
Introduction
Can trainable hearing aids be used with experienced hearing aid users? It is easy to understand the potential benefits for new hearing aid users, but won’t experienced users simply train the settings so that the new trainable hearing aids sound like their old hearing aids? We investigated this question and provided a summary of our findings in an AudiologyOnline Ask the Expert column (Mueller & Hornsby, 2014). Here are the full details. For a review of trainable hearing aids and their clinical applications, please refer to Mueller (2014).
Method
Participants
The test protocol was administered to 20 participants, 6 females and 14 males, between the age of 52 and 80 years (mean age 68.3 years). The G*Power 3 power analysis package was used for a priori calculations to estimate the required number of participants. Assuming that the results of the study would show a large effect (an effect size of f>0.4), it was estimated that a minimum of 17 participants were needed to reach statistical significance at the 0.05 level with power greater than 0.80.
All participants had bilateral sensorineural downward-sloping hearing loss and normal immittance. Hearing thresholds were no better than 15 dB at 500 Hz and no worse than 80 dB at 3000 Hz for either ear, with symmetry between ears within 20 dB for any given frequency. All participants were experienced users of bilateral hearing aids; regular use for at least two years.
Hearing Aids
The hearing aids used in this research were the Siemens Pure mini-BTE RIC instruments, fitted with closed dome earmolds. These products had 16-channel wide dynamic range compression (WDRC), and four-channel automatic gain control for output. All special features were active at default settings during the two week training period, which included low-level expansion, adaptive feedback reduction, and three different types of digital noise reduction (i.e., modulation-based, wiener filter and impulse-noise peak reduction). The hearing aids had compression training (i.e., input specific training for gain), and a treble control, which allowed for alteration of the frequency response.
Procedures
Initially, probe-microphone speech mapping measures were obtained for all participants for their personal hearing aids adjusted to their use-gain settings. The participants were then fitted bilaterally with the trainable instruments. The hearing aids were pre-programmed to the NAL-NL1 fitting algorithm contained in the Siemens CONNEXX software. Probe-microphone measures were then utilized to adjust and verify the hearing aid’s output based on the Audioscan Verifit derived NAL-NL1 earcanal SPL prescriptive targets using the real speech calibrated male talker (“carrot passage”) input signal of this equipment. Prescriptive targets were verified and recorded for three inputs: 55, 65 and 75 dB SPL.
Following the fitting and orientation, the participants were given training with the remote control which was used for making the adjustments during the two-week home trial. To encourage different listening experiences and possible instrument adjustments, they also were given a diary to complete, which included a variety of suggested listening situations and tasks. At the end of the two weeks of training, the participants returned to the clinic and their trained gain was measured. So we then had three sets of speech mapping data for three different input levels for analysis: the real-ear output for the NAL-NL1 prescription, the real-ear output for the trained gain, and the real-ear findings for their personal hearing aids. Recall that these instruments had compression training (not just overall gain), so training could be different for the different input levels.
Results and Discussion
An initial analysis was completed to confirm that match to target between the right and left ears were similar. A series of three factor repeated measures Analysis of Variance (ANOVA) were used to investigate symmetry between ears. The within subjects independent variables included test ear (right and left), input level (55, 65, and 75 dB) and frequency (250, 500, 1000, 2000, 3000, and 4000 Hz). The dependent variable was real ear level (in dB). Separate analyses comparing right and left ear values were completed on the actual NAL-NL1 targets and the aided real ear levels 1) following the initial match to target using the test hearing aids, 2) using the participants own hearing aids, and 3) using the test hearing aids following compression training.
In all comparisons no significant difference (p > 0.05) between ears for either target or measured levels was observed. Therefore levels between ears were averaged to create a single value representing bilateral levels at each frequency in each hearing aid test condition. In addition, to provide frequency information while simplifying the data analysis, frequency specific real ear levels were collapsed into a low- and high-frequency band. Real ear levels at 250 and 500 Hz were summed on a power basis to create a low frequency band level. The same process was completed using real ear levels at 1000, 2000 and 3000 Hz to create a high-frequency band level. All future analyses were completed using these bilateral, high- and low-frequency band levels. A summary of the real ear output for the different hearing aid conditions for this data grouping is shown in Figure 1.
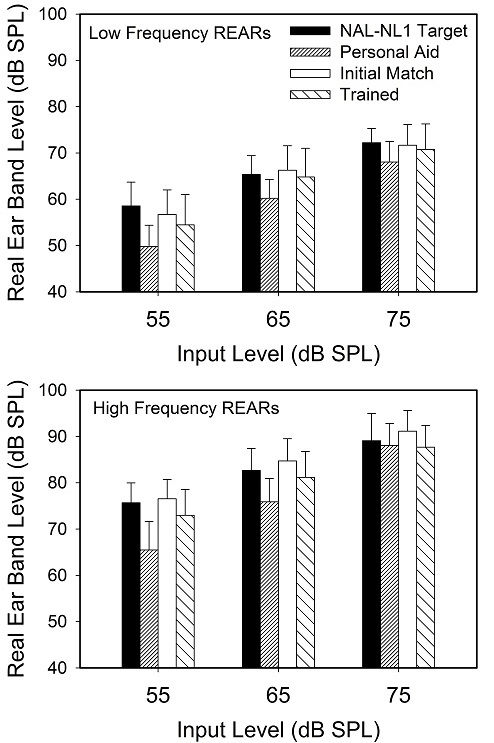
Figure 1. Mean real ear aided response (REAR; earcanal SPL) shown for the averaged low-band and high-band frequencies for the real- speech inputs for three levels. Data shown for four conditions: NAL-NL1 target, NAL-NL1 best match to target, trained gain, and average gain for the patient’s personal hearing aids.
Given the study focus, our initial analysis explored differences between hearing aid settings using a three-factor repeated measure ANOVA. NAL-NL1 target real ear levels and real ear levels obtained immediately after the initial fitting and following compression training were compared. The within subjects independent variables were hearing aid setting (NAL-NL1 target levels, initial fitting levels and Post-compression training levels), speech input level (55, 65, and 75 dB) and frequency region (low [250 and 500 Hz] and high [1000, 2000 and 3000 Hz]). The dependent variable was the target, or measured, level of amplified speech in the real ear (in dB). Due to violation of the ANOVA assumption of sphericity, a Greenhouse-Geisser correction was used when determining significance of test results.
The main effect of hearing aid setting was significant (F2,38 = 4.8, p = 0.035). In addition, all other main effects and two- and three-way interaction effects were also significant. Of particular interest in this study were potential differences between real ear levels, as a function of both frequency and level, across the different hearing aid settings. To explore these differences we conducted post-hoc pair-wise comparisons of NAL-NL1 target levels, initial fitting levels and compression trained levels for each combination of frequency (low- or high-frequency band) and speech input level (55, 65 and 75 dB). To reduce the likelihood of a type-1 error due to our multiple comparisons a Bonferoni correction was used. We were only interested in pair-wise comparisons made at each frequency/ speech level combination (i.e., differences between NAL-NL1, initial programmed values (best match to target) and compression trained values at a given frequency/speech level). Therefore the desired error rate of 0.05 was adjusted by our number of comparisons (3) in each condition resulting in a corrected p-value of p= 0.0167 (p=0.05/3).
Initial Fitting vs. Trained Gain
When comparing the initial fitting and compression trained levels a consistent difference was observed in the high-frequency band. Following compression training, real ear levels in the high-frequency bands were consistently reduced compared to the initial fitting (t= 3.5, 3.5, and 3.9; p = 0.002, 0.002, and 0.001 for the 55, 65 and 75 dB levels respectively). No difference between initial fitting levels and compression trained levels was observed in the low-frequency band. In summary pair-wise comparisons showed that, on average, compression training resulted in reduced high-frequency output for all speech input levels compared to our initial fitting levels (which were slightly higher than NAL-NL1 high-frequency targets). Following compression training levels were similar to, or slightly less than (for a 55 dB input), NAL-NL1 target levels.
Previous Use Gain vs. Trained Gain
Recall that our primary research question was whether experienced hearing aid users would train their hearing aids to match the current levels of their personal hearing aid. For example, if a person was under fit compared to NAL-NL1 targets with their personal hearing aids would they train their new hearing aids to result in a similar fitting? To test this hypothesis a three factor repeated measures ANOVA was used to compare real ear outputs, again in low- and high-frequency bands at three speech levels, for personal aids and participant’s compression trained settings. Of interest in this study were effects and interactions related to differences in hearing aid settings. The ANOVA results showed a significant main effect of hearing aid setting (F1,19 = 17.7, p <0.001). When averaged across level and frequency region real ear levels were significantly lower with the participant’s own hearing aids compared to levels obtained after compression training. A significant two way interaction between hearing aid setting and speech level (F2,38 = 33.65, p <0.001), suggested that differences between aid settings were largest at lower speech input levels and decreased as speech levels increased. Finally, a significant and three way interaction (F2,38 = 27.68, p <0.001) was also observed. Follow up testing of differences between hearing aid settings were conducted using a series of pair-wise comparisons of at each combination of frequency (low- or high-frequency band) and speech input level (55, 65 and 75 dB). Given only a single a priori planned comparison was made in each test condition no correction for Type 1 error was used. Results revealed significantly (p<0.05) lower levels for the personal aids except for the high-frequency band at a 75 dB input level (t=0.37, p=0.71). See Figure 2.
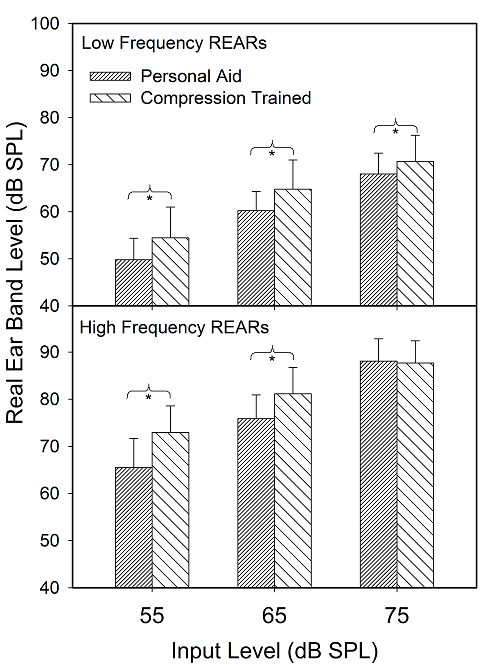
Figure 2. Average real ear levels, as a function of low- and high-frequency band and speech input level, for the participant’s personal hearing aids and the output following training. Asterisks show significant differences between Personal and Trained REARs in a given condition.
Influence of Previous Use Gain?
As shown in Figure 2, on average, participants do not necessarily train their new hearing aids to match previous hearing aid settings. However, it is still possible that previous use gain influenced the direction of training. For example, individuals with personal aids set below NAL-NL1 targets may have tended to adjust the gain on their new hearing aids down as well, even if the final gain settings were not matched. To examine this question we completed a series of correlation analyses on deviations from NAL-NL1 target levels for each individual’s personal hearing aid and their real ear levels following compression training. Scatter plots showing these relationships are shown in Figure 3.
Data points falling below the solid diagonal line in Figure 3 reflect real ear levels that are greater following compression training than with the individual’s personal aid. Data points greater than zero suggest real ear levels higher than NAL-NL1 targets. It is interesting to note that personal hearing aids with real ear levels greater than zero (higher than NAL-NL1 targets) were relatively uncommon, except for the 75 dB speech level in the high-frequency band. Our results revealed positive correlations between deviations from NAL-NL1 targets with personal hearing aids and compression trained aids. In other words, there was a tendency for individuals to deviate from NAL-NL1 targets in the same direction (i.e., above or below target) whether using their personal aid or the compression trained aid. This was particularly true when an individual’s use gain levels were substantially less than NAL-NL1 targets (i.e., negative deviations). Individuals with personal use gains closer to NAL-NL1 targets (i.e., deviations near zero) were more likely to train their hearing aids to levels higher than their previous use gain.
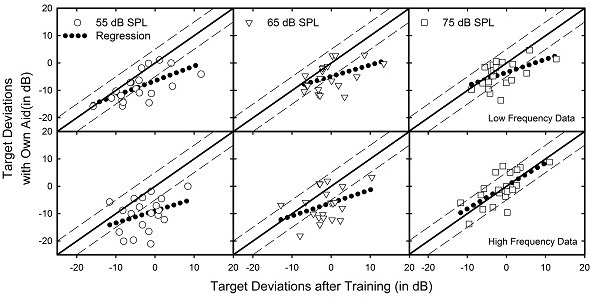
Figure 3. Scatterplot showing deviation from NAL-NL1 targets following compression training (x-axis) and with each participant’s own personal hearing aid (y-axis). Deviations falling on the solid line are the same. The dashed lines capture deviations that are ±5dB of each other. The dotted line shows a linear regression of the deviations. The upper and lower panels show deviations from low- and high-frequency band level targets, respectively. Circles, triangles and squares represent deviations at 55, 65 and 75 dB SPL speech input levels, respectively.
Comments
All the participants in this study had been fitted at the same University clinic; historically the protocol at this site was to use the manufacturer’s proprietary fitting and a patient-driven approach for post-fitting adjustments. We were not surprised, therefore, that the participants’ use gain going into the study was significantly lower than prescriptive target gain, especially for soft inputs. Had the participants all been initially fitted to NAL prescriptive gain, our comparisons would have been less interesting. But recall, a requirement for recruitment into the study was that the hearing aid users were satisfied with their current fittings. Yet, following training, on average they were using approximately 5-10 dB more gain than with their personal hearing aids for soft and conversational speech levels; 55% of the participants were using 10 dB or more than previously for the 55 dB SPL speech input.
While we did not conduct a specific measure of post-training satisfaction, it seems that if this increased audibility of soft sounds had not been okay, the participants would have reduced gain, which would have been reflected in the final trained-gain levels. If we forget about their previous use gain for a moment, the fact that their trained gain for soft inputs was similar to NAL targets is not surprising, as this has been the general finding in other research with trainable hearing aids, such as that conducted by Catherine Palmer, PhD, at the University of Pittsburgh, and the research group at the National Acoustic Laboratories of Australia.
One factor that could have influenced the outcome of this study is that maybe many of the participants simply didn’t train their hearing aids? If so, we then would be left with trained gain similar to the NAL, which was the starting point. We don’t believe this had a significant impact, for several reasons. First, the participants had a diary to complete, which included a variety of listening situations that potentially would encourage gain adjustments. Through data logging, we also could monitor the number of gain changes during the two-week period; all had at least 130 adjustments. Finally, if we examine individual data (see Figure 3; Y-axis) we see that about 50% of the participants had training of +/- 3 dB for both the 55 and 65 dB input levels.
Finally, it’s very possible that our outcome was influenced by initially fitting the participants to the NAL-NL1—the starting point for training does matter (Mueller, Hornsby, & Weber, 2008; Mueller & Ricketts, 2014). Had we initially fit them to their previous use gain, we doubt that they would have trained up to the NAL levels. This points out the potential risk involved in clinical practice, when patients are under fit, and the audiologist assumes that these patients will gradually ease into more appropriate gain. As illustrated in Figure 3, the majority of these participants, who began the study as happy hearing aid users, concluded training using significant more gain for soft sounds than what they previously had been using. This seems like a good thing.
References
Mueller, H.G., & Hornsby, B.W.Y. (2014, July). Can trainable hearing aids be used with experienced hearing aid users? AudiologyOnline, Ask the Expert 12765. Retrieved from: https://www.
Mueller, H.G. (2014, July). Siemens Expert Series: Trainable hearing aids - Friend or foe for the clinician? AudiologyOnline, Article 12774. Retrieved from: https://www.audiologyonline.com
Mueller, H. G., Hornsby, B., & Weber, J. (2008). Preferred hearing aid gain using trainable hearing aids. Journal of the American Academy of Audiology, 19(10), 758-773.
Ricketts, T.A., & Mueller, H.G. (2014, March). When is the best time to activate the 'training' feature in hearing aids? AudiologyOnline, Ask the Expert 12350. Retrieved from https://www.audiologyonline.com
Cite this content as:
Mueller, H.G., & Hornsby, B.W.Y. (2014, July). Trainable hearing aids: the influence of previous use-gain. AudiologyOnline, Article 12764. Retrieved from: https://www.audiologyonline.com


