
Thank you for joining us today for our HOPE online series. As a matter of disclaimer, I am going be talking about a number of devices that Cochlear does not manufacture or distribute, because the purpose of this presentation is to show the landscape of what is available for patients with single-sided deafness (SSD). This is information that I have gained from the public domain as a student of this particular segment of audiology and hearing rehabilitation.
SSD is defined as a condition where an individual has non-functional hearing in one ear and receives no clinical benefit from amplification in that ear, with the contralateral ear possessing normal audiometric function. We define normal audiometric function as hearing thresholds that are no poorer than 20 dB hearing level (HL) for pure-tone averages of .5, 1, 2, and 3 kHz. The non-functional ear can be, but is not limited to, a profound hearing loss. The key factor is that the poor or "bad" ear has not or will not receive benefit when traditional acoustic amplification is applied. The "good" ear must have a pure-tone average that is 20 dB or better across the pure-tone range.
SSD can be defined relative to a bone-conduction device such as Baha. The use of a Baha device for SSD is intended to improve speech recognition. SSD is an indication for a Baha for patients who suffer from unilateral sensorineural deafness on one ear, while the other ear has normal hearing of no worse than 20 dB.
Over the evolution of this product, and because of changes in classification for reimbursement purposes, we no longer refer to a Baha as a hearing aid; we refer to it as an auditory osseointegrated implant system. Before SSD was a recognized term, we lived with the description of unilateral sensorineural hearing loss, and it was usually in the profound category. The term single-sided deafness was actually coined by the predecessor company, Entific, when they started offering Baha for SSD. It has become very widely used in the industry to describe the condition of a complete sensorineural hearing loss in one ear. We use this specific term to differentiate that from someone who may have a conductive loss in one ear, as you would see in a patient with atresia or microtia. These patients typically have good cochlear function. People with SSD actually have such damage to the inner ear that traditional amplification does not provide them any benefit.
Spatial Hearing
We wanted to identify the types of problems that are created with a hearing loss of this type and configuration. First, you lose the ability to have spatial hearing, or what we traditionally think of as localization in the horizontal plane. Our two-eared auditory system is precisely oriented for using specific cues that allow us to localize sound, and we use a two-ear input system to make that happen. When one ear is taken out of the equation, it creates some confusion within the brain. We also have the addition of the head-shadow effect, which is where the non-functional ear is in the acoustic shadow of the good ear on the opposite side of the head. What ends up happening is a cumulative effect. This presents difficulty with speech intelligibility in the presence of background noise, and it is oftentimes the most prevalent when the speech target is presented at the dead ear and the signal has to cross over the head and be heard by the only hearing ear on the opposite side. It creates communication problems, and it also creates a decrement in quality of life and quality of listening.
Spatial hearing, or having two ears, is very important to us. It is one of the more qualitative features of the auditory system that allows us to be able to identify both near and distant sounds, as well as those that occur 360 degrees around our head. What we understand about spatial hearing is that there are some features we use when we have a normal functioning two-channel system.
We utilize several different attributes to allow us to have spatial hearing. One of them is the interaural time difference. That is typically a lower-frequency phenomenon. The way the auditory system and brainstem are wired allows the two ears to be compared against one another. Small differences in time in the lower-frequency domain can be measured. Typically, if the sound is coming from the left side of the head, it will actually stimulate the left ear just a few microseconds ahead of the right side, and those timing differences can be decoded in a normal-hearing scenario where two ears are involved. This is, again, predominantly a low-frequency phenomenon.
When we look at frequencies above 1600 Hz, we also deal with interaural level differences. This is a scenario where the sound is slightly louder on the side on which it is presented. The intricate connections in the auditory brainstem and lower auditory system give the brain information about where sound comes from. We call that the interaural level difference.
The last one is the spectral distance, and this has to do with the fact that there are spectral differences that occur when sound is present from one side or the other. These three attributes allow us to have spatial hearing. You can imagine that if you lose one of your channels, or ears, and you have no input, this precise system gets thrown off. It does not completely destroy all of the cues, but it modifies them in a way that creates some confusion.
The loss of spatial hearing is usually the motivating factor that moves a patient forward to treatment of SSD. It is not the only factor, but it is probably one that is recognized most often both by patients and audiologists. These individuals also report a loss of balance between the two ears, and they lose the ability to have stereo hearing. The loss of spatial hearing not only heightens communication concerns, but it also creates safety concerns. If you have a completely impaired ear on one side with inherent auditory confusions, you are at more risk, for example, as a pedestrian stepping into a street in front of a car or a bus that you might not hear. These are real issues that impact one's quality of life every day.
We do not routinely evaluate spatial hearing. When you think about the types of hearing evaluations we currently provide, we rarely evaluate how a patient hears in the spatial hearing domain, but it is a very important aspect and one that we take largely for granted. Spatial hearing is not equal to localization, but I would say that localization is a component of spatial hearing. We are going to talk about what to expect when we are doing these various treatments for individuals with complete loss in one ear.
Head-Shadow Effect
The head-shadow effect is one of the major mechanisms that is widely studied and understood, and with the loss of auditory function in this unilateral configuration, sounds that originate from the side of the non-functioning ear will actually fall in the shadow of the head. Low-frequency sounds, because of their long wavelength, bend very readily around the head and are largely unaffected, so the head is more or less transparent to the lower-frequency sounds that might be present (Figure 1). The higher-frequency sounds with shorter wavelengths tend to be reflected by the head in that shadow, and they get attenuated, which creates difficulty in audibility and clarity. When one considers that consonant sounds, which contain much of the meaning of English speech, occur in the higher-frequency domain, the head-shadow effect can be the root cause for the difficulty of communication, especially as it relates to speech understanding in the presence of background noise.
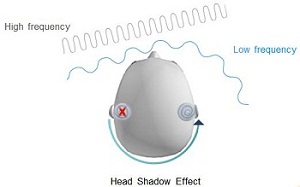
Figure 1. Head-shadow effect with low frequencies bending around the head and high frequencies deflected due to their short wavelength.
There is a combination effect of spatial hearing and the head-shadow effect that create a third problem of hearing in the presence of background noise. This is likely the other key factor that motivates one to seek treatment when they have an acquired sensorineural hearing loss on one side. Speech recognition in noise is also confounded by the lack of binaural summation. We have an incredible ability to hear in the presence of background noise when we have two ears and the full capacity of the central auditory system. However, when we have a unilateral loss in one ear, we lose the summation effect, which creates an additional confounding factor. The use of any kind of CROS (contralateral routing of signal) amplification system generally will have no helping influence on the binaural summation effect. It is a very challenging scenario that we deal with.
Causes of Single-Sided Deafness
This discussion will not be an exhaustive list by any means, but one of the known causes of SSD is the presence of an acoustic neuroma or a space-occupying lesion in the cerebellopontine angle. Typically, these types of tumors are benign and slow growing, but the surgical removal can significantly modify or damage the auditory nerve to the point where the patient has no useable hearing on that ear. It is quite important that these space occupying lesions be removed so that they do not create other types of health problems, but the side effect of treatment is often SSD.
The second cause of SSD is what we call sudden idiopathic hearing loss. This type of loss is usually due to viral infection, but is sometimes unexplained. This sudden loss is usually an inflammatory process that occurs in the cochlea. The virus infects the cochlea and causes localized swelling, and it culminates in permanent damage to the hair cells and the fine structures of the cochlea. In many instances, the ear does not recover and the patient is left without any hearing in one ear.
Blunt trauma to the head might create a transverse fracture of the temporal bone, and that renders the cochlea completely inoperable at that point in time. Unilateral vascular insults can occur to the vascular structures in the brainstem or the cochlea that damage the auditory pathway and leave one ear completely damaged. Meniere's disease is another process where excess fluid pressure in the ear causes long-term damage to the cochlea and renders the ear non-functional. There can also be congenital or genetic loss of hearing in a unilateral presentation. We know from early intervention and early screening programs that there are children born with profound unilateral loss and perfectly normal hearing in the other ear.
Solutions for Single-Sided Deafness
We have come to a point in technology where we have viable solutions for SSD. Unfortunately, the "do-nothing" solution is what is offered to a number of people. There is a fairly cavalier attitude often presented that if you have one functional ear, you should move through life and learn to live with the fact that the other ear is not going to contribute much. Believe it or not, that is exactly what some patients with SSD do, and some of them never miss a step as a result of that, but others are not so fortunate.
The first option we can offer for SSD is a CROS. In a CROS configuration, a microphone is been placed on the dead ear, and the signal that is picked up by the microphone is routed to an amplifying system with an open-tube fit on the good side. In this particular arrangement, we are able to contralaterally route the sound that is heard at the dead ear over to the good ear.
The CROS design was originally described by Harford and Barry in 1965 in the Journal of Speech and Hearing Disorders. The early devices were the eyeglass CROS hearing aids that were prevalent in the 1960s. They were able to build most of the electronics into the temple piece of the eyeglasses and use ear molds or open-tube fittings to allow for the signal to cross over. The wires that carried the connection from the microphone to the amplifier were hidden in the frames. They were even fitting these on individuals who did not have actual vision loss. Instead, they used plain glass over prescriptive lenses to be able to conceal the hearing aid and make this a more cosmetic scenario.
We have now moved from a CROS scenario that requires hardwiring to something like the Phonak CROS system that uses the Audeo SMART case, which is a mini BTE. This particular wireless CROS configuration uses advanced streaming technology to route the signal from one side of the head to the other. It can actually be built into an in-the-ear product, as well as a behind-the-ear product. We have indeed come a long way. The early CROS devices were hardwired devices, and you can imagine there was some cosmetic pushback from some patients who did not want to have that type of solution.
Another company that offers a wireless CROS configuration is Audifon, which is a German-based company. The Audifon via product also uses real-time audio streaming transmission, which provides a broadband signal to cross the head. Again, this represents a tremendous improvement over what has been traditionally available in CROS hearing aids.
There is now another way to accomplish the CROS scenario using what is called transcranial CROS. This design uses a completely-in-the-canal (CIC) power hearing aid. This was first described in the early 1990s where an acoustic CIC hearing aid was fitted to the poor or dead ear, and the sound pressure in the residual volume was loud enough to allow osseotympanic transmission of sound to cross from the bone of the dead ear to the cochlea on the contralateral side. The poor or dead ear must be able to handle the high level of sound pressure without any tolerance or recruitment issues. This was not a good treatment option, however, for patients who did not have a completely dead ear on that side. The transcranial CROS is a highly-cosmetic solution, as the nearly invisible CICs fit deep within the ear canal. There are still clinicians that use this technology, and the results vary from patient to patient.
Bone-Conduction Solutions
Now we are going to move into a discussion about how we use bone-conduction solutions to accomplish that contralateral routing of signal. In Figure 2, you can see that a Baha or bone-anchored product has been fitted behind the ear on the dead side, which creates the opportunity for the patient to have the signal routed through the bones in the skull to the functioning cochlea on the opposite side. We use these bone solutions much in the same way, but we use this pathway of bone conduction.
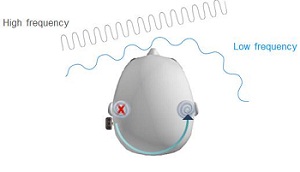
Figure 2. Bone-anchored solution to contralaterally route the signal via bone conduction to the opposite cochlea.
The very first reference to bone-conduction hearing enhancement devices came from the 1790s. A physician named Paledino in Italy developed the Fonifero, which is largely a metal rod with a stirrup. If we place the stirrup over the speaker's larynx and speak to the patient, we can transmit the raw vibration from the laryngeal output through that rod and place it either on the patient's teeth or on the bone behind their ear, which could create a bone conduction pathway. There were obvious limitations to this technology, but it was sophisticated for the 1790s.
We fast-forward now into the modern electronic age of bone-conduction oscillators. The traditional oscillator is largely an electromechanical device that allows for a coil to stimulate a magnet core. When you apply an alternating current to the electromagnet, an up-and-down movement of the armature in the center creates the vibration which then can be transmitted through the skin and into the bone to create this bone conduction pathway. This particular device was instrumental in creating bone-conduction hearing aids in the electronic age.
A traditional bone-conduction hearing aid is made by simply taking an air-conduction hearing aid and modifying the aid to drive a bone conduction oscillator attached to a headband. This arrangement worked quite well. The problem with this is that the steel headband that you have to wear is not comfortable for all-day or long-term use. It can take some adjustment to get used to and is not the most cosmetically acceptable option, but it is still used today in some situations. Many people were not using this device for SSD due to the amount of complexity and the discomfort.
Following these developments, there was the opportunity to access the bone conduction pathway in a device called the TransEAR. The TransEAR uses a behind-the-ear hearing aid, but what is attached to the other end is not an acoustic ear mold; it is actually a solid lucite earpiece that encases a bone-conduction vibrator. The in-the-ear piece is quite long. If you think back to the anatomical features of the external ear and the ear canal, the medial one-third of that canal is a bony canal. If you are able to get the ear mold seated into the second bend of the ear canal so that the tip of this ear mold is in contact with the bony ear canal, you can produce bone conduction signals through the TransEAR earpiece. You can stimulate the pathway through the skull and transfer the sound to the opposite side. This is an option for people with SSD that do not wish to have surgery. There are some limiting factors in terms of the size of the ear canal and the comfort, but overall, this product has had some success and is certainly an option for individuals who are considering treatment for SSD.
A new device that you may have heard about is called the SoundBite by Sonitus Medical in California. This is a device worn in the mouth with the external receiver worn on the outer ear. It has a retainer-looking device that has within it a bone conduction oscillator and a receiver stimulator package with an internal battery. This is worn in the mouth and snaps on the back of the molars. The behind-the-ear receiver is a microphone and a transmitter that is fitted to the deaf ear. The microphone is down in the ear canal to utilize the pinna cues. These two devices communicate by a proprietary radio frequency interface and allow for the sound to be transmitted and then amplified.
This is a relatively new device. We do not know a lot about it, other than the fact that it has obtained FDA clearance, and it is now commercially available. It operates in the very same way as other bone-conduction hearing aids, with the bone-conduction pathway including the teeth instead of the mastoid bone. That bone pathway allows the good ear, on the opposite side of the deaf ear, to be stimulated. This is another product that does not require a surgical intervention, but it does require a dentist to fit and take the dental impression and an audiologist to fit the actual hearing instrument.
Bone-Anchored Solutions
Bone-anchored solutions is the topic that is near and dear to my heart, because this is what I work with every day. I will give you an overview of what is available in this arena, as well. One of the devices current to the industry is marketed by the Sophono Corporation of Boulder, Colorado. This company was originally founded in Germany and has now manufactured in the United States. The implant package uses small, rare-earth magnets encased in a titanium carrier that are implanted underneath the skin. The sound processor is a device similar to a hearing aid, in that it is picking up sound and creating a vibrational signal. There is actually a magnetic plate attached to the back of the processor, and the transmission of sound across the skin barrier is what we call "transcutaneous pathway."
This device is actually a bone-anchored device, in that the magnetic implant is anchored under the skin, but there is nothing protruding through the skin. The two magnets attach on either side of the skin barrier, and the sound communicates across that transcutaneous barrier and, again, stimulates the bones in the skull. The option is to transmit sound to the ear opposite the deaf ear, so that there can be some cross-hearing or contralateral routing of signal.
Oticon Medical is a company that has developed a bone-anchored solution. Their newest sound processor is the Ponto Pro. This system is a percutaneous configuration, because there is a small metal snap that fits through the skin, and then there is the implanted component that is in the skull. This is a relatively new company to this particular treatment.
Of course, Cochlear has been involved for a long time with the Baha System. Figure 3 is a picture of the Cochlear system. There is an implant and an abutment that protrudes through the skin. That abutment allows for the processor to be attached and transmit sound directly into the bone by bone conduction.

Figure 3. Cochlear Baha 3 system.
The Baha System, as it relates to Cochlear's involvement, has been around since 1977 when it was first introduced into the European market. It was the first implantable hearing system that worked by virtue of what we call "direct bone conduction." The Sophono device mentioned earlier does not access a direct pathway, because the sound has to travel through the skin, but the implanted Baha allows for the sound to go directly to the bone. The sound is conducted to the skull bone, bypassing the outer and middle ear, and it stimulates the cochlear in that fashion.
From a historical perspective, the original work on Baha was completed in Sweden. The underlying property of osseointegration was identified by Professor Branemark, who discovered that titanium, if implanted in bone and left undisturbed, formed an initial bond with the bone which would strengthen over time. Dr. Branemark coined the term "osseointegration." He was also involved with dental implants, so he knew quite a bit about biomaterials technology. The Baha technology was originally developed for oral implant retention, but it very rapidly progressed to an ability to affix craniofacial prosthetics and other types of anchoring systems.
In the late 1970s, Dr. Branemark partnered with Dr. Anders Tjellstrom and some engineers at Chalmers University to develop the Baha System and commercialize it in 1977. What makes it unique is that it is a surgical procedure, but it allows for a direct bone-conduction pathway, and it makes a very stable, long-term and predictable success story. Figure 4 is the surface of a Baha implant where osteocytes are growing to the implant, and over time this becomes one with the bone. This process creates an important pathway that we call direct bone conduction.

Figure 4. Ostecytes growing on the titanium implant, or the process known as osseointegration.
This works independent of the ear canal and allows for direct transmission. It gives a very clear and natural sound. The other nice thing about these types of devices is that preoperative testing can be done, and the patients have a high wearing comfort. We do not have these spring steel headbands. In fact, the surgery for placing a Baha is very straightforward and safe and has shown a 30-year history of predictable outcome. So, for bone-anchored solutions that have percutaneous connections, Cochlear and Oticon Medical are the two available solutions.
The Food and Drug Administration (FDA) must approve devices for use in the United States. Many of these devices are scrutinized by the FDA because of the surgery involved, and they are cleared at the level of a 510(k). Remember that the original Baha device was available in 1977. It was not until 1995, however, that the device actually obtained clearance to treat mixed and conductive hearing losses. The breakout year for Baha was in 2002 when the FDA gave clearance to the Baha System for use in SSD. In that same year, we introduced a softband that allowed us to treat children under the age of five. Since that time, we have also added digital signal processors and improved the technology along the way. This has been an evolving technology. There are many people who are surprised to know that we have a 30-year history, and that it is a proven treatment option.
Win-Lose Scenarios for Baha
There are a few win-lose scenarios when talking about Baha and SSD, but they could be relative to any type of CROS scenario. Figure 5 is an illustration of a person who has a Baha on their left ear and a good-hearing ear on the right. You will notice that speech is being presented to the side where there is a Baha mounted. Noise is being presented from the front. This particular situation is what we call that the "win" situation, because the performance of the Baha is much better when the speech is the primary signal on the side where the Baha microphone is located.
The "lose" scenario is where speech is in front of the patient, and noise is presented predominantly to the Baha side. This means that the microphone picks up the noise and crosses it over to the better-hearing ear. If we use a full-bandwidth signal and do not roll off low-frequency energy, when patients get in this situation they have more difficulty and perform worse with the Baha. Sometimes patients learn a very valuable lesson when noise is the predominant signal on their Baha side. Rather than increasing the volume of the Baha, reducing the volume often improve their ability to hear speech instead. Keep in mind that this is true of all CROS technologies, because a microphone still picks up a signal at the poorer ear and transmits it to the opposite side. Again, the potential for optimal benefit is when speech is present at the microphone of the processor.
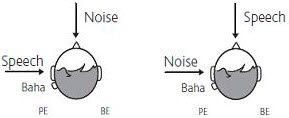
Figure 5. Win-lose scenario for Baha placement; speech at the processor and noise from the front is the best scenario while noise at the processor and speech from the front is the worst-case scenario.
Indication Criteria
Indications for the Cochlear Baha or the Oticon Medical Ponto system stipulate that the patient needs to be at least five years of age for implantation with normal hearing in the contralateral ear. We define "normal hearing" as thresholds no poorer than 20 dB for .5, 1, 2, and 3 kHz. Nowhere in this description does it describe what the level of hearing loss has to be in the poor ear, but it does state that the bone-anchored solutions function via transcranial routing of signal. Children under the age of five can use Baha on a Softband until they reach the appropriate age for implantation. The reason we do not typically implant children under the age of five is because of the immature structure of the bone and the fact that osseointegration may not take place in the same time frame as it would in adult bone.
What do we try to accomplish with bone-anchored solutions from a SSD perspective? We try to provide sufficient amplification to overcome the head transfer function. That is the ability to get the sound across the skull. The additional force that available in the sound processor may be required to overcome a larger head transfer function. The unknown for many patients is the fact that their head may be more or less dense, and if there is any hearing loss that is acquired after implantation due to aging, there is the potential to have to add additional force to overcome some of that effect.
The common difficulties for adults with SSD are hearing in background noise, localization or spatial hearing, and being able to understand individuals who are situated near or on their deaf side. This type of problem is not only experienced by adults but also by children. Common experiences that occur when we talk about children with unilateral deafness are speech and language delay, difficulty with attention in school, difficulty hearing in noisy environments, and also difficulty localizing to sound (Bess & Tharpe, 1986). We know that kids with unilateral hearing loss are 30 percent more likely to repeat a grade than their normal-hearing peers with two good hearing ears. These are things to consider when you start talking about treatment options for these individuals.
Figure 6 is an audiogram that shows how one patient performed with the Baha. In this particular situation, the patient had very normal hearing in their left ear and had a dead ear on their right side. The aided audiogram shows the Baha aided soundfield thresholds. This was performed with the speaker on the patient's right side with the left ear plugged and muffed. You can see by the aided thresholds that the sound was picked up by the Baha sound processor and easily crossed the skull and stimulated the cochlea on the left side. What we have is a nice aided result relative to the speech articulation area.
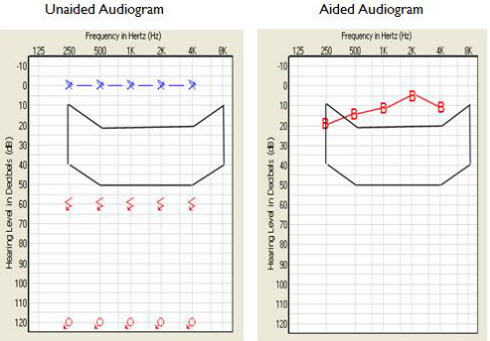
Figure 6. Unaided and aided audiograms of a Baha user. Aided Baha thresholds (B) fall within the normal hearing range.
Figure 7 is a photograph of an actual Baha that has been placed. There is a small bald spot, and you can see the implant is exposed. You can also then see where the sound processor is attached to the abutment. For patients with longer hair, particularly female patients, this can be a very cosmetically acceptable solution for SSD.


Figure 7. Baha abutment (top) with sound processor attached (bottom).
When we talk about this cross-over effect that occurs, we must recognize that transcranial attenuation does occur. Many who have studied audiology will recall that we assume a 0 dB interaural attenuation for the purposes of clinical masking, and that is translated to a generic myth that there is no attenuation of a sound once it is stimulating the skull. However, the average skull has about a 10 dB attenuation factor as the sound crosses from one side to the other. This is one of the more important things to understand and be aware of as you are working with bone-anchored devices, especially in patients with SSD.
BC Direct
Cochlear introduced a software procedure with the BP100 processor called BC Direct. It is an audiometric testing protocol where we take the fitting software for the Baha, and we turn it into an audiometer. We can produce pure-tone signals and direct them to the Baha on the abutment and ask the patient to respond, just as they would on a traditional hearing test. The advantage here is that we are able to see how the device interacts with the skull and how the signal is affected as it crosses the skull.
A study by Nolan and Lyon (1981) described the average transcranial attenuation as 10 dB. When analyzing their individual data, one can see that there were some patients that had as much as 30 dB of attenuation across the skull. This demonstrates that there is much individual variability to how these devices interact with the skull. So the BC direct measurement is quite important. Oticon Medical is now using this same kind of process, which they call in situ audiometry. It heightens the accuracy of fitting.
Figure 8 shows an audiogram where there is little or no transcranial loss of signal. The thin red line is the actual bone conduction thresholds, and the thick line with the blocks indicates the thresholds that were measured through the Baha on the abutment. This particular patient did not have a great deal of transcranial attenuation.
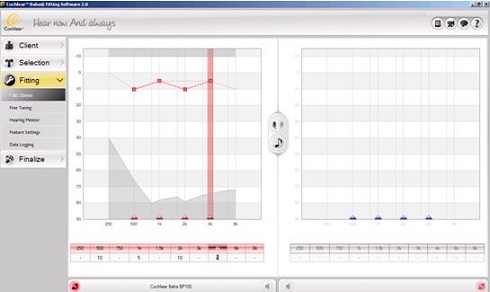
Figure 8. Screen shot of BC direct, with the Baha on the right ear. The thin, solid line represents actual bone conduction thresholds measured audiometrically; the dashed red line with blocks is the threshold measured through the abutment. The audiometrical and BC Direct thresholds do not significantly differ, indicating little to no transcranial loss.
Figure 9, in contrast, shows a patient with some transcranial loss. The bone conduction threshold, again, is the thin, solid red line. And the BC Direct thresholds are the red blocks. This patient had more loss of signal through the skull. The software that fits the device takes this difference into account and can add additional gain to make the device more effective as the signal crosses the head. As result, you will see that this particular process makes a great deal of sense for improving Baha fittings.
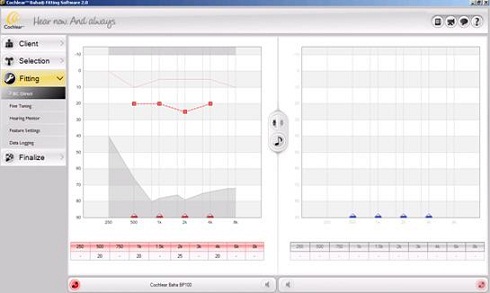
Figure 9. Screen shot of BC direct, with the Baha on the right ear. The audiometrical and BC Direct thresholds differ, indicating there is a transcranial loss for which the software will make a gain adjustment.
I am happy to field any questions that you may have. Simply e-mail me at [email protected]. And if you have any inquiries about the HOPE program, you can e-mail Donna Sorkin at [email protected] also.
Question & Answer
What do patients say about Baha, both those who are born with no hearing on one side and those who acquired SSD?
Typically, these are two different perspectives. If someone has a congenital unilateral hearing loss and lived with it a long time, they do not know any better. Furthermore, if they did not have any deleterious effects with regard to speech and language development, they often fall into the category of treatment where we do nothing.
If the loss is not creating a communication problem, it becomes harder to get motivated to do anything about it. I would have to say that individuals who acquire the hearing loss are much more likely to have an evaluation than someone who has had longstanding hearing loss. But if the hearing loss has been a struggle for them, the Baha can be quite good in that particular situation.
Is FM recommended for Baha users with SSD?
Absolutely. In school situations where there are poor acoustics, the Baha can make a big difference, but we talk with educational audiologists who see some additional improvement when they apply the FM. If the child is having some learning or attention deficit issues, the increased signal-to-noise ratio of an FM system with SSD and Baha makes quite a bit of difference and works very well.
Would you comment on the use of binaural Baha Softbands for bilateral microtia and atresia?
When there is bilateral microtia or atresia and normal, symmetrical cochlear function, it is a good idea to apply the Baha bilaterally if you can. The question then becomes, "At what age is it important?" Typically, these children are identified at birth, and you know that they have the problem, but you have to have the Bahas mounted behind their ear so that the microphone is in close proximity to the ear to be able to give them the full benefit of a bilateral presentation. However, there are some studies that demonstrate that children with bilateral microtia and atresia with symmetrical cochlear function can develop and enhance their localization ability with the use of Baha on a Softband at a young age. We try to use the Baha on a binaural Softband when the child has sufficient head control and can sit up. When they are an infant lying down, it is more difficult to manage that situation.
Can you expound on the preoperative testing you mentioned?
Absolutely. In the preoperative testing, we can apply the Baha on a hard headband or even a Softband, and we can then place the patient in the soundfield and do testing before the patient makes any determination that they actually want the surgery. We can provide a very good demonstration of how the head-shadow effect is lifted, and we can also do speech-in-noise measurements. If the patient is sufficiently impressed with that, they usually get a better result once they are implanted. When you are using a Baha on a headband or a Softband, you will deal with the transcutaneous pathway, and there are going to be skin attenuation issues, as well.
I work with eight infants and toddlers with either Baha or Ponto Softbands. Most are not wearing the devices as much as I would recommend, because families do not notice a difference and the kids do not seem to like it. I keep trying to encourage them. What would you say to them? I know that the science may be about the auditory pathways and the need of stimulating early as possible; however, there is a reality and I'm curious about how you would respond.
Yes, this is the common challenge, especially when you are in the trenches trying to manage and keep this equipment on kids. Many times it requires patient and conscientious care providers, but it also requires very good family support. If the device is only being worn when the child is at school or it is allowed to be mishandled or bounced around, it creates a challenge. When we are talking about applying the Softband technology to these kids, you really want to look at the net effect of the loss that they have, whether it be SSD, conductive or mixed loss. Typically, if the child is getting benefit from the technology, you can extinguish some of those behaviors, but I would be the first one to agree with you that this can be a very challenging issue, and it does require the village, if you will, to make all of this work.
Is Baha being used with mixed bilateral loss when traditional hearing aids cannot be used due to otorrhea?
Absolutely. One of the bigger indications to use Baha is for ears that are surgically altered or there is a medical contraindication to using traditional amplification. Chronically draining ears with conductive or mixed hearing losses are a great example of this.
Does Baha provide any tinnitus suppression?
Generally speaking, no, it does not. It is an amplifying system, but not a tinnitus masker.
References
Bess, F.H., & Tharpe, A.M. (1986). Case history data on unilaterally hearing impaired children. Ear and Hearing, 71(4), 14-19.
Harford, E., & Barry, J. (1965). A rehabilitative approach to the problem of unilateral hearing impairment: contralateral routing of signals (CROS). Journal of Speech and Hearing Disorders, 30, 121-138.
Nolan, M., & Lyon, D.J. (1981). Transcranial attenuation in bone conduction audiometry. The Journal of Laryngology & Otology, 95, 597-608.

