see from the middle and bottom panels, all three manufacturers do a reasonably good job of being close to targets for the 65 and 75 dB SPL inputs. For the 65 dB SPL input targets, two of the three manufacturers are within about 3 dB for all frequencies from 250 through 5000 Hz. While also quite close, the fit for Manufacturer B consistently falls around 2 to 5 dB under the targets. Our guess is that this manufacturer’s NAL-NL2 fit might be a little different than the true NAL-NL2, resulting in this difference (something we talked about earlier).
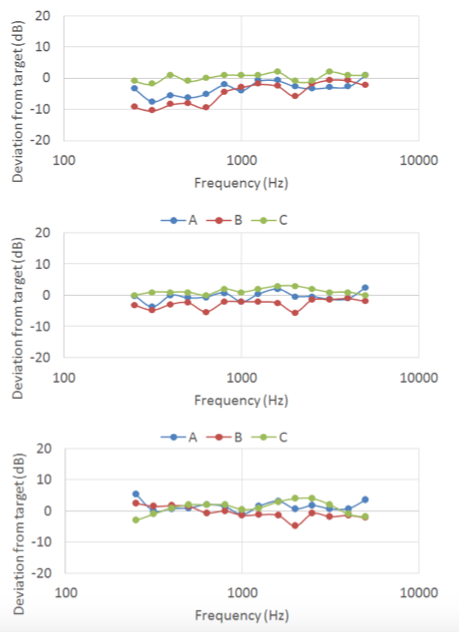
Figure 2. Illustrative findings for autoREMfit for three different manufacturers. Each individual panel shows the deviation from NAL-NL2 targets for all three manufacturers for a single input level: 55 dB SPL input (top panel), 65 dB SPL input (middle panel) and 75 dB SPL input (bottom panel). Above the horizontal center line indicates more gain than prescribed targets; below the center line is less gain than the targets.
17. There seem to be bigger errors for the 55 dB SPL input across manufacturers. What do you think is causing that?
Our guess is that this relates to the compression limitations that we described earlier. If you look at all three panels, you can see that Manufacturer C (Green), really hits the targets for all three input levels very closely. In contrast, while still a pretty good fit, Manufacturer B (Red) is more spread out. Specifically, the REAR falls below targets for the 55 dB input, particularly for the lower frequencies. While this could be an error in the fitting, it is also possible, and perhaps likely that this product applies compression that does not allow for an effective compression ratio as high as prescribed by the NAL-NL2. All in all, for this particular patient, the fittings were quite good; they were within 5 dB for most frequencies at most levels for all three manufacturers. We should mention that this patient had a relatively average REUG.
18. What about the fourth manufacturer, how was that fitting?
Not good. The match to target was off by 10 dB or more for all input levels. This wasn’t ear-specific, as we saw the same error for several participants. Of course, you would never know the error was there unless you cross-checked against traditional techniques or other equipment, which is why we did this testing to begin with. The on-screen display showed a near-perfect match to target.
After noticing this error we contacted the manufacturer directly. They did a little hunting and reported back to us that they found they indeed had been making an error related to the off-set applied when calculating targets for speech test signals. They were, of course, very interested in correcting the error and shipped out beta software with a correction. We piloted this new software on a few more people and found it did fix the problem. The update should be pushed out in the manufacturer’s fitting software by the time you read this article. This is a good example of why it is very important to update your software whenever a new version is released. Curious minds, however, also wonder why we were the first to report this, given that this autoREMfit implementation had been out for some time?
19. Will keep that in mind. You earlier mentioned the use of individual versus average REUGs. How much of an issue is that, really?
There was a lot of discussion regarding the use of measured vs. average REUGs in the early 1990s when it was popular to use the REIG for verification (e.g., Revit, 1991; Mueller 1992). In case you missed those discussions, here is an illustration of the differences you might find. We first completed an autoREMfit for a patient with a mild-to-moderate downward sloping hearing loss (see ear canal SPL thresholds in Figure 3). We purposely selected someone who had an unusual REUG. Normally we would expect an REUG peak of around 17 at 2700 Hz - his peak was at 2000 Hz and was around 25 dB. Where we would normally see a concha effect of around 10-12 dB at 4000 Hz, his REUG was only a few dB. The autoREMfit procedure we used requires the use of the measured REUG. The on-screen fit to the REIG target was excellent.
We then cross-checked for a match to REAR targets using traditional speechmapping for a 65-dB real-speech input. The results are shown in Figure 3. The dark blue dashed line is the NAL-NL2 prescriptive targets, and the lighter blue and red intertwined lines (test/retest) are the measured REARs.
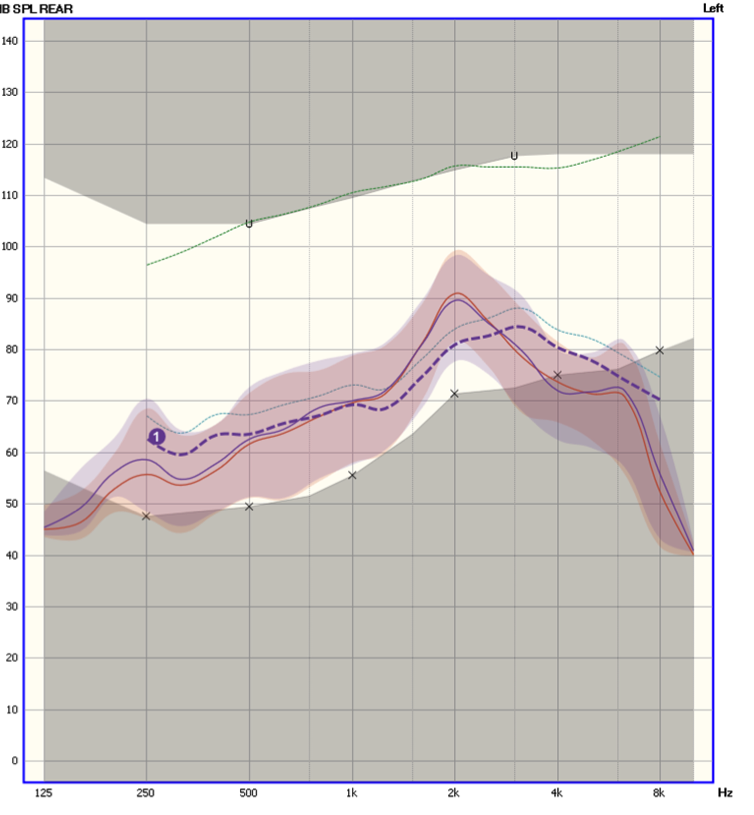
Figure 3. REARs for a 65 dB SPL real speech input following autoREMfit. The dark blue dashed line is the NAL-NL2 prescriptive targets, and the lighter blue and red intertwined lines (test/retest) are the measured REARs. The shaded area represented the 30th to 99th percentile of the amplified speech signal. The X’s below the dashed blue line are the patient’s thresholds converted to ear canal SPL.
Most any audiologist would consider this an unacceptable fitting. Note that the REAR is about 10 dB over the prescriptive target at 2000 Hz and about 7 dB under target at 4000 Hz. This, of course, is what you’d expect when correcting for the unusual REUG we described - the only way to obtain an REIG target match is to introduce an amplified speech output that to some extent mimics the measured REUG, which leaves you with a very unusual amplified LTASS at the ear drum. There are experts that believe that this is the best way to fit hearing aids but we don’t agree.
20. Bottom line - do you think that autoREMfit will indeed move the sticks?
We hope so. As we’ve already stated, considerable research shows that patients have the best chance of receiving optimal benefit, while maintaining listening comfort, when fitted to a validated prescriptive method (NAL-NL2 or DSL v5), verified using probe-microphone techniques. If autoREMfit encourages audiologists to do this, that's great! However, accuracy is important. We certainly would not want to sacrifice accuracy just to save a few minutes of test time. Our recommendations for autoREMfit implementation, therefore, would be:
- Use the NAL-NL2/DSLv5 targets of the probe-mic equipment, not those of the hearing aid fitting software.
- Fit to REAR targets using real-speech inputs.
- As best as possible, also fit to soft and loud speech targets, in addition to average speech inputs.
- If a fit to REIG targets is part of the implementation, provide the option of using an average REUG.
References
Amlani, A.M., Pumford, J., & Gessling, E. (2017). Real-ear measurement and its impact on aided audibility and patient loyalty. Hearing Review 24(10), 12-21.
Beck, D.L., & Crowe, N. (2017). Easy, fast, and accurate: Hearing aid fittings via an automated REM system using IMC 2. Hearing Review, 24(4), 30-31.
Folkeard, P., Pumford, J., Kabirrah, P.A., & Scollie, S. (2018) Linking Audioscan Verifit with Oticon Genie: Comparison of manual and automatic hearing aid fittings. Paper presented at the American Academy of Audiology Conference, Nashville, TN.
Henning, R.L. & Bentler, R.A. (2008). The effects of hearing aid compression parameters on the short-term dynamic range of continuous speech. Journal of Speech, Language, and Hearing Research, 51, 471-484.
Hickson, L., Meyer, C., Lovelock, K., Lampert, M., & Khan, A. (2014). Factors associated with success with hearing aids in older adults. International Journal of Audiology, 53(Suppl 1), S18-27.
Johnson, E. (2012, April). 20Q: Same or different - Comparing the latest NAL and DSL prescriptive targets AudiologyOnline, Article 769. Retrieved from www.audiologyonline.com
Koehler, E.E., & Kulkarni, S. (2014). Fast and easy fitting and verification with integrated real-ear measurement. Hearing Review, 21(10), 36-40.
Latzel, M., Denys, S., Anderson, S., Francart, T., Wouters, J., & Appleton-Huber, J. (2017). An integrated REM system with proven accuracy and reliability. Hearing Review, 24(10), 36-39.
Mueller, H.G. (1992). Individualizing the ordering of custom hearing aids. In Probe microphone measurements, H.G. Mueller, D.B. Hawkins, & J.L. Northern (Eds.). San Diego: Plural Publishing.
Mueller, H.G. (2014). Real-ear probe-microphone measures - 30 years of progress? AudiologyOnline, Article 12410. Retrieved from: https://www.audiologyonline.com
Mueller, H.G. (2015, May). 20Q: Today's use of validated prescriptive methods for fitting hearing aids - what would Denis say? AudiologyOnline, Article 14101. Retrieved from https://www.audiologyonline.com
Mueller, H.G. (2018, January). Hearing aid speech mapping verification - some explanations for puzzling outcomes. AudiologyOnline, Article 21062. Retrieved from www.audiologyonline.com
Mueller, H.G., Ricketts, T.A., & Bentler, R.A. (2017). Speech mapping and probe microphone measurements. San Diego: Plural Publishing.
Revit, L. (1991). New thinking on the proper application of the real ear unaided response measurements to prescriptions and fittings. New Zealand Audiological Society Bulletin, 1, 1-17.
Ricketts, T.A., Bentler, R.A., & Mueller, H.G. (2019). Essentials of modern hearing aids. San Diego: Plural Publishing.
Sanders, J., Stoody, T., Weber, J.E., & Mueller, H.G. (2015). Manufacturers’ NAL-NL2 fittings fail real-ear verification. Hearing Review, 21(3), 24-32.
Valente, M., Oeding, K., Brockmeyer, A., Smith, S., & Kallogjeri, D. (2017) Differences in word and phoneme recognition in quiet, sentence recognition in noise, and subjective outcomes between manufacturer first-fit and hearing aids programmed to NAL-NL2 using real-ear measures. Journal of the American Academy of Audiology. https://doi.org/10.3766/jaaa.17005
Citation
Mueller, H.G., & Ricketts, T.A. (2018). 20Q: Hearing aid verification - will autoREMfit move the sticks? AudiologyOnline, Article 23532. Retrieved from www.audiologyonline.com


