In this talk I will review some of the research that Dr. Denis Byrne performed and some that he initiated before his untimely death in April 2000. I will be focusing on the prescription of hearing aids, because that is where Denis most advanced the science of audiology. Indeed much of the current unquestioning acceptance of hearing prescription, as well as some of the specific procedures used, originated from the research of Denis Byrne. I would like to begin by briefly setting the context in which Denis worked.
Historical context:
Denis worked as a clinician and then as a researcher in a government-funded national rehabilitation organization, called at various times the ''Commonwealth Acoustic Laboratories,'' the ''National Acoustic Laboratories,'' and ''Australian Hearing.''
The organization has always had the day-to-day delivery of services as its primary reason for existence, so the research (which has been present since the organization's inception in 1947) has always had an applied nature. The organization initially served veterans returning from WWII, but the services were progressively widened to include all hearing-impaired children in Australia (following a Rubella epidemic) and aged pensioners (retirees). Procedures produced from the research have been designed to increase the effectiveness of clinical services delivered to these patients and to be capable of application in busy clinics operating under tight time constraints.
Denis joined the organization as a clinician in 1957 and moved to the research group a few years later. He was charged with devising a more systematic method of matching hearing aids to patients, a task he fulfilled in such a manner that the method he devised became the most used hearing aid prescription procedure around the world.
Philosophical approach to prescription:
Denis described prescription or selection as a process of matching selected characteristics of the patients to selected characteristics of the hearing aid. The immediate outcome of prescription is the specification of the desired electroacoustic performance, which in turn, enables a particular hearing aid to be selected and its controls adjusted. At the time Denis commenced his research, the dominant method of selecting and adjusting hearing aids was a reduced version of the evaluative method devised by Carhart (Carhart, 1946). In the evaluative method, the emphasis was on measuring the performance of the patient with each of several hearing aids; the aid that gave the best performance was then selected. Denis pointed out that unless the aids to be compared were chosen totally at random, the evaluative approach already involved an ''unwritten'' prescription method on which the preselection was based.
Although the differences between prescriptive and evaluative approaches are usually thought of in the context of the last 50 years, both approaches have their origins in the 19th century. One brand of dome trumpets were sold in three sizes from 2.75 inches to 3.75 inches in diameter, with advertisements recommending the larger sizes of trumpets for the greater degrees of deafness. This was amplification prescription in its infancy! Alternatively, a different brand of dome trumpet was sold with several interchangeable filters that could be inserted into the open face of the trumpet. The hearing impaired wearer was expected to try each filter and use the one that produced the most intelligible or highest quality speech. This was the start of selection by evaluation!
From time to time, Denis encountered critics of his work who claimed they selected and adjusted hearing aids using their considerable ''clinical experience''. Furthermore, they claimed, such methods were more effective than anything based on a formula could ever be, as they took many more aspects of the patient into account than did any prescriptive approach. While Denis readily agreed that there was more to a patient than an audiogram, he was scathing of ''experience'' as a scientific approach to audiology. His attitude can be summarized in the following three paraphrases:
- ''If you can't write down the rules you use, you probably don't understand what you do.''
- ''If it's not written down, no one else can do it, and no one can test whether it's better or worse than some alternative approach.''
- ''If you can't evaluate your procedure you can't improve it.''
Evaluating a procedure so that it could be improved was fundamental to Denis' approach and was the major way in which his research stood out from that of others. Denis was rarely content that any problem was fully understood, but always insisted that the best understanding be made available in a practical way to support the work of clinicians.
Gain prescription for linear hearing aids - mild to moderate losses:
In this day of non-linear amplification, it may seem outdated to spend any time talking about prescription for linear hearing aids. It's not! Virtually all the research into linear amplification has been performed for typical input levels amplified to a comfortable listening level. Similar considerations apply whether such amplification has been achieved with a linear or non-linear hearing aid. (Naturally, the research into linear amplification cannot tell us much about amplification targets for low and high-level speech, but we will return to this topic later.)
Denis Byrne's first prescription procedure had the unqualified aim of maximizing speech intelligibility. The strategy employed to achieve this goal was to amplify speech so all frequency bands had equal loudness. The thought behind this strategy was that if one band of speech dominated the others in loudness, the wearer would turn down the volume control to achieve a satisfactory overall loudness. Consequently, audibility of all other bands would be adversely affected. If, by contrast, all bands are equal in loudness, then all bands can contribute to audibility.
To convert this strategy into a specific formula, several sets of data were needed. The first related average gain to average hearing loss. While compiling data on the gain used by several thousand patients, Denis confirmed the half-gain rule first formulated 30 years earlier by Sam Lybarger, although Denis' comprehensive data led to the estimate that used-gain increased by 0.46 dB (rather than 0.5 dB) for every dB of hearing loss. Second, Denis incorporated measurements of the speech spectrum, which show that low-frequency components of speech are considerably higher in amplitude than mid- and high-frequency components. Finally, Denis assumed that if he used the published equal loudness contours for pure tones, he could readily calculate how much speech should be amplified at each frequency.
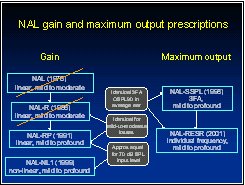
The specific goal was to raise each critical band of speech to the same loudness as all the other bands, while still achieving the average gain required by the half (actually 0.46) gain rule. The resulting formula was published by Byrne and Tonisson in 1976 and became known as the NAL prescription rule.
To make life easy for the clinician (remember, there were no computers then to make life ''easy'') the formula was turned into a slide rule. From the earliest days, Denis emphasized that it was ''real-ear'' gain that counted, not the gain achieved in any coupler. In those days, real-ear gain referred to functional gain (defined as unaided sound field threshold minus aided sound field threshold). Consequently, the front of the slide rule showed the required real-ear gain, while the back showed the coupler gain that, on average, would achieve this real-ear gain when fit with a standard earmold. NAL has kept this early emphasis on real-ear gain. As soon as probe-tube measurement equipment became commercially available, we showed that insertion gain was equivalent to functional gain (except when functional gain was wrong!) and incorporated probe-tube measurements into all hearing aid fittings (Dillon & Murray, 1987).
Denis turned his attention to another topic (binaural hearing aids) for a few years and so did not immediately evaluate the effectiveness of the NAL rule - but the organization did. Over a three-year period following its introduction nationwide, battery consumption per hearing aid increased by 50% without there being any change in the models of hearing aids being issued.
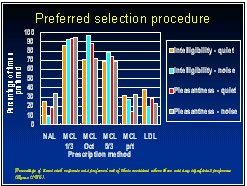
Several years later, Denis commenced his own systematic evaluation of the effectiveness of the NAL formula. He evaluated it by comparing it to several other potential prescription rules:
- Amplification of speech bands to the most comfortable level (MCL) measured using 1/3 octave bands of speech.
- Amplification of speech bands to the MCL measured using octave bands of speech.
- Amplification of speech bands to the MCL measured using bands of speech 5/3 octaves in width.
- Amplification of speech bands to the MCL measured using pure tones.
- Amplification of the speech peaks to parallel the loudness discomfort contour.
Every subject compared each response to each other response in a paired comparison task. The criteria used were both intelligibility and pleasantness and these were evaluated in both noise and in quiet. Objective measures of speech intelligibility using nonsense syllables were also gathered for each response, but these proved to be less discriminating than the paired comparison data.
The clear winners were the three responses that amplified speech to the MCLs measured using bands of speech. There were no significant differences between these three, though the response obtained with 1/3 octave bands was most often preferred. The experimental results thus validated the original aim (amplifying speech bands to achieve equal loudness) but invalidated the formula that was supposed to achieve this result.
Because the clinical population served by NAL included many young children, and many elderly clients, a prescription method that did not require measurement of MCL was desired and needed. To achieve this, Denis plotted the slope of the winning frequency response for each subject against the slope of his or her audiogram over the same frequency range. Denis also gathered data from several other experimenters who had empirically determined the best response shape for individual subjects. The various sources of data produced a consistent result: The ideal response slope varied across subjects by 0.25 to 0.35 times the audiogram slope. On average, the value was 0.31, so this number became an essential ingredient of the revised prescription rule, which became known as NAL-R. We expressed the result as a formula that simultaneously achieved the 0.46 rule for average gain, but the 0.31 rule for gain-frequency response slope (Byrne & Dillon, 1986).
One consequence of the formula was that the gain at each frequency now depended on the hearing loss at multiple frequencies, a characteristic that survives to the most recent NAL formulae and which contrasts to most other prescription rules. The NAL-R formula was also produced as a (slightly more complex) slide rule. Actually three slide rules (one each for body, BTE and ITE hearing aids) were produced; all had the same real ear gain prescriptions on the front but had different coupler prescriptions on the back.
Most people would stop, having revised the formula. Not Denis Byrne - he considered that because the formula had been changed, the new formula would also have to be evaluated.
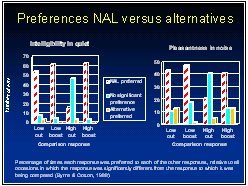
He did so by comparing the NAL-R response to responses that differed systematically from it (Byrne & Cotton, 1988). These alternatives included a bass cut, a bass boost, a treble cut and a treble boost. All responses had their overall gain adjusted so that all produced the same loudness. Subjects made paired-comparison judgements while listening to continuous discourse in quiet and in babble noise. Whether subjects were judging on the basis of intelligibility or pleasantness, the NAL-R response was strongly preferred over three of the other four responses. Only for the high cut (relative to NAL-R) was there a significant proportion of subjects (although still a minority) that preferred the alternative response. The finding was sufficiently strong for Denis to consider the NAL-R response to be validated, and not to require any further modifications. Nonetheless, because there was a small proportion of subjects who preferred one of the alternatives, Denis recommended that clinicians use the paired-comparison procedure to systematically evaluate alternative responses whenever a client complains about the sound quality.
Gain prescription for linear hearing aids - severe to profound losses:
From the outset, Denis realized the prescriptions he was producing were only appropriate for patients with mild or moderate hearing loss. For such losses, every increase in hearing threshold requires more gain to be prescribed.
It was well understood that additional considerations applied to patients with severe and profound hearing loss. For example, it was difficult to achieve sufficient gain to be useful at a frequency when the hearing loss approached 120 dB HL. Furthermore, even if audibility could be achieved, the patient would be unlikely to extract useful information at that frequency due to diminished spectral and temporal resolution. Denis reasoned that for lesser (severe and profound) losses the value of amplification must progressively decrease as hearing loss increased. Consequently, progressive variations to the prescription formula should be necessary.
To determine the nature of these variations, Denis and colleagues fit 44 adult and 14 child subjects with several different frequency responses (Byrne, Parkinson & Newall, 1991). Each subject carried out a several-week home trial with each response, at the conclusion of which speech intelligibility was measured. After all home trials for a subject were completed, the responses were compared in a paired-comparison procedure. As expected, for most of the subjects, the best response had a higher average gain, and less high-frequency emphasis than that prescribed by the NAL-R response. The NAL-R response was most in error for those subjects with the best low-frequency hearing and the worst high-frequency hearing. This observation led to the finding that the discrepancy in slope from the NAL response was moderately correlated with the subject's hearing loss at 2 kHz. We turned the experimental results into yet another formula, which became known as NAL-RP, (revised-profound) and again reprinted the slide rules.
Effective audibility and hearing loss desensitisation:
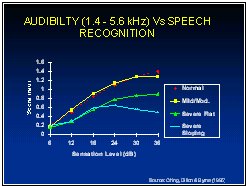
Although the experimental results with severely and profoundly hearing-impaired subjects clearly showed that gain should be de-emphasised when the loss becomes too great, there was an unsettling amount of individual variation. We did not feel we had a good understanding of the factors leading to reduced speech intelligibility for people with severe and profound hearing loss and their consequences for hearing aid prescription. Consequently, we initiated, and Teresa Ching carried out, an extensive study examining the ability of subjects to understand speech filtered in different ways and presented at a wide range of levels. Subjects with normal hearing through severe to profound loss, with sloping and flat configurations, were tested. All speech scores were compared to those predicted using the Speech Intelligibility Index (SII) model, which was previously known as the Articulation Index model (Ching, Dillon Byrne, 1998).
Results with high-pass filtered speech were particularly interesting. As expected, subjects with sloping losses that extended into the severe hearing loss range in the high frequencies achieved speech intelligibility scores much lower than the SII model predicted. Further, these deficiencies were particularly evident at the highest sensation levels. For this group of subjects as a whole, increasing the sensation level (SL) of the speech peaks above about 20 dB produced little further increase in intelligibility. What's worse, increasing the SL from 30 to 35 dB actually caused a significant decrease in intelligibility. It seems that for these subjects, on average, a little audibility in the high frequency region is usually worthwhile, but further audibility may be counterproductive.
As we wished to predict speech intelligibility for different frequency response shapes, it was clear that the SII method would have to be modified in some way. To achieve this, we defined the term ''Desensitized audibility'' (Ching et al, 2001). In the conventional SII model, contributions to audibility at each frequency increase linearly from 0 to 1 as the sensation level of the speech peaks increase from 0 to 30 dB.
Desensitized audibility was defined so that it increased from 0 to some maximum value less than 1, and we allowed the relationship between sensation level and desensitized audibility to be curvilinear. The actual maximum value, and the curvature were calculated by fitting the observed speech intelligibility to the effective audibility model. This modification produced a substantial increase in the accuracy with which intelligibility could be predicted for people with severe and profound loss. Once the various coefficients in the modified model were calculated, desensitized audibility could be plotted against sensation level, for different frequencies and degrees of hearing loss. The resulting curves dramatically show the ineffectiveness of high-frequency speech cues for people with losses of 70 dB or more in the high frequencies. Information up to 2 or perhaps 3 kHz can be well used, even for losses up to at least 80 dB HL. By contrast, speech information around 4 kHz appears to be much more degraded by hearing loss. Perhaps the timing cues carried by the low and mid-frequency region are less affected by hearing loss than the spectral cues carried in the high-frequency region.
Although the concept of desensitized audibility allows us to better estimate speech intelligibility for any combination of hearing loss, input level and gain-frequency response, the results are applicable only to the average person with the degree of loss for which the calculation is performed. Some individuals perform considerably better, and some considerably worse than average. In an effort to understand the reasons for this, we measured the frequency and temporal resolution of the same subjects for whom we had measured speech intelligibility. As expected, at each frequency there was a strong correlation between frequency selectivity and hearing threshold, and between temporal resolution and hearing threshold. As was also expected, for any degree of loss there was also a significant range of variability in frequency selectivity and temporal resolution. Unfortunately, there were only small correlations between these psychoacoustic measures and intelligibility measures once the variation of psychoacoustic measures with hearing thresholds was taken into account. The inability to accurately predict speech intelligibility for an arbitrary gain-frequency response for an individual aid wearer remains a major obstacle to devising optimal prescriptions for individuals with severe and profound hearing loss. Identifying dead regions in the cochlea (Moore, 2000) may be helpful, but as such regions should also be associated with greatly reduced frequency selectivity, we thought that our measure of frequency selectivity would have allowed for this.
Gain prescription for non-linear hearing aids:
At the time we started work on the NAL-NL1 prescription procedure there were already several non-linear prescription procedures. For example; FIG6, DSL[i/o], IHAFF/CONTOUR/VIOLA, RELM/LGOB, and various other methods proprietary to hearing aid manufacturers.
Why did we bother making another prescription method? Although we cannot be certain what rationale all the proprietary methods are based on, the remaining methods are all based on the concept of loudness normalization and we suspected that the proprietary methods were too. At any frequency, loudness normalization aims to prescribe sufficient gain that the hearing aid user will assign the same loudness as would a normal-hearing person listening to the same sound.
Denis Byrne postulated several reasons why normalizing loudness should not be the best thing to do:
- It is not clear why normal loudness should be important - normal hearing people communicate in a wide range of situations in which overall loudness and the balance of loudness across frequencies vary widely, seemingly without any adverse consequences.
- Our auditory system evolved in less noisy, pre-industrialised, pre-amplified times, and presumably has been optimized for those quieter times.
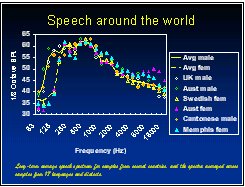
- The research described above strongly supports the belief that across frequency, all speech bands should be equally loud for maximum intelligibility, whereas the low frequency speech bands are normally louder than the high frequency bands (Keidser et al (2000). (It is, of course, an assumption that we should fit hearing aids to maximize intelligibility, but this seems a reasonable assumption in at least some circumstances).
- For people with normal hearing, loudness normalization requires a flat frequency response, and a flat response does not maximize speech intelligibility in difficult listening situations (Walker, 1997).
- Loudness normalization requires a very low compression threshold, whereas hearing aid wearers usually prefer higher compression thresholds (at least for single-channel fast-acting compressors) (Barker & Dillon, 1999; Storey et al. 1998).
To derive the NAL-NL1 procedure, we made the following four assumptions:
- Hearing aid users prefer a response that maximizes intelligibility.
- Speech intelligibility, on average, can be predicted using our modification of the SII procedure.
- Hearing aid users do not want the overall loudness to be any greater than that perceived by normal hearing people.
- Overall loudness can be predicted, on average, using the Moore and Glasberg (1998) loudness model.
Assumption 3 was necessary, or else assumption 1 would cause us to amplify all input levels to the same output level - one at which intelligibility is maximized - and this constant output level is not likely to provide an acceptable listening experience. To turn these four assumptions into a prescription we did the following.
For an arbitrarily chosen input level, we calculated the loudness that would be perceived by the average normal-hearing listener. We then selected an audiogram, and in a high-speed computer, juggled the insertion gain curve until the predicted speech intelligibility was maximized without exceeding the normal loudness constraint. This process was repeated for 51 representative audiograms and input levels from 40 to 90 dB SPL. As the process was too complex and time consuming for clinical use, we then fitted an equation to the results so that insertion gain could be more simply calculated from the audiogram and input level of the speech. As with its NAL predecessors, the gain at any frequency depends on the entire audiogram, not just the loss at that frequency.
Two modifications to the prescription were necessary. As with procedures that normalize loudness one frequency at a time, the assumptions require compression to be prescribed down to the threshold of normal hearing. As mentioned above, hearing aid wearers do not prefer very soft sounds to be amplified to normal loudness. Consequently, linear amplification is prescribed for low input levels. To achieve this, a compression threshold is prescribed such that speech at an overall level of 52 dB SPL just causes each channel of a multi-channel hearing aid to go into compression. The second modification was to lower the gain whenever high level inputs cause the output to be sufficiently high to require limiting, using the NAL-RESR method (outlined later in this article).
When the loudness model is used to observe the consequences of the prescription, a very reassuring phenomenon occurs. For mild and moderate hearing losses, the 1/3 octave bands of speech across the mid-frequency range are observed to be approximately equal in loudness. Recall that the original 1976 NAL formula was derived by assuming that this should be the case, and that the evaluation research strongly supported this aim. For the NAL-NL1 prescription, there is no such assumption implicit in the derivation, but rather equal loudness is the consequence of the desire to maximize speech intelligibility.
However, there is one twist that was not built into the earlier thinking. With NAL-NL1, as the input level decreases, the frequency range over which the speech bands are equally loud shrinks, with lower and higher frequencies dropping off in loudness. The reason is that at low input levels, the maximum allowable total loudness (i.e. normal loudness) is low, and intelligibility can be maximized by concentrating audibility in the frequency range where the most information can be extracted. For a mild or moderate loss, this is the mid-frequency region, for severe or profound loss, preference is also given to the region of least loss. Although the NAL-NL1 prescription has been theoretically derived, the prescriptions for a 70 dB SPL input level are amazingly similar to those from the NAL-RP procedure, which has been much more influenced by empirical observations. This convergence is also highly reassuring.
Not surprisingly, NAL-NL1 prescriptions are different from loudness-based procedures such as FIG6 or DSL[i/o] (Byrne et al., 2000). Differences from these procedures are most marked for:
- Flat losses - NAL-NL1 prescribes less low-frequency gain
- Steeply sloping losses - NAL-NL1 prescribes less high-frequency gain
- Severe or profound losses - NAL-NL1 prescribes less gain where the loss is greatest
NAL-NL1 can be used via the stand-alone clinician software (see www.nal.gov.au for details). It is also progressively being included within the fitting menus of most leading hearing aid manufacturers.
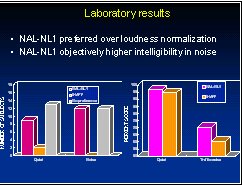
In keeping with Denis' philosophy, an evaluation of NAL-NL1 relative to loudness normalization was performed by comparing its effectiveness to loudness normalization (Keidser & Grant, 1999). As threshold-based procedures only approximate loudness normalization, we chose the IHAFF protocol employing the CONTOUR loudness scaling method and the VIOLA fitting program as the reference condition.
Twenty-four subjects compared the procedures in laboratory paired-comparison trials, laboratory measures of speech intelligibility and field trial familiarization and paired-comparison conditions. Both the laboratory and field trial results strongly favoured NAL-NL1 over the loudness normalization alternative. Preferences most strongly favoured NAL-NL1 when the differences between the two prescriptions was largest.
Prescribing gain for infants and children:
To what extent do infants and children hearing aid prescriptions different from adults? One aspect of this question is easy to answer: children have smaller ear canals and this difference must be accounted for in some way. Let us first assume that the goal is to achieve the same SPL at the eardrum as would be applied to an adult with the same loss (when thresholds of hearing for both are expressed as SPL in the ear canal). The easiest way to achieve this is to measure the real-ear to coupler difference (RECD) for the child (Moodie, Seewald & Sinclair, 1994), and use this to calculate the coupler gain that would achieve the target real-ear aided gain (REAG; defined as SPL in the ear canal minus SPL in the sound field outside the head):
Coupler gain = REAG - RECD - MLE.
ALIGN=''CENTER''>The third term, microphone location effects (MLE) can satisfactorily be ignored for BTE hearing aids. RECD must not be ignored; during the first few months of life, RECD can be up to 20 dB higher than is measured for the average adult. It approximates adult values by age five years.
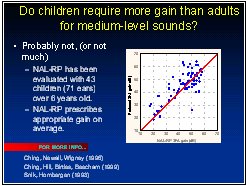
The second aspect of how children differ is much more difficult. Should children receive the same aided SPL as adults with the same hearing loss? It is commonly stated that because normal hearing children need a sensation level higher than adults to achieve optimal performance, hearing-impaired children should be given more gain than adults.
Denis Byrne was certainly aware of this, as he systematically measured the effect in the 1960's and published it 20 years later (Byrne, 1983). It is not at all clear, however, that the phenomenon requires children to be given more gain. Perhaps it justifies them receiving more gain for low input levels, but cannot justify more gain for medium-level inputs and especially high-level inputs. Note that a consequence of providing more gain for low-level inputs but not for high-level inputs would be that a higher compression ratio is prescribed for children than for adults. There is, as of yet, little or no experimental evidence concerning how much gain is needed for low-level sounds for either children or adults.
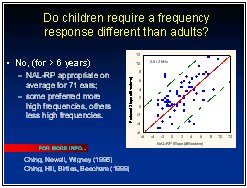
There is, however, a wealth of evidence concerning the gain and frequency response needed for children for mid-level sounds. Several studies have shown that the gain-frequency response prescribed by the NAL-RP response is just as appropriate for children as it is for adults (Byrne, Parkinson Newall, 1990; Ching, Newall & Wigney, 1997; Snik et al, 1995). The data suggest that at most, the children prefer about 3 dB more real-ear gain than adults with the same degree of loss. These studies are mostly based on the gain and frequency response preferred by children over the age of 6 years. These studies have the limitation that the child's preferred response may be influenced by the response to which the child has become accustomed. NAL is currently performing a study in collaboration with the University of Western Ontario to resolve this question.
NAL is also developing new evaluation methods that will enable clinicians to more objectively determine the relative effectiveness of different amplification characteristics in children as young as three months of age. The first of these methods is functional assessment, in which detailed structured interviews of parents and/or teachers/interventionists enables an effectiveness score to be assigned to whatever amplification condition the child has been wearing during the previous few weeks. The second method is an objective electrophysiological measure based on the cortical response to selected speech and non-speech sounds. Children hear the sounds through a loudspeaker while wearing their hearing aids. The research has so far established that for normal-hearing infants, different speech and non-speech sounds elicit different cortical responses. We hope that the methods will allow evaluation and fine-tuning to be carried out for individual children in the hearing clinic, as well as being suitable for research evaluation of alternative prescription strategies.
Prescription of maximum output:
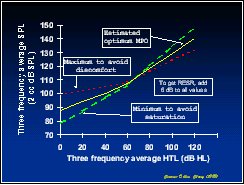
The maximum output of a hearing aid is variously called OSPL90, SSPL, SSLP90, and MPO when measured in a 2 cc coupler, and RESR (real-ear saturated response) when measured in the ear canal. Although it is common for researchers to assume that maximum output should be set equal to the aid wearer's loudness discomfort level (LDL), Denis Byrne pointed out that this was very much an assumption. Instead he suggested that there were really two constraints. One was that the maximum output should be sufficiently low to avoid discomfort in real life, (which is not necessarily the same as keeping OSPL90 below the clinically measured LDL). The second constraint is that the output level should be high enough to achieve an adequate sensation level without causing excessive limiting in the hearing aid. Consequently, we devised a prescription procedure that took both these constraints into account by prescribing maximum output to be halfway between the value that just avoided discomfort and the value that just avoided excessive saturation of a 75 dB SPL speech signal (Dillon and Storey, 1998). The procedure, referred to as NAL-SSPL, prescribed three-frequency average OSPL90 on the basis of three-frequency average hearing thresholds.
Naturally, we evaluated the effectiveness of the prescription. Initially, we sought to experimentally find the optimal value of OSPL90 by allowing the subjects to switch between different OSPL90 values while wearing their hearing aids during their daily activities (Storey et al, 1998). We quickly found that subjects often had no clear preference, even when the OSPL90 values being compared were 8 dB apart. Instead, we slightly modified the aim to find the lowest and highest acceptable OSPL90 values, still using pairwise comparisons of different values. On average, the prescription neither under-nor over-estimated the midpoint between the lowest and highest acceptable values.
In case the subjects had not been adequately exposed to high level sounds in their daily aid use, and to gather more insights into the problems caused by an excessively low OSPL90, we also investigated the lowest and highest acceptable OSPL90 values using laboratory equipment. For the laboratory experiment, we used both peak clipping and compression limiting to control the maximum output of the laboratory hearing aid. The laboratory results were very similar to those of the field trial. For the peak-clipping hearing aid, prescription lay within the acceptable range for most of the subjects. There was a wider range of acceptable OSPL90 values for compression limiting than for peak clipping. This wider range occurred because for the compression limiter, subjects were not concerned about distortion as OSPL90 decreased, only about inadequate loudness.
Overall, the results suggested that the NAL-SSPL procedure prescribed values that were typically neither too high nor too low and we concluded the procedure did not require modification. However, because the prescription did not produce an acceptable OSPL90 for approximately 20% of the subjects, we concluded that the procedure is suitable only for determining the initial value of OSPL90. Further, we recommended that evaluation of the appropriateness of the prescribed value should be carried out for all patients.
For hearing aids that can independently alter the maximum output in different frequency ranges, prescription of maximum output at different frequencies is necessary.
We provided such a prescription (NAL-RESR) by applying the same principles as for NAL-SSPL, except that the calculations were carried out separately at each frequency (Dillon, 2001). There were two other differences. First, the prescription was expressed in terms of maximum output in the real ear (hence RESR) so that the same values apply from infants through to adults, and so that the same values apply for all hearing aid types, from deeply seated CIC hearing aids through to minimally seated BTE earmolds. Conversion to an OSPL90 target simply requires individual (or average) RECD values to be subtracted from the RESR target. The second modification involves an allowance for power summation and loudness summation in multi-channel hearing aids. Where the limiting occurs independently within each channel of a multi-channel hearing aid, an intense broadband sound will easily cause loudness discomfort even if the sounds in each channel are limited to below their respective discomfort levels.
Prescriptions for multi-memory hearing aids:
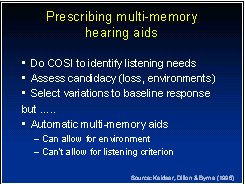
The above discussion perhaps implies there is a single optimal prescription for each client. In fact, there is ample evidence (Keidser 1995) that the optimal prescription varies with both the type of background noise and the desired listening goal (e.g. maximizing intelligibility versus minimizing annoyance of the noise).
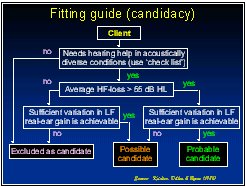
An extensive study into how prescriptions should vary with the listening situation established the general principal that gain should be decreased in those regions where the signal-to-noise ratio is poorest (Keidser, Dillon & Byrne, 1996). The same study also established some criteria for deciding which patients were candidates for multi-memory hearing aids. The most likely candidates are those; wishing to use their hearing aids in diverse situations, have a high-frequency loss exceeding 55 dB HL, and have sufficient low-frequency loss that they require more than 0 dB gain at 500 Hz. It is worth mentioning that hearing aids are becoming increasingly capable of switching responses or gradually altering their response as the characteristics of the acoustic environment alter, thus removing some of the need for the patient to do this.
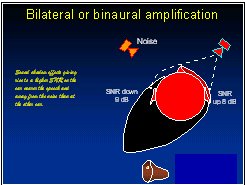
Bilateral amplification and localization:
Denis was a strong proponent of bilateral amplification (the fitting of two hearing aids) at a time when only a very small proportion of patients was receiving two aids. While many researchers were focussed on whether normal binaural interactions would occur within the auditory system of people with hearing loss, Denis quickly realized that the major advantage of having two hearing aids was that in many situations, one ear would be closer to the talker and/or further away from the dominant noise source than the other ear. Consequently, head baffle effects would cause the output from one hearing aid to be clearer than the output from the other. If a person wore only one hearing aid, he or she would often lose the opportunity to hear amplified sound on the side of the head with the better signal-to-noise ratio. The clarity of Denis' views on this issue can be seen in the following quotes from Byrne (1981):
- ''Binaural fitting should not be regarded as a special technique for a few selected cases, but rather it should be seriously considered for all hearing aid candidates unless there are definite contraindications''.
- ''Audiological contraindications are few and can be reduced almost to saying that we should fit all cases except where one ear is unaidable because of too little or too much hearing''.
- ''Head shadow advantage is virtually bound to occur if both ears receive a reasonable level of aided signal and have reasonable speech discrimination''.
Denis acquired an early interest in sound localization. He pointed out that good localization ability had several advantages:
- Survival - avoiding danger, finding food
- Aesthetic - enjoy locating sound makers
- Psychological well-being - good spatial orientation and externalization of sounds
- Lipreading - quickly locating the talker in group discussions
- Noise suppression - possible relationship to hearing speech in noise
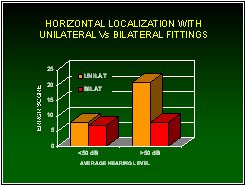
Denis and colleagues carried out many experiments that quantified the difficulties hearing-impaired people face while localizing the source. His research showed that vertical localization ability is greatly diminished by high-frequency hearing loss -- and that hearing aids do not restore this ability. Horizontal localization ability is diminished by low-frequency hearing loss whenever the combination of the hearing loss and the input signal causes poor audibility in either ear (Byrne & Noble, 1998; Byrne, Noble & LePage, 1992). Not surprisingly, hearing aids enhance horizontal localization whenever they enable an otherwise inaudible signal in either ear to be clearly audible in both ears (Dermody & Byrne, 1975). For patients with good low-frequency hearing, all hearing aids have to do is not get in the way. This is achieved by using open earmolds or shells.
Objectives in hearing aid fitting:
During his final years, Denis became interested in broadening the goals of hearing aid prescription. He pointed out that prescription methods were either totally focussed on loudness (e.g. all the loudness normalization methods), or on speech intelligibility (e.g. the early NAL methods) or on a combination of the two (e.g. NAL-NL1). Whenever a clinician fits a hearing aid, however, the clinician inevitably asks the patient ''how does that sound?'' which invites a response in terms of sound quality.
Denis thought that as a fitting goal is to achieve things such as comfort, naturalness, localization, externalization, detection of environmental sounds, and tonal balance, then such issues ought to be taken into account in the prescription wherever possible. He commented that compromises might sometimes be needed, such as additional low-frequency emphasis for good localization of soft sounds but additional high-frequency emphasis for good intelligibility of soft speech.
In the first experiment to arise from this line of thinking, Karolina Smeds (visiting scientist to NAL in 2001) has measured the loudness and SPL preferred by normal hearing people for a variety of speech and non-speech sounds while they watched the listening situation on a video screen. Subjects preferred any sounds above about 65 dB SPL to be decreased in level compared to their naturally occurring levels. The experiment is being replicated with hearing-impaired people and in actual real-life situations. The considerable challenges in broadening the perspective of the prescription process are firstly learning how to quantify each of the factors, and secondly, determining how any trade-offs should be made.
In conclusion:
Denis Byrne did not invent hearing aid prescription. However, through his careful, systematic, thoughtful, practical, self-critical research, he made it possible for clinicians to use prescriptive procedures based on sound rationales and an appropriate evidence base.
What can we learn from his approach? When clinicians are presented with a new procedure or device, they can ask three key questions:
- What is the rationale behind the procedure or device?
- What assumptions have been made in producing the procedure or device?
- What actual evidence supports using the procedure or device relative to alternative approaches?
When we researchers devise a new procedure or device we can tell ourselves that a small part of our job is done. Howevere, it is only after we have evaluated the effectiveness of the thing we have produced, relative to reasonable alternatives, revised our invention as necessary, and continued around the improvement loop until there is diminishing return, can we consider that we have really done our job.
A complete set of PowerPoint slides for the talk can be downloaded from www.nal.gov.au. The various NAL prescriptions are described in more detail (but still in summary form) in Dillon (2001). Complete descriptions can be found in the references cited.
REFERENCES:
Barker, C. and Dillon, H. Client preferences for compression threshold in single-channel wide dynamic range compression hearing aids. Ear & Hear. 1999; 20(2):127-139.
Byrne, D. Clinical issues and options in binaural hearing aid fitting. Ear & Hear. 1981; 2(5):187-193.
Byrne, D. Word familiarity in speech perception testing of children. Aust J Audiol. 1983; 5(2):77-80.
Byrne, D and Cotton, S. Evaluation of the National Acoustic Laboratories' new hearing aid selection procedure. J Speech Hear Res. 1988; 31(2):178-186.
Byrne, D and Dillon, H. The National Acoustic Laboratories' (NAL) new procedure for selecting the gain and frequency response of a hearing aid. Ear & Hear. 1986; 7(4):257-265.
Byrne, D.; Dillon, H.; Ching, T.; Katsch, R., and Keidser, G. The NAL-NL1 procedure for fitting non-linear hearing aids: Characteristics and comparisons with other procedures. J
Amer Acad Audiol. 2001; 12(1):37-51.
Byrne, D; Noble, W, and LePage, B. Effects of long-term bilateral and unilateral fitting of different hearing aid types on the ability to locate sounds. J Amer Acad Audiol. 1992; 3(6):369-382.
Byrne, D; Parkinson, A, and Newall, P. Hearing aid gain and frequency response requirements for the severely/profoundly hearing impaired. Ear & Hear. 1990; 11(1):40-49.
Byrne, D and Tonisson, W. Selecting the gain of hearing aids for persons with sensorineural hearing impairments. Scand Audiol. 1976; 5:51-59.
Carhart, R. Selection of hearing aids. Archives of Otolaryngology. 1946; 44:1-18.
Ching, T. Y.; Newall, P., and Wigney, D. Comparison of severely and profoundly hearing-impaired children's amplification preferences with the NAL-RP and the DSL 3.0 prescriptions. Scand Audiol. 1997; 26(4):219-22.
Ching, T. Y. C.; Dillon, H., and Byrne, D. Speech recognition of hearing-impaired listeners: Predictions from audibility and the limited role of high frequency amplification. J Acoust Soc Amer. 1998; 103(2):1128-1140.
Ching, T. Y. C; Dillon, H; Katsch, R, and Byrne, D. Maximizing effective audibility in hearing aid fitting. Ear & Hear. 2001; 22(3):212-224.
Ching, TYC; Hill, M; Birtles, G, and Beecham, L. Clinical use of paired comparisons to evaluate hearing aid fitting of severely/profoundly hearing impaired children. Aust J Audiol. 1999; 21(2):51-64.
Dermody, P. and Byrne, D. Auditory localization by hearing-impaired persons using binaural in-the-ear hearing aids. Brit J Audiol. 1975; 9:93-101.
Dillon, H. Hearing Aids. Sydney: Boomerang Press; 2001.
Dillon, H and Murray, N. Accuracy of twelve methods for estimating the real ear gain of hearing aids. Ear & Hear. 1987; 8(1):2-11.
Dillon, H. and Storey, L. The National Acoustic Laboratories' procedure for selecting the saturation sound pressure level of hearing aids: theoretical derivation. Ear & Hear. 1998; 19(4):255-66.
Keidser, G. The relationship between listening conditions and alternative amplification schemes for multiple memory hearing aids. Ear & Hear. 1995; 16(6):575-586.
Keidser, G.; Dillon, H., and Byrne, D. Guidelines for fitting multiple memory hearing aids. J Amer Acad Audiol. 1996; 7:406-418.
Keidser, G. and Grant, F. Evaluation of loudness equalisation versus loudness normalisation. Presented at Hearing Aid Amplification for the New Millenium. Sydney, 1999.
Keidser G; Katsch R; Dillon H, and Grant, F. Relative loudness perception of low and high frequency sounds in the open and occluded ear. J Acoust Soc Amer. 2000; 107(6):3351-3357.
Moodie, K. S.; Seewald, R. C., and Sinclair, S. T. Procedure for predicting real-ear hearing aid performance in young children. Amer J Audiol. 1994; 3:23-31.
Moore, B. C. J. and Glasberg, B. R. A model of loudness perception applied to cochlear hearing loss. Auditory Neurosci. 1997; 3:289-311.
Snik, A. F.; van den Borne, P.; Brokx, J. P., and Hoekstra, C. Hearing aid fitting in profoundly hearing-impaired children: comparison of prescription rules. Scand Audiol. 1995; 24:225-230.
Snik, AF and Hombergen, GC. Hearing aid fitting of preschool and primary school children. An evaluation using the insertion gain measurement. Scand Audiol. 1993; 22(4):245-250.
Storey, L.; Dillon, H.; Yeend, I., and Wigney, D. The National Acoustic Laboratories' procedure for selecting the saturation sound pressure level of hearing aids: experimental validation. Ear & Hear. 1998; 19(4):267-79.
Walker, G. The preferred speech spectrum of people with normal hearing and its relevance to hearing aid fitting. Aust J Audiol. 1997; 19(1):1-8.
