
Introduction
Today we'll be talking about sound and the science behind NIHL. In order to keep to the allotted timeframe, I'm going to have to oversimplify in a few areas as we cannot adequately cover a complex topic like this in just an hour. In addition to the science behind NIHL, the topics I'll discuss today include: regulatory attempts in the United States and abroad to minimize NIHL; exposures of music consumers (noise survey); the clinical evaluation of NIHL, and implications for the prevention of NIHL, including the use of hearing protection devices.
Recreational NIHL risk other than music
The National Hearing Conservation Association (NHCA) meeting was held in Portland, OR a few years ago and while we were there we had an opportunity to visit the Listen Up! exhibit at the Oregon Museum of Science and Industry (OMSI). In this exhibit, participants answer questions about their own sound exposures and then, if they consent, go through a simple threshold measurement at 4 kHz. Some very interesting information has been gained from the Listen Up! exhibit (Figure 1).
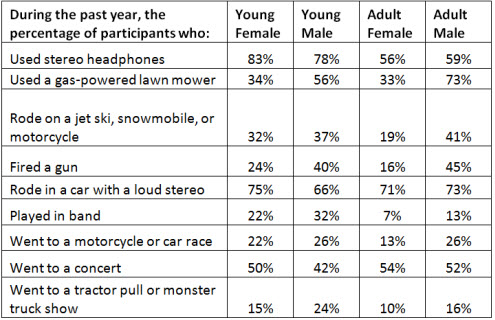
Figure 1. Data collected from the Oregon Museum of Science and Industry's Listen Up! exhibit (www.dangerousdecibels.org/research/omsi-research-data/)
As we look across different sounds to which one might be recreationally exposed, we see that a lot of people use headphones, shoot firearms, and ride in cars with loud music (Figure 1). These are potentially our patients. Out of the thousands of people who have participated in this OMSI exhibit, 22% exhibited hearing loss at 4 kHz. The percentage of children, defined as teenagers and younger, where the hearing threshold was equal to or poorer than 30 dBHL at 4 kHz was 9% of the boys (n = 6,400) and 10% of the girls (n = 9,700). In the adult population, 12% had a loss at 4 kHz. Overall, a higher percentage of male adults showed hearing loss at this frequency (16% of 8,700 men) as compared to women (9% of 12,000) or the youth group as a whole. Perhaps as men are getting older they outpace the women in terms of hearing loss, or perhaps in the younger population both are equally exposed to high level sound.
My research background is in sound exposures from music and subsequent NIHL. We know that the number-one recreational source of NIHL is a firearm. Just to orient ourselves, what levels are dangerous exactly? I want to share with you some firearm data that Michael Stewart (2008) presented in our first AudiologyOnline NIHL series. To give you an idea of the force behind any firearm, the sound exposure ranges from 140 dB up to 160 - 170 dB with a larger caliber rifle. These peak levels are capable of causing a physical acoustic trauma, which we will talk about in a moment.
WOOD Magazine (Hunter, 2008) published information related to the intensity of power tools found in a woodshop. Some tools such as a minilathe with spindle do not exceed a dangerous level, while others, such as a circular saw and chainsaw, are extremely dangerous. A person working in a small enclosed workspace should not only worry about dust particles that may damage their eyes or lungs, but obviously also about the noise exposure to their hearing as well.
Other sources of recreational NIHL include motor sporting events, jet skis, and all terrain vehicles. All of these at full throttle reach levels above 100 dB. One of my friends was at a football game in Colorado, and she measured sound levels there to be over 100 dB time-weighted average for a four-hour game. NASCAR is another popular sporting event in America, and also one of the loudest. A recent study (Rose, Ebert, Prazma, & Pillsbury, 2008) showed that the noise at a seat 150 feet from the race track over the course of four hours measured close to 101 dBA average. This is dramatic. At 20 feet from the race track in the front row, average levels were 106 dBA. You could expect that if a person did not have hearing protection at a NASCAR event, they might walk out with some permanent hearing damage.
As we are now in early July, many of us who practice audiology in Children's Hospitals are waiting to see how many kids will come in with a unilateral loss or asymmetric permanent threshold shifts, along with finger burns from holding fireworks too close to the fuse. A study from the late 1980's described sound levels from fireworks at three meters away (Gupta & Vishwakarma, 1989). Some fireworks measured 126 to 156 dB. The authors also noticed that children aged 9 to 15-years-old were more likely to have permanent hearing loss from fireworks than adults. Perhaps this is because children's ears are more sensitive or because they did not move away as quickly as the adults, or maybe a combination of the two.
Elements of a Hearing Loss Prevention Program
In bringing people back to thinking about hearing loss prevention, what kind of exposures are you going to see in the clinic? How can we prevent those exposures from being dangerous? Once it has been determined that the exposures are dangerous, what can we do to mitigate the risk or damage that could result? All of these are elements of a hearing loss prevention program, and while this is drawn very much from the occupational sector, we can certainly apply it to music exposures. Today I am going to try to give you a more broad understanding of these five tenants:
- Noise survey and assessment
- Engineering controls
- Audiometric monitoring
- Education and motivation
- Hearing protection devices
Frank Wartinger, who was an extern at Children's Hospital Boston, and I were hired to do some noise surveys for the Bamboozle Road Show last summer during a four-and-a-half hour concert featuring Boys Like Girls and All Time Low at the Comcast Center in Mansfield, Massachusetts. Frank and I did some sound surveys to see what kind of risk might the audience have, but the study was primarily for musicians to give them an idea what kind of hearing protection devices they might need. We stood at front of house at the audio engineer's mixing board, which is directly in front of the stage, set back at the edge of the audience area.
All Time Low used a sound level meter, the kind you would purchase at Radio Shack, and placed it at front of house on the mixing board to get an idea of what kinds of sound levels were reaching the audience. It measured 104 dBA on slow integration. What does that mean? Well, we found that the overall equivalent continuous levels, basically how loud the concert was, for somebody who had attended the show from start to finish was 105 dB. If we consider that an 85 dBA time weighted average for an 8 hour continuous level with a 3 decibel exchange rate as our maximum allowable exposure, an audience member at this concert would sustain a 5000% noise dose (Fligor & Wartinger, 2011). This is about 50 times what you would be allowed to be exposed to before we would suspect damage. For someone working in the crew backstage or on the perimeter of the grounds, the levels are lower at 2198% noise dose. The equivalent continuous level is 99 dB for these individuals. But between setup and sound checks the crew's exposure time was 7 hours. So while the levels are a lot less, the overall total exposure for the crew ended up being about 22 times their allowable amount. Although they may not be getting such a marked overdose as that of an audience member, consider that the crew and the band do this about 200 times a year, as opposed to the maybe four or five times a year of a concert patron.
What are the mechanisms of NIHL? Generally, we think of NIHL coming from two different aspects: gradually developing noise-induced permanent threshold shift or one-time acoustic trauma. A permanent threshold shift (PTS) arises from exposures of about 78 dB, which is the lowest intensity level known to cause hearing shifts in a very fragile population, to upwards of 130 dB or more. This range depends entirely on the "toughness" of the ear. Somewhere in this range the ears are metabolically overloaded, with the primary site of lesion being the outer hair cells. There is some swelling within the spiral ganglia and some changes that occur in the stria vascularis. This results in a gradual loss in sensory hearing and is also often marked by a noise-induced temporary threshold shift. We have all had this experience: You go to the concert, you get that 5000% noise dose, your ears are overloaded and you cannot hear quite as well for a day or two. As audiologists, we know that this is a temporary threshold shift (TTS), and if you give your ears between a few hours and two days, your ears should recover back to baseline. But if you do this often enough, you are going to have some PTS instead of just a TTS. Over time, thresholds do not come all the way back to baseline.
This situation can be contrasted with acoustic trauma. Acoustic trauma, generally speaking, can occur after a blast of 140 dB peak-SPL or greater. Dick Price, back in 1981, showed that in highly susceptible individuals that level is as low as about 132 dB (Price, 1981). The impulse of noises that have a very brief, fast rise time often result in mechanical damage. After a single exposure to that kind of a blast, the sound wave shears off the basilar membrane and leads to sensory hearing loss. Acoustic trauma can result from this brief, marked overdose. You can incur mechanical damage as well as some metabolic damage when you get these one-time overdoses.
Injury from Chronic Noise Exposure
We know that injury from chronic noise exposure is a function of time as well as intensity, and it is frequency dependent. This is why sound levels in decibels are described in terms of an A-weighting filter. A-weighting approximates the function of the middle ear at moderate sound intensities. We know that at higher sound levels the middle ear transfer function flattens out and becomes C weighting, but all the sound surveys that were done that tell us how loud is too loud before you sustain injury were all collected in dBA. For those of us who do a lot of testing, the noise-induced PTS is what we think of as a noise notch on the audiogram. A noise notch typically occurs between 4000 and 6000 Hz, where the thresholds are the poorest. An average adult man will have the poorest thresholds around 4000 Hz after noise-induced hearing loss.
Other injuries from chronic noise exposure that are very important for us to consider include tinnitus, or a constant ringing, buzzing, hissing, or phantom noise in the ear. Individuals may also suffer abnormal pitch perception and loudness tolerance problems.
We may have learned back from our noise courses in college that 90 dB for an 8 hour time weighted average with a 5 decibel exchange rate was considered an acceptable exposure level. Well, it turns out that is actually not an acceptable level. OSHA in 1981 reported on data from three different organizations that described how many people had hearing loss as a result of sound exposure. The organizations (ISO, EPA, and NIOSH) looked at groups exposed to 80 dB for an 8-hour time-weighted average over their working lifetime. Zero to five percent of the people exposed to 80 dB sounds had what would be considered a "material hearing impairment." A material hearing impairment was defined as greater than a 25 dBHL loss determined by averaging the thresholds at 1000, 2000, 3000, and 4000 Hz (NIOSH, 1998). Bear in mind that you are going to have a lot of loss at 4000 Hz before you have loss at 1000 Hz when it comes to noise exposure. People exposed to 85 dB for an 8 hour time weighted average over their working lifetime had between a 10 and 15% risk of having a material hearing impairment. People exposed to 90 dB for an 8 hour time weighted average over their working lifetime would have a 21 to 29% risk of a material hearing impairment. A re-analysis of the original data was conducted by Prince and colleagues in 1997, and they reported that roughly 8% of people who were at risk for material hearing impairment are exposed to 85 dBA for 8 hour time weighted average. The point is that even at 80 dB, if exposure time is long enough, some people are going to sustain a material hearing impairment.
Music-Induced Hearing Loss
Before we dive into this subject, I wanted to mention a couple of books and chapters that are good resources on music-induced hearing loss. Hearing Loss in Musicians: Prevention and Management by Marshall Chasin (2009) is a thorough textbook on the subject. He also wrote the Consumer Handbook on Hearing Loss and Noise (Chasin, 2010) which is geared towards the avid interested consumer and is written in good layman's terms.
To put it simply, many people use headphones. This has been a topic in the popular media for at least the last seven years. I collected data for my dissertation under Clark Cox on the outputs of various headphones at different volume settings of a CD player and published those findings in 2004 (Fligor & Cox, 2004). I want to point out that all the headphones we examined are capable of putting out sound levels over 85 or 90 dB, but there is a lot of variation from one manufacturer to the next. This does not mean people automatically use their headphones too loudly, but if a person chose to use their headphones at a high level, how long could they listen safely? This exact question came from a young man when I was a student clinician, and, as it turned out, there was no good answer for him at that time.
In order to obtain those kinds of measures we have to get a good understanding of how to measure something that is in your ear. This does not mean taking a sound level meter and holding it up to the headphone as that does not tell you what you need to know.
Hearing aids are meant to be measured in a coupler, and therefore you have to measure them in the real ear using a probe microphone or in a 2-cc coupler. Headphones technically are also used in a coupler, which is, of course, your ear.
If you consider the transfer function of the open ear, you'll see that the gain at the eardrum in some people is above 15 dB between 2000 and 4000 Hz. When we measure risk, we actually do this outside of the ear, not at the eardrum. The original data that told us "how loud is too loud" were recordings made with dosimeters placed near a person's shoulder. But when we are using headphones or measuring a sound in the near field, you cannot merely hold a sound-level meter up to the outside of a person's head. The hazard has to be measured down near the eardrum to get an accurate measure. The difference between the level at those two locations - the eardrum and outside the head - is the transfer function of the open ear. Essentially what we have to do is equate the level that we measure down at the eardrum to what it would be if we were able to measure it outside the head.
We used measurements such as there in a recent study, where we wanted to describe "how loud is too loud" for a person that wants to enjoy using headphones at a loud level, and limit their listening time in order to reduce their risk of NIHL. In this study, we offered an 80 90 rule, meaning a person could listen at about 80% of the maximum volume for 90 minutes a day without significantly increasing the risk for a NIHL (Portnuff, Fligor, & Arehart, in press). This basically estimates a 50% noise dose, i.e. if a person were to listen at approximately 80% of their maximum volume, their free-field equivalent continuous level would be 89 dBA.
Terry Ives and I did another study (Fligor & Ives, in review) out of Salus University where we looked at 100 subjects using four different earphones in four different listening environments. We used one over-the-ear style and three different earbud-style headphones, which typically do not block out much background noise. We wanted to see how people would use their headphones knowing that some headphones put out more sound than others.
It turns out people do use these headphones very differently. We varied the amount of background noise in their environment. We included everything from pink noise to restaurant noise to airplane cabin noise. For your information, noise levels on an airplane are about 80 dB. We found that the more sound isolation you give somebody in the ear, the less ambient noise makes its way in the ear canal and the lower people would tend to listen.
We found that for every decibel of background noise that makes its way into the ear canal, people choose to listen at about another three tenths of a decibel higher. Up at the higher-intensity background noise levels, people are listening well above 80 dB and some of them are therefore putting themselves at a potentially serious risk of NIHL.
The simple recommendation to someone wanting to protect themselves against NIHL from using headphones too high is to give them the sound-isolating earphones. This implementation in the study literally changed listening behavior rather significantly, and had an effective full one third of influence on their listening behaviors.
So how do people really use their headphones? Some colleagues and I published a paper (Levey, Levey, & Fligor, 2011) on listening levels of college students in New York City. We chose New York City because the subway tends to be really loud, as are subways in a lot of cities. Dr. Robyn Gershon and her colleagues (2006) documented that the overall equivalent continuous sound exposures might, in fact, put some people at risk for NIHL from riding the subway alone. Consider that some people use headphones while riding the subway, too. If the average ambient noise on a subway is between 83 and 106 dBA (Gershon, Neitzel, Barrera, & Akram, 2006) , and we know some people crank up the headphones when the background noise goes up, how loud are people actually listening when riding the subway?
We caught people as they exited the subway station platform to measure their headphone levels. The average free-field equivalent continuous levels for women and for men were 92.4 dBA and 92.7dBA, respectively, with no difference between the two genders. These are fairly high levels. Contrast that with a study in Australia (Williams, 2005) where their chosen listening level was 86.1 dBA. Our New York City listeners were about 6dB higher.
When we average a single listening session, or basically what we would call an 8 hour equivalent continuous level, an estimated weekly equivalent continuous level for the New Yorker's sound exposures were 87.2 and 87.4 dBA, respectively (Levey, Levey, & Fligor, 2011). What that tells us is that the average person, out of our 189 subjects in New York City, was overexposed. We recommend an exposure level of no higher than 85 dBA, and there were quite a few people above that level. Fifty percent of our participants were at 87 dBA and above. That is a bit concerning to us. High background-noise levels mean that some people are turning the volume up and listening for durations long enough to put them at risk.
It has often been reported in the literature that women do not listen at levels as high as men. Well, this notion did not reach significance in our study. The men, anecdotally, may listen ever-so-slightly higher than women, but this did not reach any level of significance in our study, which means that men and women are equally at risk, just from headphones alone.
Audiometric Monitoring
Periodic audiometric monitoring is important for anyone routinely exposed to noise, simply because the ear is a sensitive indicator of its own damage. An initial evaluation at the Musician's Hearing Program at Children's Hospital Boston encompasses a series of testing to inform us where an individual is at baseline and then annually from that point forward. We perform comprehensive audiometry using air, bone and speech measures. Just because the patients are musicians or audio engineers or some other sound-exposed person does not mean they could not have a tumor or otosclerosis or something else that needs medical management. Conducting immittance and acoustic reflex testing if indicated may also be included in the overall test battery. We include distortion-product otoacoustic emissions. I incorporate a very wide range, from 1500 Hz to 10,000 Hz, sampling close to four frequencies per octave. It is very helpful in describing how much damage we might be able to detect.
If a person reports at the initial appointment that they have tinnitus in their ears, we ask them to fill out a Tinnitus Reaction Questionnaire or the TRQ (Wilson, Henry, & Bowen, 1991), which happens to be my favorite survey for tinnitus assessment. You can also use the Tinnitus Handicap Inventory (THI; Newman, Jacobson, & Spitzer, 1996). If you have a total score of 17 or higher on the TRQ, it is considered clinically significant (Wilson et al., 1991). Certainly, in my experience, that equates pretty well with people who are slightly bothered by the tinnitus and people who are really suffering.
Figure 3 is an audiogram of a patient who came through our clinic. This was a 39 year old male who was suffering from tinnitus. His TRQ score was about 45. You see across the range of all the inter-octave frequencies he has normal hearing sensitivity (Figure 2). He does have a 20 dB notch at 6 kHz in one ear, but it is really not significant overall and his hearing would be considered in the normal range.
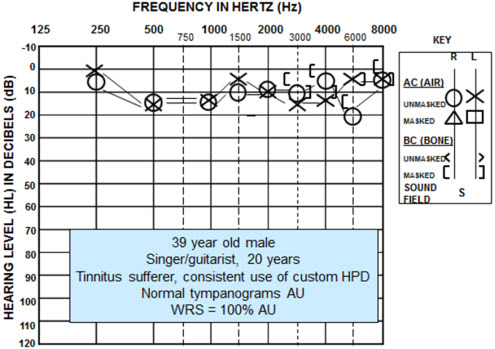
Figure 2. Audiometric data of male tinnitus patient.
His distortion-product otoacoustic emissions are shown in Figure 3, and you can see at roughly an F2 of 6000 Hz to 10,0000 Hz he has absent emissions. We see slight reductions in the strength of the emissions at 2000 Hz also, but considering his pure-tone thresholds, we may not have expected to see such a drop in the emissions at the higher frequencies. After being presented his results, and learning that there was indeed an underlying biological cause to his tinnitus and in fact he did have some damage to his ear, his TRQ dropped 50%. His score then was still in the low 20s, which is still clinically significant for tinnitus impacting daily life, but it gave him much relief to know that there was a reason for his tinnitus and he was not making it up.
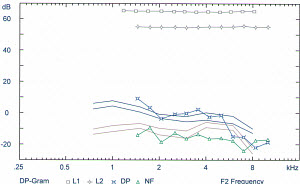
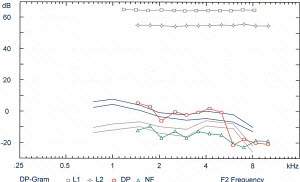
Figure 3. Distortion-product otoacoustic emission results from a male patient suffering from tinnitus. Audiogram shown in Figure 4.
Hearing Protection Devices
Consider that when a person uses hearing protection devices it means that other aspects of a hearing loss prevention program have, in fact, failed to protect the person. It means we are giving up on being able to prevent them from being exposed to hazardous sounds in the first place, and now we are putting our trust in something placed in their ear to protect them instead. Education and motivation are the most significant predictors for a person preventing a NIHL. They are also the most difficult to put into place, especially when you consider the audience we are recommending this to. These are people that come in year after year at their jobs, push a button when they hear the beep, and then listen to a lecture on how to roll, pull, and insert that foam ear plug. For people on the recreational side, if they make their way in to see you it often means that they are highly motivated. But then you have the flip side where the people are very fatalistic and say, "You know what, this is part of rock and roll. We are going to have some hearing loss. It is just what is going to happen." Bearing that in mind, some people do need to use hearing protection devices because they are going to be exposed to high levels of sound.
Why might a person want to use "flat frequency attenuators" or "musicians' ear plugs" as they have been termed? The answer is simply because sticking a foam plug in your ear or putting an earmuff over your ear changes the quality of sound, on top of not looking cool to some people. The change in the quality of sound is rather dramatic. When you change the fundamental frequency and the harmonics of a given musical note, it alters the perception of the sound. If you play an A above middle C on a piano, the fundamental frequency is 440 Hz. But the harmonics above that are at integrals of 440 Hz: 880 Hz, 1320 Hz, 1760 Hz, and 2200 Hz. A violin sounds like a violin because of its harmonic structure. That describes its timbre.
Figure 3 is a real-ear measure of an 85 dB swept tone down near my eardrum with and without a foam earplug. What we see with the green line is a transfer function of the open ear. When I insert a foam plug in my ear, we obliterate that open-ear response and lose the natural ear canal resonance, which can be seen in the pink line of Figure 4. There is not much attenuation at the low frequencies but a lot at in the highs. I can tell you that someone who really wants to listen to music is going to reject use of that foam plug because of the high-frequency attenuation to the music.
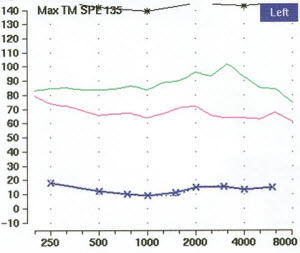
Figure 4. Real-ear transfer function of the open ear (green line) and ear occluded with a foam earplug (pink line).
Etymotic Research developed filtered earplugs in levels of 15 and 25 dB sound attenuation (ER15 and ER25). These earplugs help to preserve the relative harmonic structure of the music. For those of you who work with musicians and these particular earplugs, I implore you do an 85 dB swept tone with the earplug in the coupler of your hearing aid verification equipment (Figure 5). We know real-ear measures significantly improve patient satisfaction when they are used with hearing aids. I would say that the same is true when a person is using musicians' ear plugs. If you fit a person with a musicians' ear plug that does not perform well, they may reject them, and then you are putting their hearing at further risk because now they are going to reject future hearing protection, even flat-frequency attenuators as well. They are musicians. They know if the sound is flat and can hear that difference if it is not.
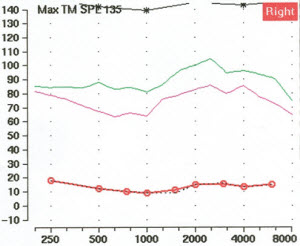
Figure 5. Transfer function of the open ear (green line) contrasted with the same input through an Etymotic Research ER15 filtered earplug (pink line), which maintains the high-frequency characteristics of the music.
Hypothetically, what would happen at the Bamboozle concert with our audience member if we applied ear plugs? Remember that the audience was exposed to 105 dB for 4 hours when they attended that concert, so their unprotected noise dose was 5000%. Let's say they were wearing an ER15 earplug; their noise dose drops all the way down to 158% (Fligor & Wartinger, 2011). Now, that is not less than 100% but a person can be slightly overexposed on limited occasions. It is not that significant in terms of adding to the wear and tear over their lifetime. You could be extremely conservative and fit them with a higher level musician's ear plug, an ER25, and drop them down to a 16% dose, but that may be going a little overboard as when a person goes to a show they expect it to be loud. If an audience member listens at 105 dB minus 15 dB when wearing the ER15 plugs, they will be listening at 90 dB, and 90 dB is still loud. Their calculated exposure is 158% considering they did not take any listening breaks. If they go to the bathroom or concession stand and get a break from the music their dose is going to be less than that.
What about for the crew member or the band member? Their unprotected noise dose was about 2200%, and that is significant given that they are going to be hit with that about 200 times a year. The ER15 earplug puts them at 70% sound exposure (Fligor & Wartinger, 2011), so I would suggest that an ER15 would be appropriate. You could fit them with ER25, but again, they really want to be able to listen to the sound especially if this is an engineer. Do foam plugs protect? Absolutely they do. But a foam plug may not be the best approach to use for these people.
What other things can be done to limit the noise exposure? We can look at our engineering controls. One thing that can be done is to use in-ear monitors, which are just like any other headphone for the most part. The idea is to take the sound from the stage and play it back directly into the artist's ear, instead of it being broadcast back through some on-stage loud speakers. The main loud speakers that project the sound to the audience are not effective in getting the sound back to the musician without a time delay after bouncing off the back of the venue. This alters the singer's timing; they have to be able to hear themselves well on stage.
If you fit the musician with an in-ear monitor, they are going to be able to hear themselves pretty well no matter where they are. They can walk around. They can interact with the audience in one direction or another. And given that you do not have the wedge monitor on stage, you give them really good sound isolation. Remember that Fligor and Ives (in review) showed when you provide sound isolation, the individual is going to listen at lower levels. You can use a universal fit or a full custom sleeve, similar to an earmold. These provide really good sound isolation and really good sound quality for musicians.
In-ear monitors can also be made with an ambient microphone, so while their ear has good sound isolation, they can still hear what is happening around them. These microphones are very high quality and do not saturate even up about 140 dB. The reason they do not saturate is that there is a 9 volt battery in the exterior pack powering it. There is a potentiometer that allows you to dial down the ambient sound from the audience in 4 dB steps. What is presented to the person's ear is a mix of ambient sound and their own voice or instrumentals. It is whatever the musician wants to hear. They offer binaural hearing with good sound isolation and voice quality.
I am sure plenty of you have seen a performer on TV with one ear monitor out and the other ear monitor in. With only one monitor in, they are losing their binaural summation of loudness, and they are going to be tempted to turn the level up to achieve their perceived loudness. You are increasing the loudness that the person is getting in the ear with the monitor. The other ear without the monitor is getting exposed to the audience levels, again, around 105 dB, which is a significant exposure when the person is playing longer than 15 to 30 minutes. Allowing the musician to mix in some of the ambient sound allows them to keep both in-ear monitors properly seated and the monitoring at a level that is comfortably low. I counsel my musician patients to listen at the lowest level at which they are comfortable. That typically gives people a little incentive to not overexpose their ears because these can be very powerful receivers. You can crank these things way up. They are not a hearing protection device. You can damage your hearing very easily with in-ear monitors, so there is a need to counsel a person on how to use them correctly and conservatively.
Certainly the practice of hearing healthcare is a business, as all healthcare is a business. I think it is really important for us to focus our efforts on a holistic perspective. We are looking at noise survey through hearing protection devices and should not be bundling all of our services into the hearing protection device itself. Certainly not every payor is going to reimburse you for this, but I have been reimbursed for CPT code 92596 (Ear Protector Evaluation) when we are able to bill an individual for services. We are selling a service as opposed to selling a device. That is my little soap box to unbundle where you can. I have found this to be very successful within my own practice, and I would applaud others who are looking to do that. These are patients who are looking to be cared for and not consumers to be sold to.
Management of Noise-Induced Hearing Disorders
Noise exposure can leave an individual with more than just a hearing loss, so I call it a hearing disorder. They may also experience tinnitus, abnormal loudness perception or hyperacusis, and abnormal pitch perception, or diplacusis. The important thing is if you are not used to working in this area, do not just dabble in it; but on the flip side do not limit your services, either. If a musician is searching you out and says, "I have ringing in my ear. It is driving me crazy, and I think I have to quit playing." Get a mentor. Find somebody to help you to work with this person because they are looking for help. The tinnitus patients, in particular, are really in need of some help. I have a fair number of musicians in their 30s to 40s and then certainly in their 50s who are using hearing aids, and use of hearing aids really does improve sound enhancement. There is general background sound there to help take the person's perspective away from the constant ringing. Hearing aids can certainly reduce stress if they are having difficulty with communication as well.
Communication impairment from the hearing loss increases their stress level, which exacerbates their tinnitus. Understand, however, that when a hearing aid is set to maximize speech understanding it is very likely not going to be an appropriate setting for music because speech and music are very, very different inputs. If you are doing some work in this area or want to look into it, the audio engineers are your best friends. These are the people that know things like Fletcher curves, and they understand loudness but do not necessarily understand things like intensity over time and how that damages the ear. They are very technologically savvy, and they will be your ally in working with musicians and crew. They are the ones that are going to tell the musician to shut up and use the device.
We often think about the fact that tinnitus cannot be cured. The issue here is that this mindset focuses on your perception of the tinnitus, and it becomes very difficult to habituate to the perception. The focus should be put more on habituating to the reaction to the tinnitus. In my experience, I have found that once the person habituates their reaction to the tinnitus their perception often times does follow, and their suffering decreases.
Summary
Understand that music exposure is not always recreational, but it is certainly unregulated. These exposures are significant for placing people at risk for music-induced hearing disorders. We have excellent tools for assessing it as I have discussed today. Remember that fitting people with in-ear devices helps to fulfill the goals of a hearing loss prevention program, but it is not the fix. The fix is you, the audiologist, and your expertise and care in working with these patients.
Question & Answer
Can we recommend any kind of special hearing aids in the case of NIHL?
Well, it depends on what the purpose is. If it is for general communication, I am a little bit
partial to the receiver-in-the-canal open fittings. If you want to use an earmold, make as large of a sound bore as you can just for general communication. These are people who typically have really good hearing in the low to mid frequencies and then have a lot of hearing loss slipping off 3 kHz and above. An open fit really is better in those instances.
Once people are on stage you really could use the hearing aid if it is set appropriately. You could use the hearing aid as an ear monitor if you have it hooked up with an FM system, and in that instance you would need to have a fully occluded full-shell mold with no vent. Certainly do not hesitate to use combination devices - hearing aids with a combined tinnitus masker if appropriate. Some people have done very well with that.
What is damage criteria?
The damage risk criteria is a way of describing how many people would be at risk for sustaining a material hearing impairment given a certain sound exposure. It is not how loud something is, but how loud and how long you are exposed. Understanding that you are not going to protect everybody unless you keep the levels so low that nobody is going to be overexposed, and some people are really going to want it louder. The level I prefer when I set my iPod® volume is 89 dB. Well, 89 dB is safe for roughly about three hours. So if I go more than three hours, I've passed my permissible exposure level. Feel free to e mail me and I will give you a little more information about that if you need.
What specific services are you including under the 92956 CPT code? Are you submitting this in addition to the basic audiology codes?
Yes, I am. To summarize, because I do not have the CPT manual in front of me, Ear Protector Evaluation basically says that you are able to measure unprotected exposure and protected exposure and you show a difference in the sound level that would reach the eardrum. You can do that a few different ways. You can do a measure called real-ear attenuated threshold, which is where you perform standard pure-tone audiometry in soundfield without an ear plug in and then again with the plug in. You can imagine that takes a little while. What I showed with the real-ear probe microphone (Figure 8), is that you can get each ear individually and demonstrate that you have got some sound isolation and where the attenuation occurs. That is in addition to the 92557 immittance codes.
Just to clarify, if I am running a musician's plug using real-ear equipment, the 85 dB swept tone should reveal a transfer function similar to that of the open ear, just attenuated. Is that correct?
Yes, that is correct. Refer back to Figure 5 where you can see the green line as an unprotected run, and then the pink line with a well-fitted musician's ear plug. You see the little notch up around 3200Hz is very similar between the two runs. Bear in mind you have a probe microphone in place, which can cause a small slit leak in your run. This is an artificial attenuation of the low frequencies. One thing you can do to help mitigate that is to put a drop of otoease on the probe so there is more of a seal between the ear plug and the opening of the ear canal.
Have you had much experience with musicians being dissatisfied with the musicians' plugs?
Yes, but not overwhelmingly. I do not know how much is "much." I do not have a lot of people say, "I don't like how it sounds." First off, this could partly be because I counsel them that it has to be quieter, and because of the real-ear measure I know it is performing very similar to how the open ear performs. It is very rare, but on occasion I do get a plug back from the lab that doesn't fit or measure correctly. I take a new earmold impression and send it back to the lab and ask them to remake it. That has helped me to reduce the dissatisfaction.
References
Chasin, M. (2009). Hearing loss in musicians: Prevention and management. Sedona: Auricle Ink Publishers.
Chasin, M. (2010). Consumer handbook on hearing loss and noise. Sedona: Auricle Ink Publishers.
Fligor, B.J., & Cox, L.C. (2004). Output levels of commercially available portable compact disc players and the potential risk to hearing. Ear and Hearing, 25(6), 513-527.
Fligor, B.J.,& Wartinger, F. (2011). Musicians' hearing program. Audiology Today, 23(3), 30-40.
Fligor, B.J. & Ives, T. (in review, 2011). Does headphone type affect risk for noise induced hearing loss?
Gershon, R.R.M,, Neitzel, R., Barrera, M,, & Akram, M. (2006). Pilot survey of subway and bus stop noise levels. Journal of Urban Health, 83(5), 802-812.
Gupta, D., & Vishwakarma, S.K. (1989). Toy weapons and firecrackers: a source of hearing loss. Laryngoscope, 99, 330-334.
Hunter, B. (2008). Understanding shop noise! WOOD Magazine, 184, 86.
Levey, S., Levey, T., & Fligor, B.J. (2011). Noise exposure estimates of urban MP3 player users. Journal of Speech, Language, and Hearing Research, 54, 263-277.
Newman, C.W., Jacobson, G.P., & Spitzer, J.B. (1996). Development of the tinnitus handicap inventory. Archives of Otolaryngology Head & Neck Surgery, 122(2), 143-148.
NIOSH. (1988). A proposed national strategy for the prevention of noise-induced hearing loss. Chapter 8 in Proposed National strategies for the Prevention of Leading Work-Related Diseases and Injuries, Part 2. National Institute for Occupational Safety and Health: Cincinnati, OH.
OSHA. (1981). Occupational Safety and Health Administration, Occupational noise exposure: Hearing conservation amendment. 46 Fed. Reg. 4078-4179.
Portnuff, C.D.F., Fligor, B.J. & Arehart, K.H. (in press). Teenage use of portable listening devices: A hazard to hearing? Journal of the American Academy of Audiology.
Price, G. R. (1981). Implications of a critical level in the ear for the assessment of noise hazard at high intensities. Journal of the Acoustical Society of America, 69, 171-177.
Prince, M.M., Stayner, L.T., Smith, R.J., & Gilbert, S.J. (1997). A re-examination of risk estimates from the NIOSH occupational noise and hearing survey (ONHS). Journal of the Acoustical Society of America, 101(2), 950-963.
Stewart, M. (2008, July 22). Recreational firearm noise exposure. AudiologyOnline, Recorded course 11552. Retrieved August 15, 2011, from the e-learning section on www.audiologyonline.com
Rose, A.S., Ebert Jr., C.S., Prazma, J., & Pillsbury III, H.C. (2008). Noise exposure levels in stock car auto racing. Ear, Nose, & Throat Journal, 87(12), 689-692.
Williams, W. (2005). Noise levels from personal stereo use. International Journal of Audiology, 44, 231-236.
Wilson, P.H., Henry, J., & Bowen, M. (2006). Tinnitus reaction questionnaire: psychometric properties of a measure of distress associated with tinnitus. Journal of Speech and Hearing Research, 34, 197-201.

