
Introduction
Cerumen removal or cerumen management (CM) has been within the audiologist's scope of practice since 1992 (ASHA, 1992). CM is necessary when excessive or impacted cerumen results in insufficient access to the ear canal, creating a blockage of sound and possibly hindering audiological measurements. Specifically, excessive cerumen can potentially result in misleading and/or inaccurate audiologic results and interfere with hearing instruments (CASLPO, 2005;Gleitman, Ballachanda, & Goldstein, 1992).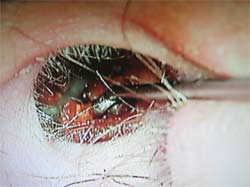
Figure 1. Visual of cerumen management
One option for CM, otomicroscopy, provides superior illumination and magnification and gives the clinician the freedom of both hands to operate. However, even though the advantages of CM using otomicroscopy as compared to simple otoscopy or video-otoscopy are well accepted (Ballachanda, 1995;Courtois, 1999), audiologists in general have not incorporated microscopes into their practices. This is partially due to perceived high cost (Purdy, 2002) and lack of required training to effectively use an operating microscope (Ballachanda, 1995).

Figures 2 and 3. Examples of microscopes used for otomicroscopy
This paper calls into question both of these notions. Although the cost for a new wall or floor mount microscope is approximately $7000.00, used microscopes are available for much less. Therefore, contrary to past opinions, otolaryngology style microscopes are not unaffordable by the average private practice audiologist. Furthermore, learning to use a microscope is neither difficult nor requires extensive training. This paper has two purposes:
- Encourage audiologists who are faced with ceruminosis as a common complicating factor to consider the value of microscopy in their practices (i.e., using the best equipment available), and
- Encourage companies selling smaller operating microscopes to view audiologists, especially those in private practice, as a potentially viable market similar to otolaryngologists and dentists.
Survey of Current CM Methods by Audiologists
To determine the typical audiologist's views about microscopes, I conducted a small survey of 25 audiologists and audiology students at the 2008 American Academy of Audiology meeting in Charlotte, North Carolina. Sixty-eight percent of those interviewed stated they perform CM on a routine basis. Of those performing CM, 40% stated they use a hand-held (HH) otoscope (usually of the Hotchkiss variety);24% use a video-otoscope (VO) system with an otoloop attachment (although most agreed VO is not very handy for cerumenectomies);20% use a combination of HH and VO;12% use a headlamp;and only 4% (i.e., one person) reported using an operating microscope (Table 1).
Table 1. CM Survey Results
Click Here to View Larger Version of Table 1 (PDF)
Regardless of these findings, most of those surveyed believed an operating microscope would be the better and safer method to extract cerumen;however, participants cited the following reasons for not using (or even considering) an operating microscope for their practices:
- not trained in school with a microscope
- not enough space
- high cost (some thought the cost of a microscope was between $20-30k)
- CM not reimbursed through insurance;therefore, anything more than an otoscope is too expensive
- not sure if they could ever learn to use a microscope
Considerations Before Performing CM
Before purchasing otoscopic equipment, the practitioner should determine what he or she wants to achieve and how much room is needed to operate. If the goal is only a visual screening of the outer ear, using a simple otoscope and/or video-otoscope may be sufficient. However, if the goal includes CM, otomicroscopy is the preferred method as long as it is not cost prohibitive. Table 2 compares various otoscopy methods by price, illumination, magnification, ease of CM, approximate space needed to operate, and ability to document results.
Table 2. Comparison of Otoscopy Methods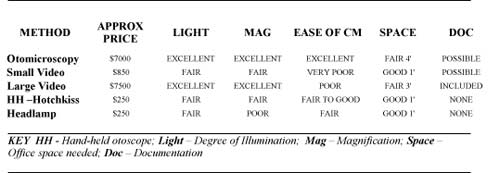
Click Here to View Larger Version of Table 2 (PDF)
As shown in Table 2, the perceived high cost of otomicroscopy would appear to be a misperception, especially when compared to the cost of the larger video-otoscope systems. While the cost of otomicroscopy and larger video-otoscope systems is about the same ($4000 - $9000), otomicroscopy is considerably more practical if one performs cerumen removal on a routine basis.
Furthermore, transitioning to the microscope is relatively easy for most practitioners already skilled at CM although basic supervised instruction and tips from experienced users are helpful. Because most audiologists are not trained to use the microscope in their university education, it is understandable that some may be intimidated to try this form of CM. However, after a few hours of supervised training and routine practice, otomicroscopy becomes more natural to the audiologist.
Once an audiologist decides that a microscope would be beneficial, it is necessary to verify that the office has the necessary space and floor plan for the device. The wall-mount Omni-10 ENT microscope from Prescott's, Inc. (Figure 4) is approximately 5' tall and 3' wide. Patients may be examined in a sitting or lying position. A helpful room design includes the patient sitting in a swivel type exam chair positioned so that the examining ear is toward the microscope as shown in Figure 4.
Figure 4. Omni-10 wall-mount ENT microscope
Patient and University (Large Group) Education
One of the outstanding features of video-otoscopy (VO) is the visual output;such documentation is valuable for patient education and/or referrals (Sullivan, 1997). Similarly, most microscopes can be interfaced with a video camera and attached to a flat screen TV or an LCD projector (Figure 5). In addition to visualizing their canal and tympanic membrane (TM), most patients find watching the actual cermenectomy procedure interesting. This visual allows an audiologist to have the patient look at the screen (see), tell them where in the ear canal they will be touched (tell), and proceed (do) (See-Tell-Do).
Figure 5. Flat screen TV display of output from the microscope.
Figure 6 shows a microscope with a small video camera mounted on the microscope. The video-cam can be attached to a DVR, S-Video, and/or simple video equipment. The video box is located on the left so the clinician can manipulate the scope and focus with his or her right hand.
Figure 6. Hitachi video camera box.
Figure 7 shows a microscope's video output attached to an LCD projector (in this case with S-Video). The individual or student sees the same image observed through the microscope. This has the potential of providing real-life, hands-on instruction when learning safe and effective CM techniques.
Figure 7.Real-time video imaging for instructional purposes.
Video-otomicroscopy also has the potential of helping university faculty more easily and effectively train students on appropriate otoscopic techniques by demonstrating them the correct procedure, watching students, correcting students, and ultimately evaluating their clinical abilities. This format is currently used in CM workshops for practicing audiologists in Colorado.
Figure 8.Classroom instruction with a video-cam on a microscope interfaced with an LCD projector.
Private and Insurance Reimbursement
Insurance coverage for ear cleanings is a topic of professional issues and is beyond the scope of this paper;however, to briefly summarize, ear cleanings are not reimbursed through Medicare or by most insurance companies. This will probably not change in the near future. That said, such a fact should not discount the value or importance of using superior equipment on patients.
As a reference, a clinic could charge a patient a fee (per ear) for CM;however, this may be waived if the amount of cerumen is minimal, the CM is conducted for a patient desiring to purchase hearing aids, or if an existing patient needs occasional CM.
Near Absence of Distributor Marketing to Audiologists
Compared to video-otoscopes, there has been little marketing of microscopes to practicing audiologists. Companies selling and servicing operating microscopes have never (to the author's knowledge) exhibited at AAA, ADA, or ASHA nor have they advertised in professional trade journals. This should change as Prescott's Microscopes* will exhibit at the 2008 convention of the Academy of Doctors of Audiology in Las Vegas and the 2009 American Academy of Audiology meeting in Dallas. This is a perfect opportunity to sit down and try a microscope. The view is extraordinarily better than traditional methods, and as marketing increases in the field of audiology, it is expected that the use of simple otoscopes and video-otoscope systems will decline in favor of superior equipment such as microscopes.
Conclusion
Otomicroscopy is not incorporated into most audiologists' offices, which is most likely due to lack of exposure to microscopy during training and internships and lack of marketing on the part of microscope companies. It is the author's opinion that if and when audiologists are given a "hands-on" demonstration with microscopy, learn of the relatively affordable price, and are given a couple of pointers on using the microscope, the operating microscope will emerge as a standard piece of equipment in audiology practices.
The Author's Personal Experience with Otomicroscopy
My "conversion" to using an otomicroscope started in 1993. I was cleaning the ears of a local opera celebrity and trying to be extra careful, in part because he was a public figure. I was using my best eye to look through my Hotchkiss otoscope (dealing with the fair illumination and magnification) and having to position the scope with my left hand so that I could remove cerumen with my right. The process was not easy, and in my opinion, the reason was due to inferior equipment. I finished the procedure without causing too much discomfort for my opera star, but I realized I needed better illumination and magnification, along with a hands-free system to more easily perform cerumen removal.
Figure 9.Eugene R. McHugh, EdD, CCC-A
As many audiologists recall in 1993, video-otoscopy (VO) was being heavily marketed to audiologists and hearing aid specialists. There were exceptional articles on its benefits (cf. Sullivan, 1993), and many colleagues had one, therefore, I requested a demonstration. It was my impression that video-otoscopy provided excellent illumination and magnification of the canal and TM along with outputting a handy color picture for documentation;however, it did not offer much help with CM. I discussed my dilemma with a local otologist who recommended I get a microscope rather than a video-otoscope. Once I was able to view an ear canal through a binocular microscope with its excellent fiber optic illumination and magnification, the decision on the most effective method for exams and CM was clear. Most of all, both hands were free to work. As it were, "I saw the light."
I have been using an operating microscope for over 15 years and believe it to be an excellent, perhaps even the best, investment I have made, especially considering the potential liability associated with CM. Our "used" wall-mounted microscope, purchased from Prescott's, Inc. was very affordable when compared to other audiologic equipment in our clinic, extremely durable, and relatively easy to use. (I recently traded in my used microscope for an upgraded model, Prescott's Omni-10, for a cost of $6800.00. I received a credit on my used system that Prescott's can service and re-sell.) It now seems inconceivable to use anything but a microscope for CM on our patients. Patients are more comfortable, my visual accuracy has significantly enhanced, and the hands free operation while cleaning ears is indispensable. Most importantly, prior to every hearing test, my patients have completely clear ears. As my competency in CM by otomicroscopy has improved over the years, I now feel comfortable with even very challenging cases that prior to using a microscope would require a referral.
References
American Speech-Language-Hearing Association (1992). External auditory canal examination and cerumen management. ASHA, 34. 22-24.
Ballachanda, B. (1995). The Human ear canal. San Diego: Singular Publishing Group.
College of Audiologists and Speech-Language Pathologists of Ontario (2005). Preferred practice guidelines for
cerumen management. Direct URL: caslpo.com/english_site/ppg_cerumenmanagement.pdf. Retrieved February 1, 2008 from the Preferred Practice Guidelines Archive at caslpo.com
Courtois, J. (1999) Earwax and foreign bodies in the ear canal. Available through Widex.
Gleitman, R.M., Ballachanda, B.B. & Goldstein, D.P. (1992). Prevalence of cerumen impaction in the general population. The Hearing Journal, 45, 28-32.
Purdy, J. (2002, September 3). Managing cerumen. AudiologyOnline, Article 365. Direct URL:
www.audiologyonline.com/articles/article_detail.asp?article_id=365. Retrieved May 15, 2008 from the Articles Archive at www.audiologyonline.com
Sullivan, R. (1993). How video otoscopy benefits hearing health care practice. Hearing Instruments, 44(4), 15-18.
Sullivan, R. (1997). Video otoscopy in audiologic practice. J. Am Academy of Audiology, 44(8), 447-47.
Biography
Eugene (Gene) R. McHugh, EdD is a private practice audiologist for 23 years in Colorado Springs, CO.
*Disclosure: Dr. McHugh is a non-paid consultant with Prescott's, Inc., a nationwide distributor of operating microscopes for many specialties located in Monument, CO with sales and service centers in 19 locations around the country.
