
Learning Outcomes
After this course, participants will be able to:
- Explain the importance of patient-specific factors besides pure-tone audiometric thresholds for a hearing aid fitting and name factors that should be considered.
- Explain how the software-based fitting assistant (Connexx Hearing Profile) gathers information on the hearing characteristics and proposes an optimized first fit configuration for each patient.
- Describe how Connexx Hearing Profile supports the HCP to achieve better fittings for his patients to determine groups of HCPs and patients that will benefit in particular.
Introduction
Individual Perception of Hearing and its Influence on the Hearing Aid Fitting
In general, the gain and output for the initial fitting of hearing aids is derived from the individual’s hearing thresholds in quiet, which is one of the most important factors to determine the frequency-dependent amplification (Dillon, 2001). However, these derived values are for the average patient; hearing care professionals (HCP) and hearing-impaired people report that this does not always result in an entirely satisfying hearing aid fitting with respect to benefit and acceptance. One task of audiologic research is to analyze this gap and shed light on the relation between the individual’s impaired perceptions and the technical solutions that could be provided by hearing aid algorithms.
It is known that speech intelligibility is not completely explained by the pure-tone audiometric thresholds (Lazarus, Sust, Steckel, Kulka & Kurtz, 2007; Humes, 2002). This implies that there are other patient-specific factors that influence speech understanding, and in particular, speech understanding in background noise. Research has focused, among other things, on age (Dubno, Dirks, & Morgan, 1984; Gordon-Salant, 2005), cognition (Pichora-Fuller, Schneider, & Daneman, 1995; Lunner, 2003) and various psychoacoustic measures such as frequency selectivity, temporal fine structure sensitivity and modulation thresholds (Hopkins and Moore, 2011; Bernstein, et al., 2013).
In relation to the individual fine tuning of hearing aid settings (e.g. gain adjustments, noise reduction strength, etc.) it appears that besides the hearing threshold, the patient’s working memory and its executive functions, like inhibition of irrelevant and focus on relevant input (Lunner & Sundevall-Thorén, 2007; Neher & Wagener, 2014; Neher, Wagener, & Fischer, 2015), personality (Hutchinson, Duffy, & Kelly, 2005) and the acceptable noise level (Neher & Wagener, 2016) come into play. While this research usually uses extreme hearing aid settings, Serman, Fischer, Herbig, and Hannemann (2017) have shown that there are also relations between the benefit from several hearing aid settings that are suitable for daily-life and individual factors of the hearing impaired, such as age, tonal working memory, loudness sensitivity and hearing aid experience. Furthermore, self-reported hearing difficulties and the outcome expectancy for hearing aid use were related to the hearing aid settings. These findings resulted in the development of software-based assistance to support in optimizing the fitting, which is referred to as the Connexx Hearing Profile. It provides individualized proposals for the initial hearing aid settings. Beyond this, the Connexx Hearing Profile is a software-based means that can leverage the interaction and communication between the hearing care professionals and their patients. In addition, it enables the patient to actively contribute to the fitting, which might result in an improved motivation to use hearing aids. The full concept of the Connexx Hearing Profile was assessed in a field study with respect to its effect on the hearing aid fitting success.
Short Description of the Connexx Hearing Profile
The Connexx Hearing Profile is part of the Connexx fitting software used to fit Signia hearing aids. It can be directly accessed via an icon on the toolbar at the top of the main fitting page (Figure 1; encircled in blue). It is designed to an active contribution of the patient. By answering a 6-item questionnaire and conducting a short sound quiz, the patient provides information about relevant factors for the individualized first fit. Complex mathematical algorithms evaluate the available information and propose the best hearing aid fitting for each patient. The resulting personal hearing profile proposes one of five optimized first fit configurations (Figure 1; encircled in green). Furthermore, an individual summary of the hearing personality is shown. It is directed to the patient but could be also used by the HCP to leverage the communication about hearing abilities and needs. (Figure 1; "Summary of your patient´s Hearing Profile“). The conduction takes about 5 to 10 minutes and is self-explaining to the greatest possible extend.
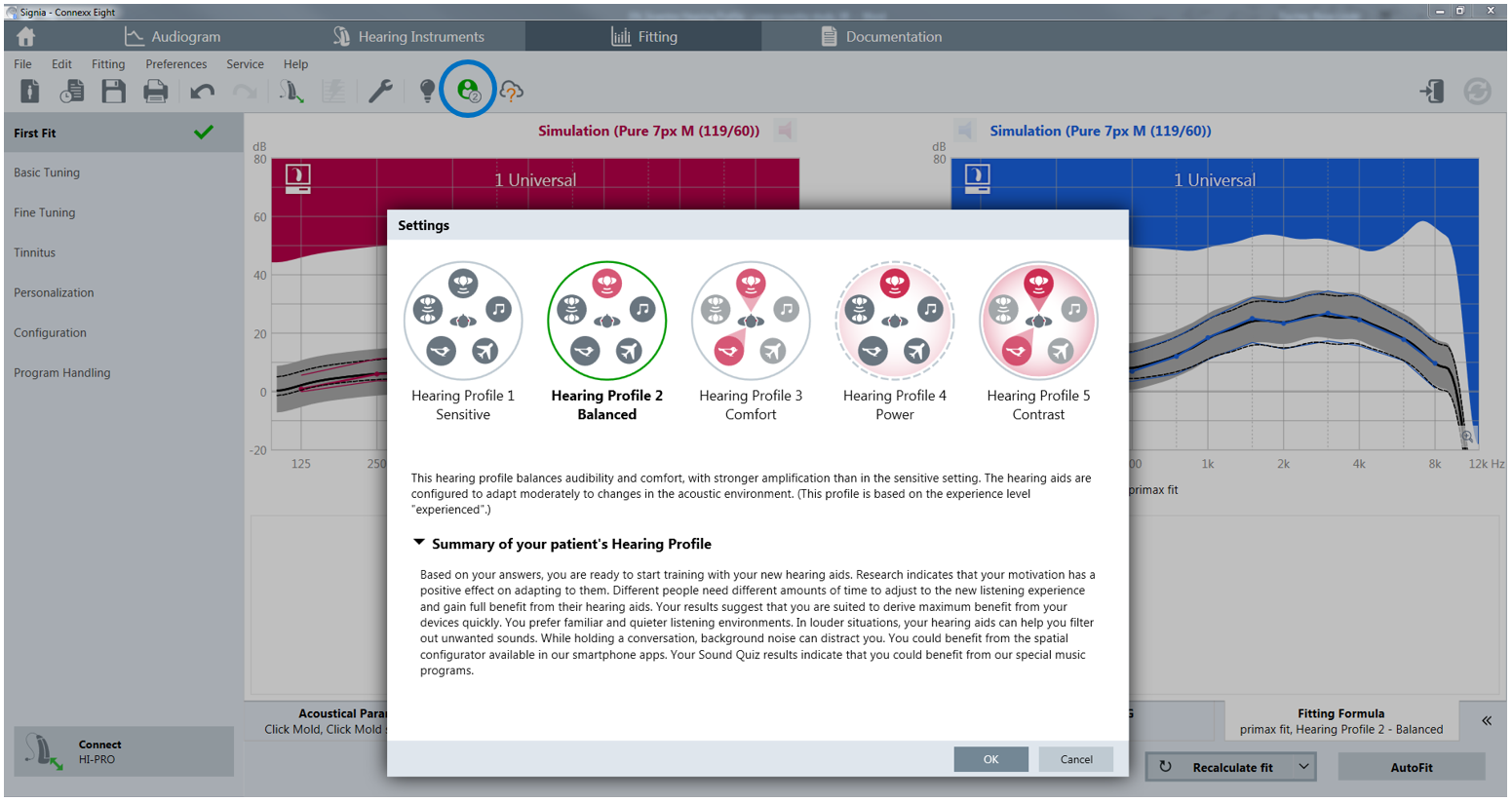
Figure 1. Resulting hearing profile screen once the icon has been clicked (upper bar, circled in blue) in the HCP’s view.
Study Design
Whereas Serman, Fischer, Herbig, and Hannemann (2017) verified the positive influence of the Connexx Hearing Profile on patient acceptance and listening effort. The current study addressed its usefulness in the HCP´s daily fitting routine, and the influence on the cooperation between the HCP and the patient. In comparison to the traditional method of fitting hearing aids, we evaluated whether the Connexx Hearing Profile provided suitable support for the HCP and whether the different course of the fitting procedure caused a positive effect on overall fitting success. In order to gather information that might have widespread implications, the study was conducted in various countries. Furthermore, not only the opinion of the HCPs but also of their patients was researched.
The study was conducted after the launch of the fitting software Signia Connexx 8.3 with the incorporated Connexx Hearing Profile for a period of four months (May to August 2017) in Germany (DE), Austria (AT), Poland (PL) and the United States (US).
Overall, 28 HCPs (AT: 7, DE: 8, PL: 6, US: 7) participated in this study. On average, they were 37 years old (range 26-69 years) and varied in their professional degree. Half of the participating HCPs reported being a hearing instrument specialist (HIS), whereas the other half were audiologists (Figure 2). The assumed number of fittings per year was on average 102 and showed no difference among the countries. The professional experience ranged between “unexperienced” (relatively new at fitting hearing aids) and 39 years (Mean = 12 years).
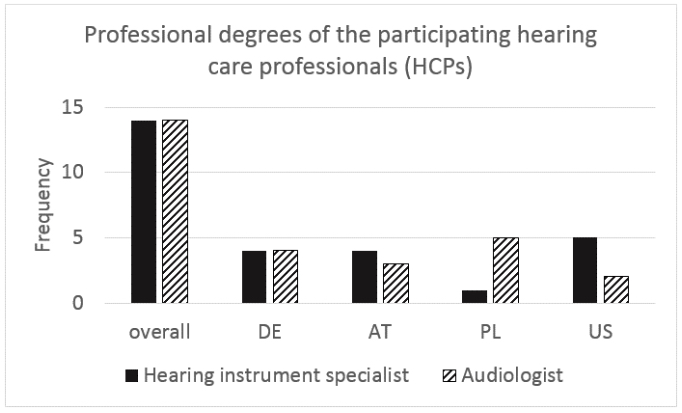
Figure 2. Professional degrees of the HCPs over the participating countries. For the analyses, the education levels “Assistant"/"Bachelor"/"Hearing instrument specialist” and “Master craftsman“/“Master" and “Audiologists” were grouped, respectively. During the course of this article, we will refer to the groups as a hearing instrument specialist (HIS) or audiologist.
The choice of the participating patients was decided by the HCP: Altogether, 319 hearing instrument wearers (evenly distributed across countries) participated in this study. Of this total, 163 were fitted with the standard workflow while 156 were fitted with the Connexx Hearing Profile. The two fitting workflows were alternated with sequential patients. Descriptive data on the patients are shown in Table 1.
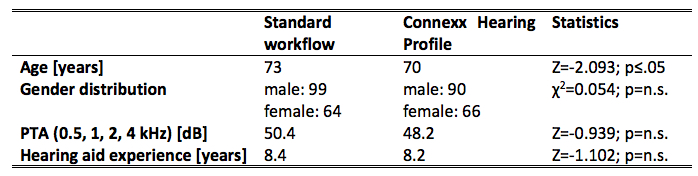
Table 1. Overview of subjects‘ statistics (Age, gender distribution, hearing loss, hearing aid experience). Statistical analyses were performed using Mann-Whitney-U-Test and Chi-square analysis.
Signia Primax Pure 13 RIC devices were used for the fitting of each patient. Receiver power level and acoustic coupling were individually selected by the HCP. In both fitting workflows open, semi-open or closed domes (Figure 3) were chosen.
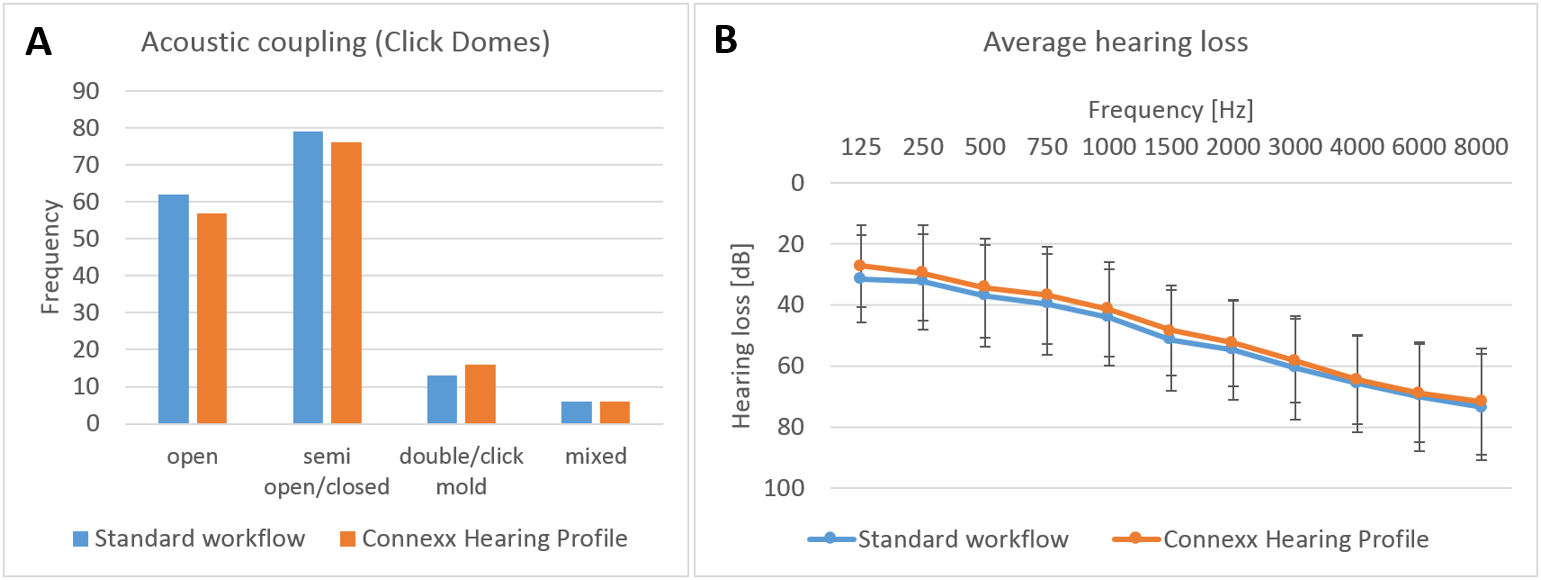
Figure 3. Acoustic coupling and average hearing loss. A) Distribution of the acoustic coupling over both fitting workflows. B) Average hearing loss in dB over both fitting workflows. Values are displayed as Mean±Standard deviation.
The general study protocol is shown in Figure 4. After an introductory meeting, the HCPs were introduced to the study protocol and the Connexx Hearing Profile. In the next step, the HCPs were invited to use the Connexx Hearing Profile on themselves. Finally, they were asked to evaluate the new fitting workflow in comparison to their routine way of fitting hearing aids by completing a questionnaire (Figure 4B). To capture possible changes in these opinions following use of the protocols, they completed the same questionnaire at the end of the study.
In the second part of the evaluation, the HCPs used either of the procedures to provide their patients with hearing aids in the first fit setting. If necessary, the HCP performed fine tuning until the patient was willing to take the hearing aids home for further testing. For this part, the patients and the HCPs were asked to rate the fitting process by questions that referred to the patient’s involvement and motivation as well as the provided information during the fitting (4-tier scale: strongly disagree – strongly agree).
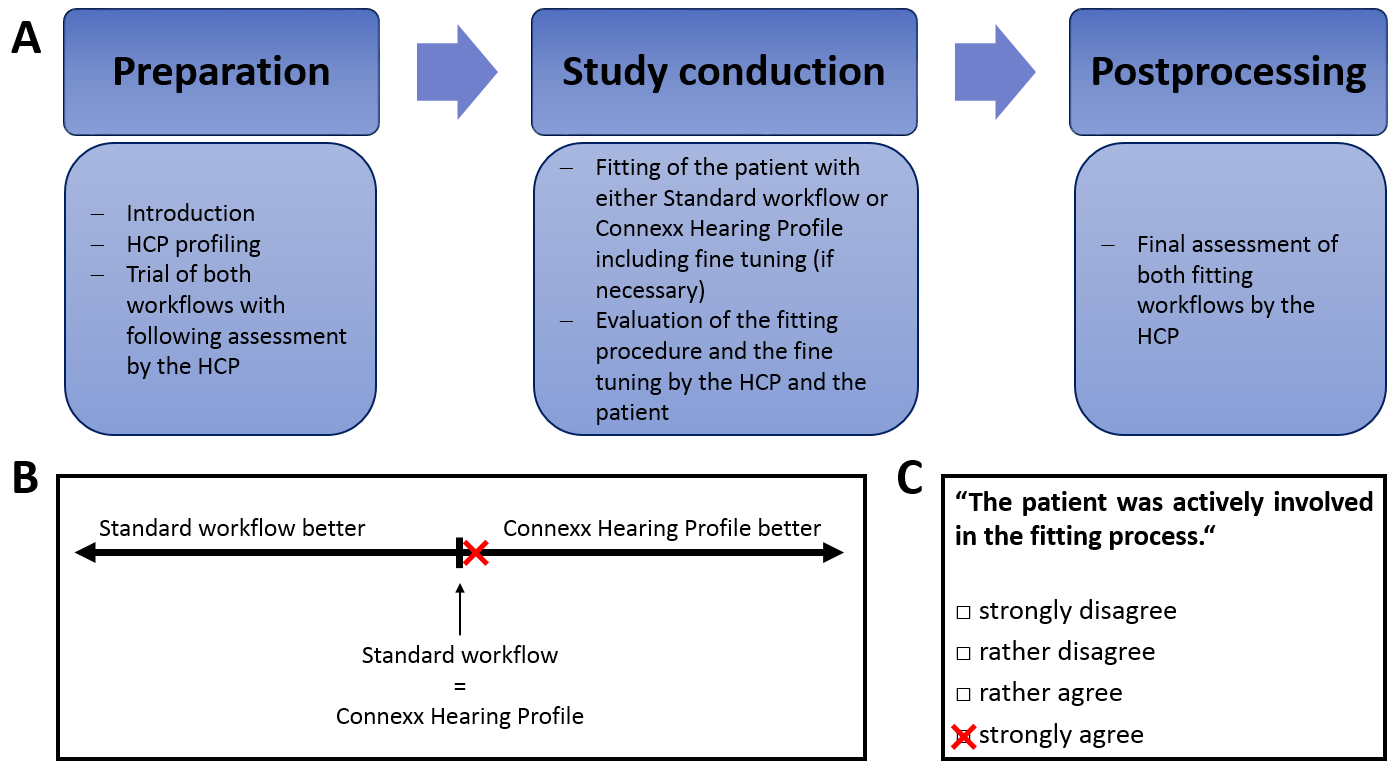
Figure 4. Study protocol and questionnaire examples. A) Schematic overview of the study protocol. B) The rating scale of the questionnaires in the beginning and at the end of the study. All HCPs compared the standard workflow with the Connexx Hearing Profile after the introduction of both fitting workflows and after all fittings. C) Sample from the questionnaires filled out for each subject. All HCPs evaluated their patients after the first part of the fitting procedure and after completing the fitting procedure. Furthermore, the patients themselves assessed the workflow after the fitting procedure, (if necessary) after the fine tuning and at the end of the entire session.
Results
In the following section, the fittings with the standard workflow and the Connexx Hearing Profile are compared, focusing either on the HCPs’ daily fitting routine (general benefits, influence of educational level) or the influence on the patient (general benefits, influence of the HCPs’ professional degree, suitability for specific patients).
Perspective of the Hearing Care Professional
In order to analyze the Connexx Hearing Profile’s impact on the HCPs’ fitting routine, both fitting workflows were compared regarding various properties in the beginning and at the end of the study (Figure 5). The ratings in the study’s beginning (black) and end (grey) are juxtaposed against one another and statistically significant differences, when present, are shown (deviations from the baseline via One-Sample-T-Tests).
General Advantages When Using the Connexx Hearing Profile
After the introduction of the Connexx Hearing Profile, the HCPs were already open-minded towards the new way of fitting. Whereas they did not foresee a disadvantage of any workflow regarding the fitting duration, they expected the Connexx Hearing Profile to benefit the patient’s involvement, motivation, and acceptance. Moreover, the HCPs anticipated to acquire patient information that would prove to be relevant concerning their work. The expectations were fulfilled: All HCPs still preferred the Connexx Hearing Profile over the standard workflow regarding these criteria at the end of the study (Figure 5).
While HCPs initially did not prefer any workflow in terms of utility, comprehensibility and the estimation of the fitting support, they favored the Connexx Hearing Profile at the end of the study for these factors. Furthermore, the gain prescription targets provided by the Connexx Hearing Profile (rated only at the end of the study) appeared more appropriate than those of the standard workflow.
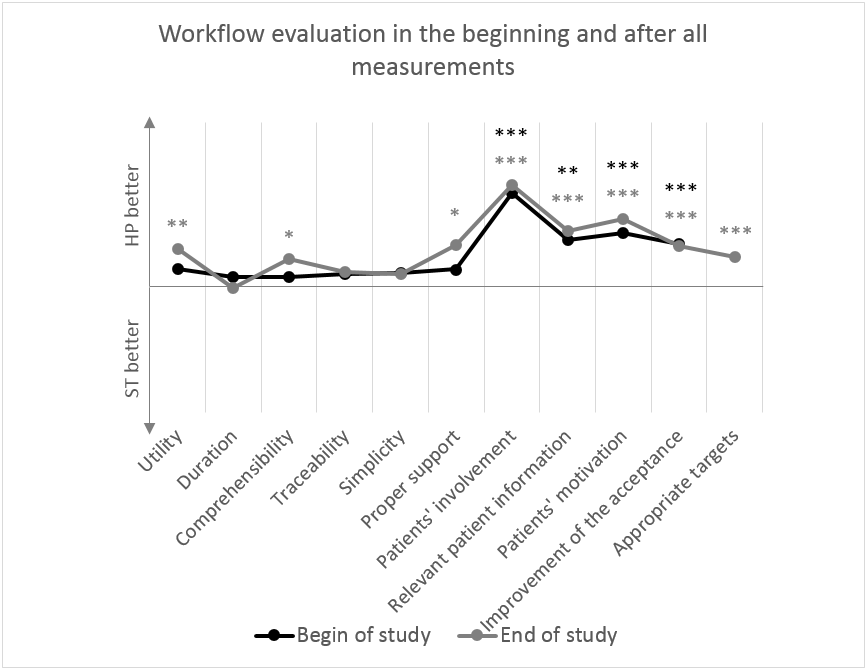
Figure 5. HCPs’ ratings in the beginning (black) and at the end of the study (grey). Values on the baseline represent no differences between standard workflow (ST) and Connexx Hearing Profile (HP) regarding this variable. Positive values indicate a preference for the Connexx Hearing Profile, whereas negative values imply a preference for the standard workflow. Deviations to the baseline were analyzed via One-Sample-T-Test.
Impact of the HCPs’ Professional Degree
The previous results referred to all HCPs. In this section, findings were clustered by HCP professional degree, i.e. hearing instrument specialists (HIS) and audiologists were analyzed separately regarding the aforementioned factors.
The initial HIS´ ratings differed from those of the audiologists´ assessments: HCPs with the initial professional degree (HIS) rated the comprehensibility (t(26)=1.685; p=.104, Figure 6) and the provided support for the fitting (t(26)=1.660; p=.109) higher than HCPs with a more advanced education (audiologists). These differences were balanced at the end of the study when all HCPs independently on their professional degree preferred the Connexx Hearing Profile over the standard workflow. In addition, HIS reported to receive a higher extent of valuable information out of the Connexx Hearing Profile compared to the standard workflow (1.96 vs. 1.56; Z=-2.813; p≤.01; not shown).
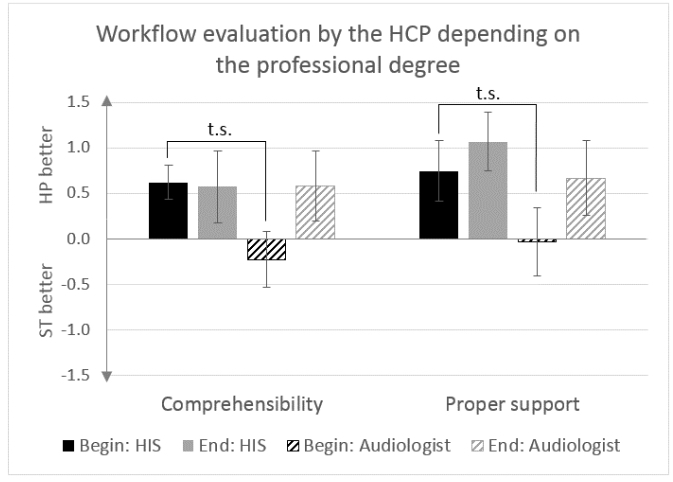
Figure 6. HCPs‘ ratings at the beginning and at the end of the study depending on the professional degree. Ratings of HCPs with different professional degrees (“HIS,” “Audiologist”) from the beginning (black, black-striped) and the end of the study (grey, grey-striped) are depicted. Positive values indicate a preference for the Connexx Hearing Profile, whereas negative values imply a preference for the standard workflow. Values are displayed as Mean±Standard error of the mean (SEM).
Our findings suggest that in particular, HIS could benefit from the Connexx Hearing Profile regarding post-fitting fine tuning. In both fitting workflows, audiologists spent up to 10 minutes on the fine tuning, while the HIS required more time in the standard workflow. During the use of the Connexx Hearing Profile, the HIS reduced the time needed to perform the fine tuning (Z=-1.682; p=.093, Figure 7A) and even outpaced the audiologists (Z=-1.736; p=.082, Figure 7A). The patients’ satisfaction remained unchanged and the willingness to take home the hearing aids could be even increased towards the standard workflow (Z=-3.368; p≤.01, Figure 7B) and also towards the audiologists using the Connexx Hearing Profile (Z= -2.549; p≤.05, Figure 7B).
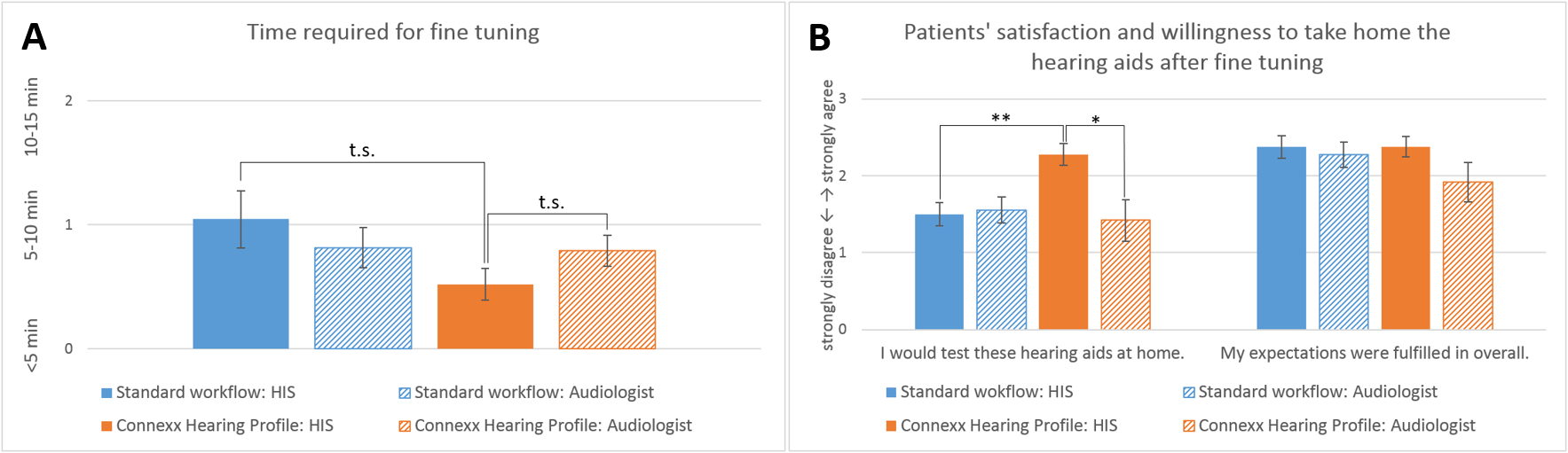
Figure 7. Fine tuning depending on the HCP’s professional degree. A) Fine tuning duration compared between HIS and audiologists. B) Patient satisfaction and willingness to take the hearing aids home for further testing after fine tuning compared between HIS and audiologists. Values are displayed as Mean±SEM.
Collectively, the Connexx Hearing Profile offers the following advantages to the HCPs:
- Relevant information for an individual fitting
- Appropriate fitting targets
- Improved cooperation between HCPs with entry-level education and their patients
- Reduced fine tuning duration
- Increased willingness to take home the hearing aids
- Useful, software-based means to actively involve the patient
- Higher patients’ motivation and acceptance.
Impact on the Patient
To analyze the impact of using the Connexx Hearing Profile on the patient, all HCPs evaluated their patients after the first part of the fitting procedure and after completing the entire fitting procedure. Furthermore, the patients themselves assessed the workflow after the fitting procedure, (if necessary) after the fine tuning and at the end of the entire session.
General Advantages of the Connexx Hearing Profile
The Connexx Hearing Profile already outperformed the standard workflow in a general comparison (Figure 8). All HCPs – regardless of their professional degree – experienced the Connexx Hearing Profile as more involving (Z=-7.644; p≤.001; Figure 8A) and indicated a better contribution of the patient to the fitting (Z=-3.534; p≤.001) compared to the standard workflow. Also, the HCPs perceived their patients as more motivated during the fitting with the Connexx Hearing Profile (Z=-3.024; p≤.01; Figure 8B).
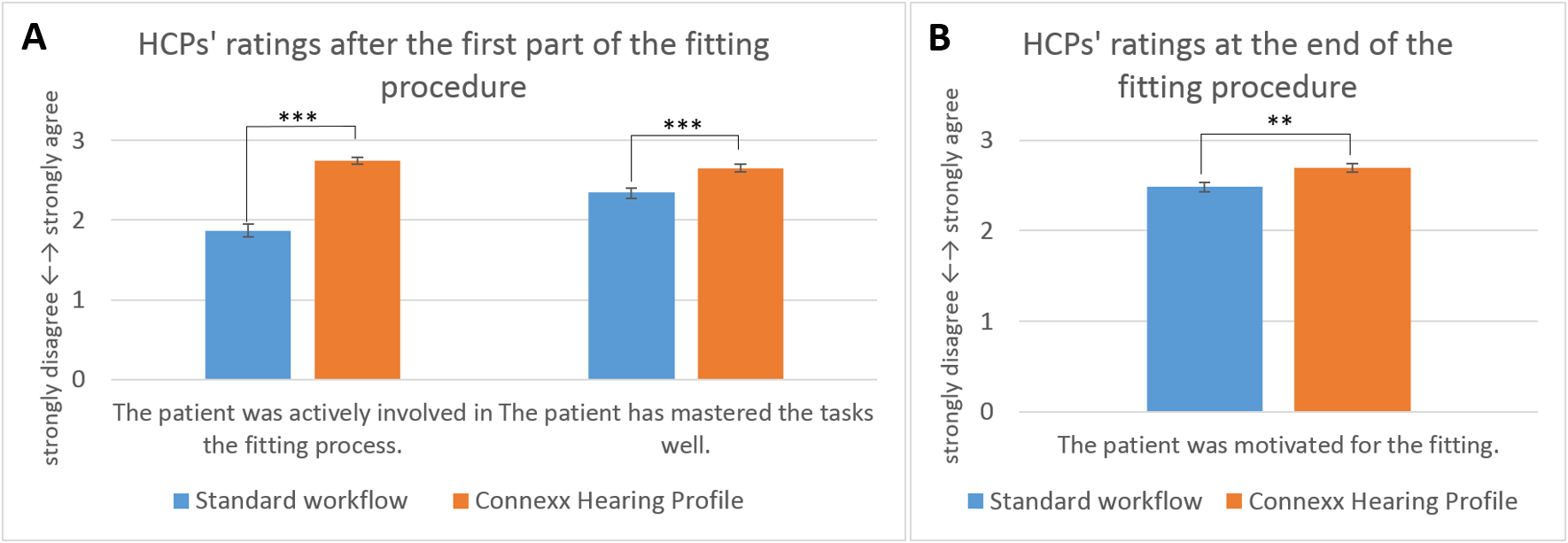
Figure 8. HCPs‘ ratings of the standard workflow (blue) and the Connexx Hearing Profile (orange). A ) HCPs‘ ratings regarding the patient during the fitting. Each patient was evaluated individually concerning the process. B) HCPs‘ assessments of the patient’s motivation. This evaluation took place at the end of the fitting procedure. Values are displayed as Mean±SEM.
The previously discussed results of the HCPs can be confirmed by the patients’ ratings. The patients who were fitted with the Connexx Hearing Profile felt more involved (Z=-7.384; p≤.001; Figure 9A) and received more interesting information (Z=-1.69; p=.091) than those who underwent the standard workflow. Additionally, the willingness to take home the hearing aids was higher for the Connexx Hearing Profile group (Z=-2.236; p≤.05; Figure 9B).
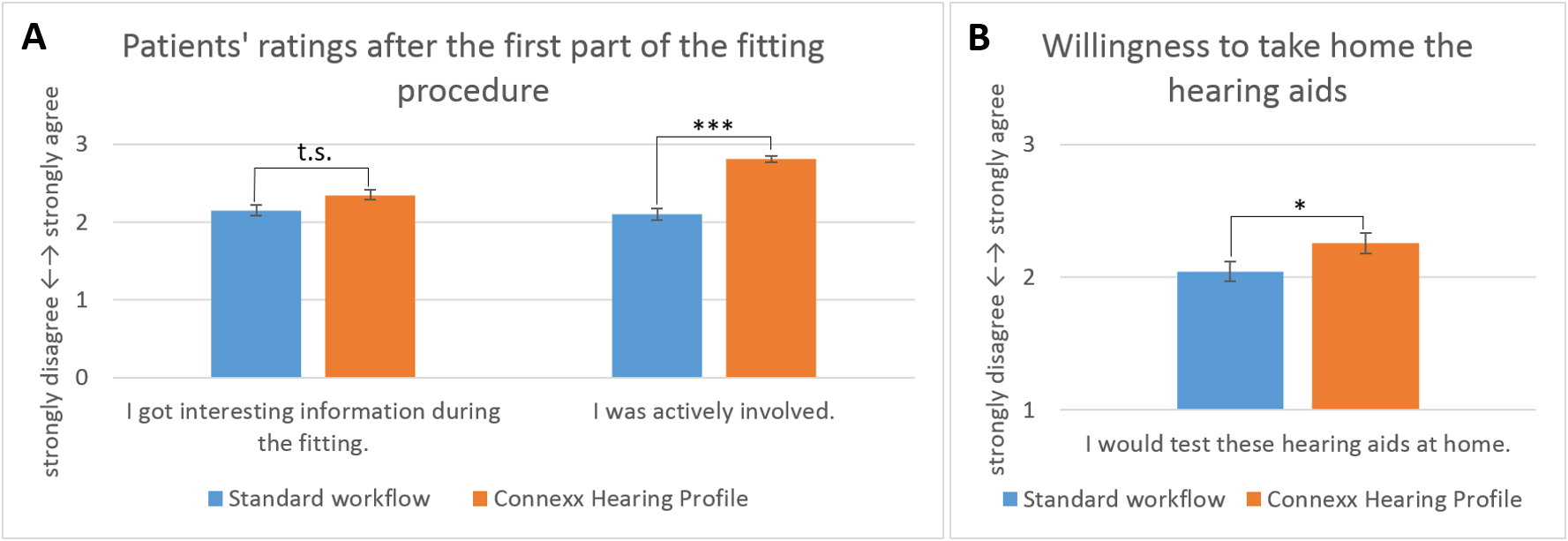
Figure 9. Patients‘ ratings of the standard workflow (blue) and the Connexx Hearing Profile (orange). A) Patients‘ ratings regarding the fitting process. B) Willingness to take home the fitted hearing aids after both fitting workflows. Values are displayed as Mean±SEM.
Impact of the HCPs’ Professional Degree
The previous results presented the general perception of the patients during the fitting. In the following section, we assessed whether these ratings were altered by the HCPs professional degree.
Whereas the audiologists‘ ratings did not differ between the standard workflow and the Connexx Hearing Profile, the HIS rated the patient’s contribution to the fitting (Z=-4.53; p≤.001; Figure 10A), motivation (Z=-4.24; p≤.001; Figure 10B) and the obtained information (Z= -5.219; p≤.001, Figure 10A) better in the Connexx Hearing Profile than in the standard process.
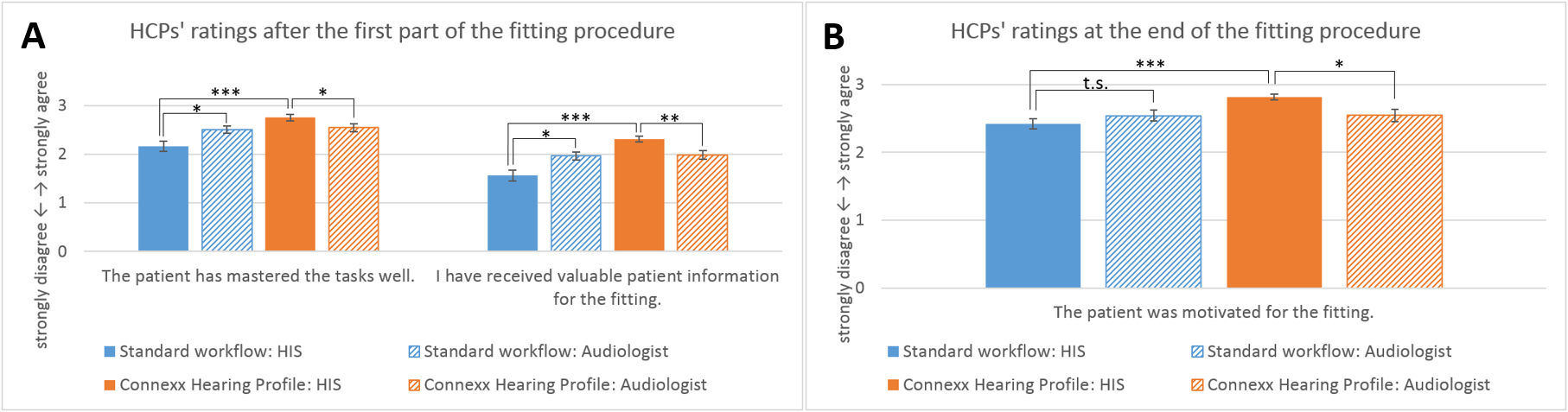
Figure 10. HCPs‘ ratings of the standard workflow (blue) and the Connexx Hearing Profile (orange) depending on the HCP’s professional degree. A) Individual rating of the patient and the fitting procedure. B Perceived patient’s motivation during the fitting procedure. Values are displayed as Mean±SEM.
When fitted by a HIS, also the patients using the Connexx Hearing Profile rated the received information as more interesting than the comparison group of the standard workflow (Z=-2.768; p≤.01; Figure 11A). These findings exceeded the ratings of the Connexx Hearing Profile’s patients fitted by audiologists (Z=-2.0; p≤.05). The HIS´ patients felt less involved in the standard workflow than the group fitted by audiologists as well (Z=-2.647, p≤.01). This effect did not occur in the Connexx Hearing Profile (Z=-0.99, p=n.s.). Moreover, the patients who were fitted by HIS with the Connexx Hearing Profile showed an increased willingness to take the hearing aids home in comparison to the group fitted with the standard workflow (Z=-2.256; p≤.05; Figure 11B). Therefore, the interaction between HCPs with entry-level education and their patients could, in particular, be improved using the Connexx Hearing Profile.
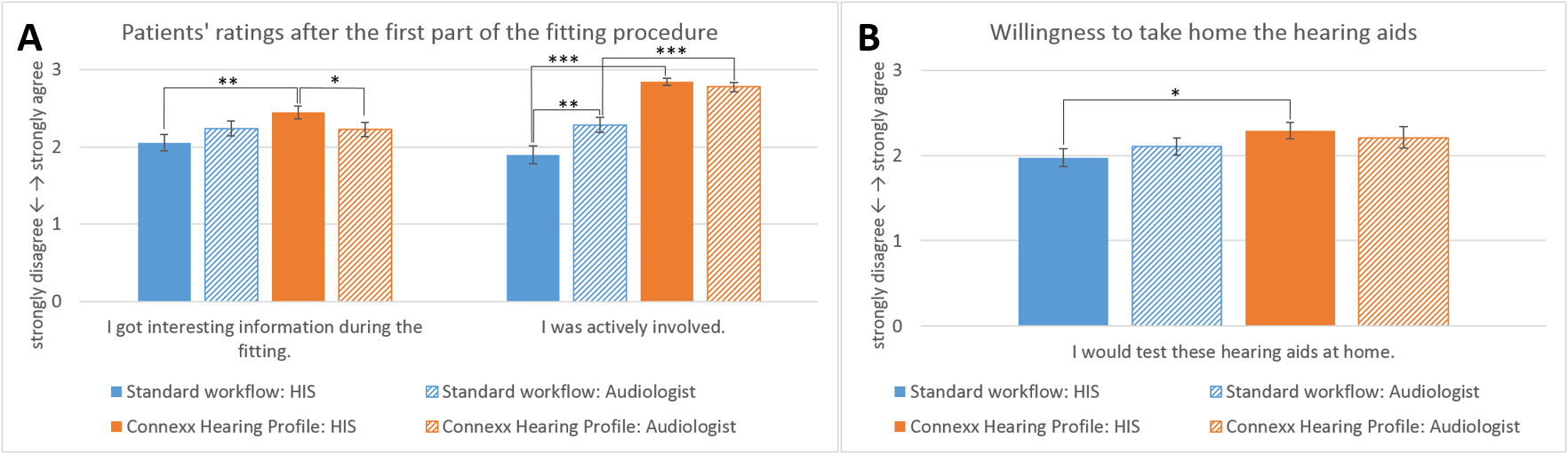
Figure 11. Patients‘ ratings of the standard workflow (blue) and the Connexx Hearing Profile (orange) depending on the HCP’s professional degree. A) Patients‘ ratings of the fitting procedure until the first fit. B) Patient’s willingness to take home the hearing aids. Values are displayed as Mean±SEM.
Benefit for Specific Patient Groups
So far, a general positive influence of the Connexx Hearing Profile on the patient has been observed. We questioned, however, whether the fitting with the Connexx Hearing Profile especially lends itself to a specific patient group (age, hearing aid experience, etc.).
The patients were divided into subgroups with respect to age and hearing aid experience via a median split across all study participants. In order to form two even groups, the central value of the distribution was set as a threshold.
The analysis elicited an interesting result (Figure 12): After a fitting with the standard process, patients with at least five years of hearing aid experience showed a decreasing willingness to take the devices home (Z=3.623; p≤.001; Figure 12B). On the contrary, after conduction of the Connexx Hearing Profile, the rating remained at the same high level as that of the patients with less than five years hearing aid experience (Z=-0.477; p=n.s.). Moreover, the work with the Connexx Hearing Profile resulted in an increased willingness to take the devices home for the more experienced patients (Z=-2.923, p≤.01).
The rating regarding the patients´ satisfaction provided by the HCPs trends in the same direction. After using the standard process, the satisfaction rating for the more experienced patients was worse than that of the less experienced group (Z=-2.414; p≤.05; Figure 12A). In contrast, when the Connexx Hearing Profile was used the satisfaction was equal for both groups (Z=-1.427; p=n.s.). The same was true for the HCPs’ rating, whether the patient could test the devices at home (standard process: Z=-2.992; p≤.01 |Connexx Hearing Profile: Z=-1.427; p=n.s.).
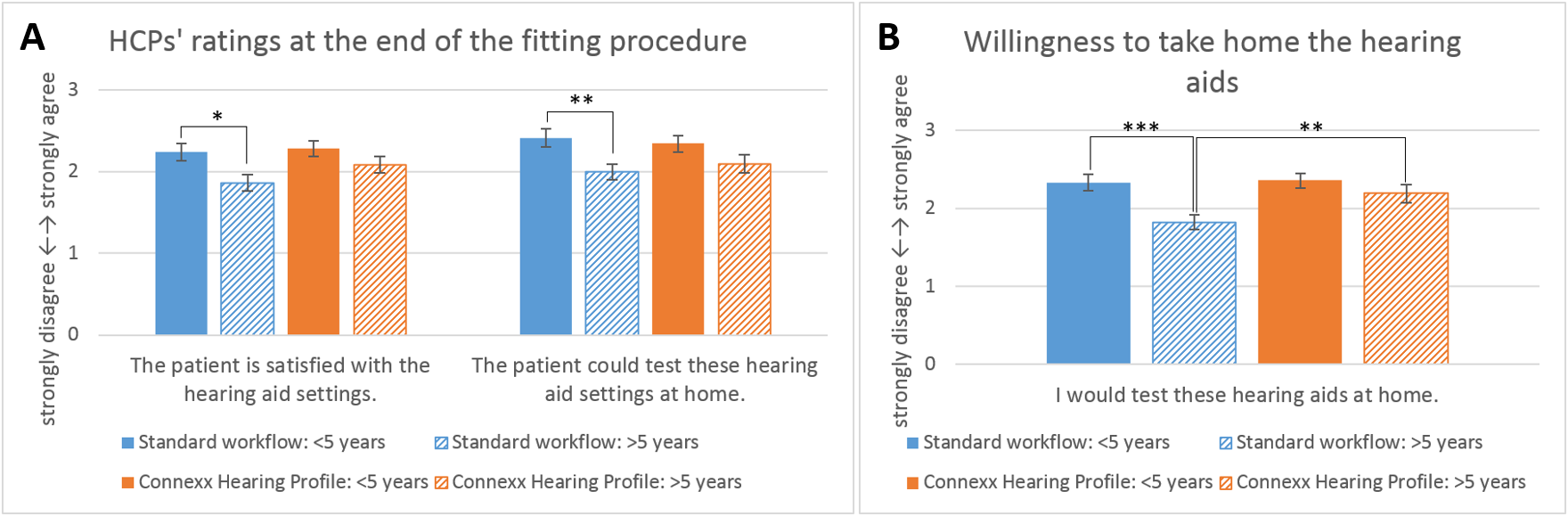
Figure 12. HCPs' and patients' ratings of both fitting workflows depending on the patient’s hearing aid experience. A) HCP’s individual assessment of the patient’s satisfaction with the hearing aid settings depending on the hearing aid experience. B) Patient’s willingness to take home the hearing aids depending on the hearing aid experience. Values are displayed as Mean±SEM.
The benefit of the Connexx Hearing Profile was also visible in regard to different age groups. In particular, the motivation for the fitting was maintained for older patients (>73 years). In the standard procedure, these patients were less motivated than the younger ones (Z=-2.171; p≤.05; Figure 13B), while in the Connexx Hearing Profile the motivation of the patients rated by the HCPs was the same (Z=-0.99; p=n.s.). The assessment of the patient’s contribution to the fitting showed a similar pattern. In the standard process, the older patients were perceived as less able to contribute to the fitting than the younger group (Z=-2.167; p≤.05; Figure 13A). In the Connexx Hearing Profile, however, the two groups were similar (Z=-0.971; p=n.s.) and the HCPs rated the contribution of their older patients significantly higher in the Connexx Hearing Profile than in the standard procedure (Z=-3.929, p≤.001). In addition, the HCPs found that they could retrieve valuable information for the fitting of older patients from Connexx Hearing Profile (Z= -2.963; p≤.01).
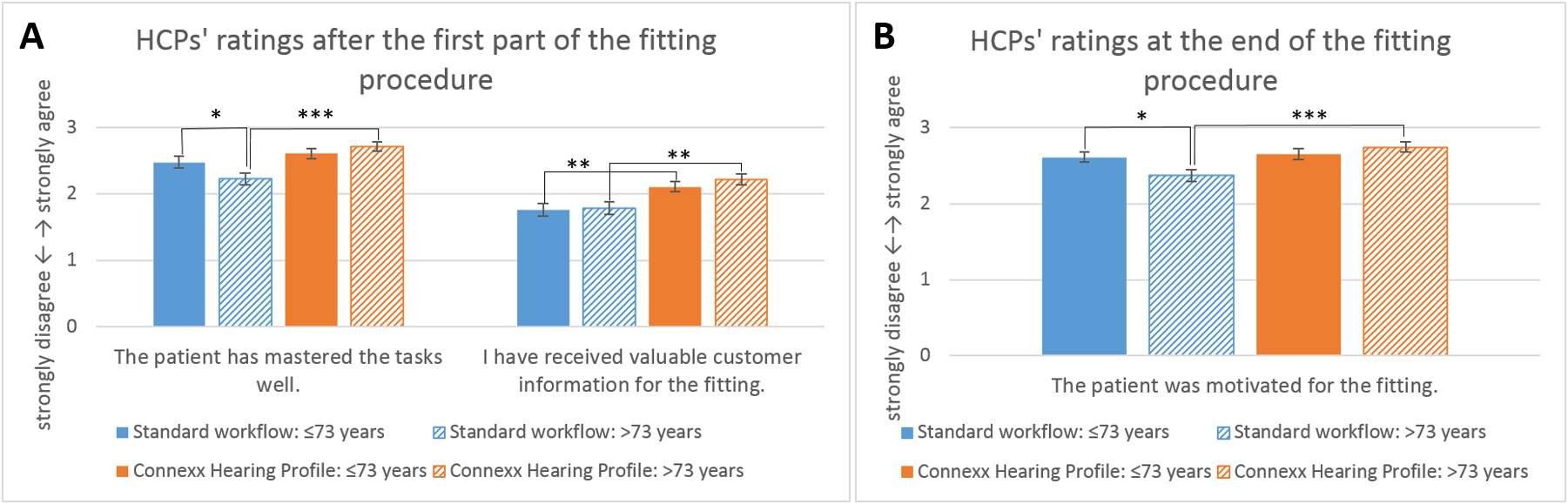
Figure 13. HCPs‘ ratings on their patients in both fitting workflows depending on the patient’s age. A) Individual rating on the patient and the fitting until the first fit. B) Perceived patient’s motivation. All values are displayed as Mean±SEM.
The same pattern was reflected in the patients´ ratings. In the standard procedure, the older patients found their tasks related to the fitting harder to solve than the younger ones (Z=-2.043; p≤.05; Figure 14). Such differences were not observed when using the Connexx Hearing Profile (Z=-0.098; p=n.s.). In addition, the older patients valued the information they retrieved from the Connexx Hearing Profile (Z=-2.158; p≤.05).
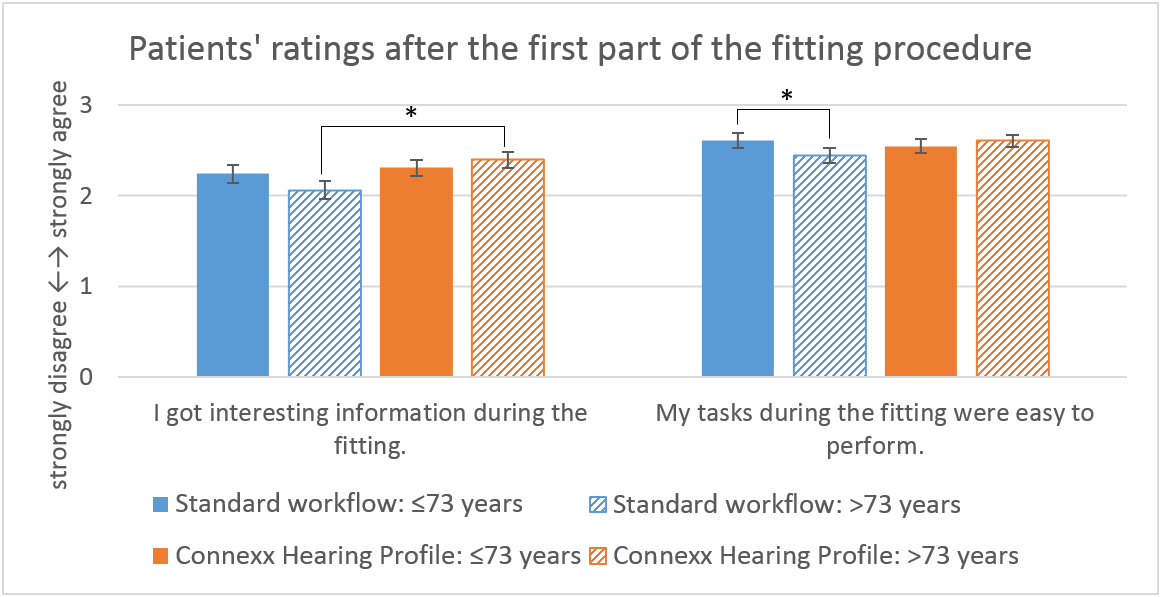
Figure 14. Patients‘ ratings of both fitting workflows depending on their age. Values are displayed as Mean±SEM.
In summary, the Connexx Hearing Profile offers the following advantages to the patient:
- Increased satisfaction and willingness to take the hearing aids home
- Valuable information on their hearing characteristics
- Software-supported communication tool for the patient to actively contribute to the fitting, special suitability for older and more experienced patients
- Increased motivation and satisfaction
- Raise of involvement and commitment to the fitting
Summary
The Connexx Hearing Profile provides numerous advantages for both patients and HCPs. The consideration and use of individual information on the hearing characteristics results in a selection of patient-specific first fit prescriptions. Serman, Fischer, Herbig, and Hannemann (2017) have already proven the benefit of this individualized fitting approach. In comparison to the standard procedure, the use of the Connexx Hearing Profile resulted in a 12 percent increase regarding acceptance rating for unsatisfied people. It could be shown as well, that listening effort was decreased, if the first fit was derived from the Connexx Hearing Profile (Serman, Fischer, Herbig, & Hannemann 2017).
Beyond this, the Connexx Hearing Profile leverages the fitting process. After extensive experience with both procedures, the HCPs found the gain prescription of the Connexx Hearing Profile was improved, without compromising the duration of the fitting process. Furthermore, the HCPs reported that using the Connexx Hearing Profile increased the patients´ acceptance in comparison to the standard process. The motivation of the patient during the fitting was positively influenced and the patients´ satisfaction was increased as well. In particular, hearing instrument specialists could incorporate the information provided by the Connexx Hearing Profile into their work, which then led to a decrease of fine tuning duration while the willingness to take the hearing aid devices home was increased. Finally, the comprehensibility of the Connexx Hearing Profile and the supportive effect to their work was positively perceived by all HCPs.
The Connexx Hearing Profile also serves as an appropriate means for improving the patients´ involvement in the fitting by actively providing individual information. In general, by the usage of the Connexx Hearing Profile, they retrieved interesting facts about their hearing characteristics, were motivated for the fitting process and the use of the hearing aid devices at home. Older and more experienced patients profited in particular from the Connexx Hearing Profile with respect to these effects.
Overall, in this real-world field study, the Connexx Hearing Profile was shown to be a valuable tool for HCPs, not only by providing an individualized first fit with an appropriate target prescription, but also a means to leverage the cooperation between HCP and patient which results in improved fitting success.
References
Bernstein, J., Mehraei, G., Shamma, S., Gallun, F., Theodoroff, S., & Leek, M. (2013). Spectrotemporal modulation sensitivity as a predictor of speech intelligibility for hearing impaired listeners. Journal of the American Academy of Audiology, 24(4), S. 293-306.
Dillon, H. (2001). Hearing Aids. Sydney: Boomerang Press.
Dubno, J., Dirks, D., & Morgan, D. (1984). Effects of age and mild hearing loss on speech recognition in noise. The Journal of the Acoustical Society of America, 76(1), S. 87-96.
Gordon-Salant, S. (2005). Hearing loss and aging: new research findings and clinical implications. Journal of Rehabilitation Research and Development, 42(4), S. 9.
Hopkins, K., & Moore, B. (2011). The effects of age and cochlear hearing loss on temporal fine structure sensitivity, frequency selectivity, and speech reception in noise. The Journal of the Acoustical Society of America, 130(1), S. 334-349.
Humes, L. (2002). Factors underlying the speech-recognition performance of elderly hearing aid wearers. Acoustical Society of America, S. 1112-1132.
Hutchinson, K., Duffy, T., & Kelly, L. (2005). How personality types correlate with hearing aid outcome measures. The Hearing Journal, 58(7), S. 28-30.
Lazarus, H., Sust, C. A., Steckel, R., Kulka, M., & Kurtz, P. (2007). Akustische Grundlagen sprachlicher Kommunikation. Springer-Verlag Berlin Heidelberg.
Lunner, T. (2003). Cognitive function in relation to hearing aid use. Int. J. Audiol. 42 (Suppl. 1), S. 49-58.
Lunner, T., & Sundevall-Thorén, E. (2007). Interactions between cognition, compression, and listening conditions: effects on speech-in-noise performance in a two-channel hearing aid. J. Am. Acad. Audiol. 18, S. 604-617.
Neher, T., & Wagener, K. (2016). Investigating differences in preferred noise reduction strength among hearing aid users. In: Trends in Hearing (Online), 20, S. 1-14.
Neher, T., Wagner, T., & Fischer, R.-L. (2015). Individuelle Anpassung von ein- und mehrkanaligen Algorithmen zur Störgeräuschreduktion in Hörgeräten. Tagungsband der 18. Jahrestagung der Deutschen Gesellschaft für Audiologie, Bochum.
Pichora-Fuller, M., Schneider, B., & Daneman, M. (1995). How young and old adults listen to and remember speech in noise. The Journal of the Acoustical Society of America, 97(1), S. 593-608.
Serman, M., Fischer, R.-L., Herbig, R., & Hannemann, R. (17. July 2017). Moving Beyond the Audiogram Towards a Patient-Centered, Interactive First Fit. Audiology Online.
Citation
Fischer, R., Schuelke, M., Hannemann, R., & Serman, M. (2018). Software-based hearing profile improves hearing aid fitting process. AudiologyOnline, Article 23716. Retrieved from https://www.audiologyonline.com




