This course is an edited transcript of a Phonak webinar on AudiologyOnline.
Learning Outcomes
After this course learners will be able to:
- Describe the types of unilateral hearing loss.
- Describe the use cases of the Phonak Sky V, CROS II, and Roger Focus.
- Describe the process of verification of the Phonak CROS II and Roger Focus.
Introduction and Overview
In today’s seminar, we will be addressing unilateral hearing loss (UHL) in children and its impact on those children. Hearing with only one ear is not enough for a child to function normally. Modern hearing solutions from Phonak can help children with a unilateral hearing loss be ready for success. We offer multiple solutions, including the Sky V, the CROS II with the Sky V, and the Roger Focus.
UHL Defined
Unilateral hearing loss means that one ear has normal hearing thresholds, and the impaired ear can have any degree of hearing loss. Unilateral hearing loss is classified as a minimal hearing loss. Single-sided deafness (SSD) is a subset of unilateral hearing loss where there is no usable hearing on the impaired ear.
UHL in Children
How often is unilateral hearing loss present in children? One in 1,000 newborns are identified with unilateral hearing loss at birth. By the time they reach school age, 3 in 100 children may have developed unilateral hearing loss (Bess, Dodd-Murphy, & Parker, 1998). Some of the causes of UHL include bacterial meningitis, malformations of the ear canal, congenital cytomegalovirus (CMV), enlarged vestibular aqueduct syndrome (EVA), and premature birth. In some cases, the cause of UHL is idiopathic; we cannot pinpoint a specific reason why it occurred (Prieve et al., 2000).
Hearing with both ears provides a child binaural advantages that they lack when they have hearing loss in one ear. These advantages include: binaural summation, making up for the head shadow effect, sound localization, spatial release from masking, and help in reverberant situations. Any impairment can result in difficulties in real-world listening environments, such as: hearing at a distance or in noise, sound localization, segregating sounds, selective attention (ability to discern a specific sound or speaker in a noisy situation), and speech understanding.
Impact of UHL on Children: Studies
What is the impact of unilateral hearing loss for these children due to the difficulties in those environments? Because a child with UHL does not hear the full picture, they are more likely to experience difficulty in the following areas:
- Speech-language delay
- General communication difficulties
- Psycholinguistic dysfunction (ability to learn language)
- Social-emotional problems
- Quality of life effects
- Academic and behavioral difficulties
Language Scores
A study by Lieu and colleagues (Lieu, Tye-Murray, Karzon, & Piccirillo, 2010) looked at the effect of unilateral hearing loss on speech and language scores in children. It was a case-control study of 74 matched pairs of siblings (ages 6-12). They found a child with a hearing loss and compared their speech and language scores to their sibling. Their rationale for comparing siblings was that it would take out any socioeconomic factors, and focus only on the delays caused by the unilateral hearing loss.
Some of the children with UHL were unaided, and some weren’t. They administered the OWLS assessment (Oral and Written Language Scales). The children with UHL scored worse than their siblings, in language comprehension, oral expression, and oral composite. Unilateral hearing loss was the independent predictor of the OWLS scores. Family income and maternal education were also independent predictors of oral expression and composite scores.
The authors’ conclusions were that school age children with unilateral hearing loss demonstrate worse oral language scores than their sibling. In addition, withholding hearing related accommodations should be reconsidered and studied. Parents and educators should be informed of unilateral hearing loss effects on oral language skills.
Language, Cognitive, and Achievement Scores with Differing Audiologic Characteristics
Another study from Lieu and colleagues (2013) similarly compared children with unilateral hearing loss to their siblings. Again, it was a case controlled study, this time with 107 sibling pairs. In this study, they also wanted to compare and see if the outcomes were affected by the unilateral hearing loss.
Once again, the children with UHL had worse OWLS scores than their siblings. As one might expect, the children with profound unilateral hearing loss had the worst scores, in both verbal cognitive and oral language. However, there were no differences in achievement scores using the Wechsler Individual Achievement Test, where recognition scores of the normal ear in quiet and in noise correlate to higher scores.
The authors concluded that school-age children with unilateral hearing loss have worse language scores than their siblings. Furthermore, those with profound unilateral hearing loss tend to have the worst outcomes. There were no differences whether the hearing loss was in the left or the right ear.
Quality of Life
In 2007, Sarah Borton conducted a pilot study to determine whether children (ages 6-17) with UHL experience a lower quality of life. It consisted of a qualitative study, comparing children and parent focus groups, and a quantitative study, using the Pediatric Quality of Life Inventory Version 4.0.
According to the child reports, those with UHL scored more poorly for several scales than those with normal hearing or bilateral hearing loss, on all primary quality of life scales (total, psychosocial and physical). The parent reports were similar to the child reports, except better on psychosocial functioning as compared to bilateral hearing loss. The author's conclusion was that children with unilateral hearing loss demonstrated overall lower and wider range of quality of life scores compared to normal hearing peers, and their peers with bilateral hearing loss.
In summary, UHL affects about 3% of school age children, may cause issues with language and academics, and it results in a difficulty in complex or noisy environments.
Academic/Psychosocial Skill Difficulties
In the Comprehensive Handbook of Pediatric Audiology, Porter and colleagues (2016) state, "All children with permanent minimal hearing loss must be considered at risk for psychoeducational difficulties and managed accordingly" (p. 903). Let's take a look at some of the academic difficulties that may be experienced by children with UHL.
In 2004, Gravel conducted a meta-analysis, comparing the results from six studies to pinpoint the areas where children with UHL are having trouble. Across all six studies, children with UHL who failed one or more grades ranged anywhere from 18% to 40%. According to four of the studies, between 12% to 41% of students required extra help in one or more grades throughout their academic careers. Students who required both resource help and also failed a grade ranged from 48 to 65%. As the evidence suggests, these children have more difficulty in academic situations or in school than children with normal hearing. They are 10 times more likely to repeat a grade, and five times more likely to need additional educational resources. They are clearly being negatively impacted by the unilateral hearing loss in school situations.
Children with UHL had a higher incidence of failure rate or negative comments on their report card (Keller & Bundy, 1980). Furthermore, teachers rated these children more negatively than normal hearing peers (Culbertson & Gilbert, 1986). For example, whether they pay attention to an academic task, in their peer relations and social confidence, their dependence versus independence in the classroom, and emotional ability. Finally, English and Church (1999) found that teachers had behavioral concerns for children with unilateral hearing loss. If you have more trouble paying attention and it's more difficult to hear, it stands to reason that you're going to act out. You're not going to be able to pay attention as well as some of the other children in the class, and those come across as behavior issues.
Typical Classroom Noise Levels
Shield and Dockrell (2004) measured typical noise levels in 140 classrooms using an internal noise survey. They found that if one person is speaking in the classroom, it measures about 61 dB. If students are sitting at tables doing group work, it's about 73 dB; if they are doing group work with movement, it can measure up to 77 dB. Children alone working at tables is about 65 dB. During “silent” reading time, the noise level still measures about 56 dB. If people are simply moving around the classroom, it can be up to 72 dB. It’s a complex listening environment. In today's classrooms, students do a lot of group work and work at tables. Gone are the days of students sitting at their individual desks facing forward with the teacher speaking at the front of the room. Today's classrooms are more dynamic listening environments, because they are always changing. It can be very difficult to listen, even if you have normal hearing.
Children with UHL have difficulty hearing in dynamic listening situations and as such, are challenged when faced with complex listening tasks. Although their speech and language scores may be within the normal limits on some tests, as the listening environment becomes more complex, they start to break down and not perform as well as their normal hearing peers. That's why we examined the classroom setting to show that it is a complex and ever-changing listening environment.
Complex Listening Tasks
Lewis et al. (2015) analyzed complex listening tasks, using comprehension and sentence recognition. The subjects included 18 normal hearing children (ages 8-12) matched with 18 children who had either minimal hearing loss, or UHL. They were asked to perform speech recognition tasks in a simulated classroom.
All children performed at or near the ceiling. The children with unilateral hearing loss performed more poorly than children with normal hearing on the complex tasks. Individual looking behavior differed between the two groups. In other words, for those with hearing loss, attempting to visualize, or locate, the speaker may inefficiently utilize cognitive resources. That makes sense, because UHL affects localization.
The authors concluded that children with unilateral hearing loss perform more poorly than peers with normal hearing during complex listening tasks with multiple talkers. Patterns of looking behaviors differ, suggesting differences in the use of visual information. Again, those with hearing loss have trouble finding the main speaker when multiple people are talking. They have more difficulty locating the speaker; as such, they need to look around more.
Solutions for Unilateral Hearing Loss
The American Academy of Audiology (AAA) Pediatric Amplification Protocol addressed fitting of amplification on children with mild bilateral hearing loss (MBHL) and UHL in its Special Consideration section. Here is an excerpt from the guideline:
Children with minimal and mild hearing loss should be considered candidates for amplification and/or personal FM system or sound-field systems for use in school. Use of hearing aid amplification is indicated for some children with unilateral hearing losses. The decision to fit a child with unilateral hearing loss should be made on an individual basis, taking into consideration the child's or family's preference as well as audiologic, developmental, communication, and educational factors.
This decision should be made on an individual basis because there are several types of unilateral hearing loss. Furthermore, every child will be affected differently in different environments; children with UHL are a heterogeneous group. When deliberating which solution to use, the choice should be made based specifically on that child’s needs; there is no blanket one-size-fits-all solution for every child with a UHL. As we will demonstrate in the remainder of this presentation, Phonak offers multiple solutions for each type of UHL.
A child might have an aidable unilateral hearing loss, where the impairment may be mild or more severe, but they still have the ability to recognize speech. Or, a child might have severe to profound unilateral hearing loss, where the impaired ear is unaidable. As a result, they have significantly poor speech understanding in the impaired ear. What do we consider appropriate timing for treatment? Delayed amplification may lead to auditory deprivation, and the benefits of amplification have been proven.
Phonak Sky V for Aidable UHL
Let's say that the hearing-impaired ear is aidable. You can have any degree of hearing loss on that ear, from mild to severe. Amplification should be the default fitting option. Benefit can be determined during the trial period. Remote microphone usage for noisy situations or listening at a distance (e.g., in a classroom), is recommended. For this case, we have Phonak Sky V with Roger.
The Phonak Sky V is our current pediatric line of hearing aids along with the fitting range for each (Figure 1). There are five models to fit any hearing loss. The Sky V-M is for mild to moderate loss. It has the 312 battery. The Sky V-P is not just the power aid; the fitting range is very broad. It can fit a mild to moderate hearing loss, and it does have the power to fit a more severe loss. The Sky V-SP has more gain than previous superpower hearing aids, so it also can fit a pretty severe loss. The Sky V-UP has a 675 battery. We also offer the Sky V-RIC, which has three receivers and three possible fitting ranges, including a UP receiver. You can fit a fairly significant loss with the Sky V-RIC.
All Sky V hearing aids have direct audio input and mix and match color options, where you can match the housing and change the color of the tone hook. They all have tamper-proof options. You can optimize the hearing performance, especially for a child's environment, and I'll explain that later in the presentation. The IP rating for all of these hearing aids is IP68. They all have an indicator light, which means the hearing aid is on and the battery is working. When it goes into the Roger program, it can show you with two flashes every few seconds. Three flashes every few seconds indicates a low battery warning, and that you have 30 minutes to change the battery.
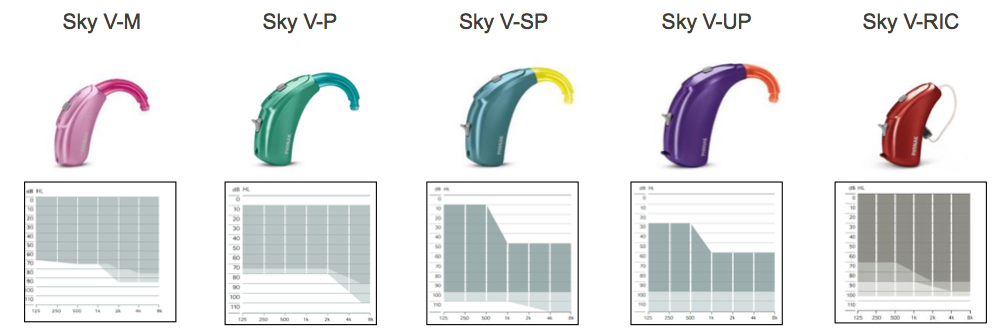
Figure 1. Sky V hearing aids and their corresponding fitting ranges.
SoundRecover2
SoundRecover2 is utilized in the Sky V line, which gives children access to a broader range of sounds essential for speech and language development. SoundRecover 2 differs from SoundRecover in that there is still non-linear frequency compression, but it is adaptive. It has two cut-off frequencies: one that is a higher frequency cut-off, and one that is a lower frequency cut off. Whenever low frequency information is coming through the hearing aid, it will only compress to the high frequency cut-off so it doesn't affect the low and mid frequencies. When low or mid frequencies come through the hearing aid, they're unchanged. If you have high frequency information coming through the hearing aid, it will compress down to that lower frequency cut-off. The reason for this is to get more high frequency sound in, even with a hearing loss that slopes off early, so that we can compress to where they need it compressed, but still preserve the mid and low frequencies. For example, if I said the word “she,” when I pronounce the “sh” part of the word, it will compress to the lower frequency to make sure that I was able to hear the “sh.” When I get to the “e” part of the word “she,” it would only compress to the high frequency cut-off, so that the “e” sound is unaffected.
AutoSense Sky OS
Phonak Sky V was specifically created to optimize hearing performance in a child's environment. AutoSense Sky OS is the automatic program used in the Sky V line. It is different from our other automatic program used in our adult hearing aids, because children often participate in situations where adults would not typically be (e.g., playing on a playground or in a park). When we took the adult classifier and we put it through a child's day, we noticed that when they were playing outside on the playground, or in physical education class where they're yelling and screaming in a gymnasium, it was switching into the music program. Therefore, we adjusted the AutoSense to go into speech in noise, and speech and comfort programs at an earlier threshold than it does with our adult hearing aids. Then, we performed research through Dr. Jace Wolf, and found that children performed better and preferred AutoSense Sky to regular AutoSense. It's designed specifically for a child's school day.
Roger and Directional Setting
In previous Phonak hearing aids (and any other manufacturer's hearing aids), when they would go into the Roger or the FM program, it would be Roger plus the hearing aid microphone (+Mic). The +Mic version would essentially be our omnidirectional Program. Now, you have the ability to turn directional microphones on or off within the Roger program. You can set it to one of three settings: Omni (which uses the omnidirectional mic), Real Ear Sound (which is close to omnidirectional, but with the pinna effect added for better localization, as well as some increase in the high and mid frequencies), or Fixed Directionality. If you choose Fixed Directionality, the hearing aid will not go into directional all the time; rather, it's an automatic directional microphone. For example, if the classroom goes above 54 decibels, you'll have Fixed Directionality; if it goes back down below 54 dB, the hearing aid will go back to Real Ear Sound. It's an automatic directional microphone within the Roger program. We chose Fixed Directional instead of "adaptive directional" for a reason. When you're in a classroom, you do a lot of lateral listening; it's important that the hearing aid doesn't reduce voices from the sides of the child. If you have Fixed Directionality, you know exactly what the hearing aid is doing at all times, and you know that it won't cut down specifically the voice of a child to the left or the right that is asking a question. Therefore, you can put the child in the appropriate place and know exactly what the hearing aid is doing at all times for lateral listening.
Quality of Life Improvement Study
McKay (2002) conducted a study to look at the improvement in quality of life for children with aidable UHL after they were fit with hearing aids. They administered surveys to 20 families with children who had mild to moderately severe unilateral hearing loss (ages 2-17). The parents' comments included, “It would be a blessing if we would have put hearing aids on these kids sooner”, and “He was missing one half of everything before he got his hearing aid.”
Most parents said that since the hearing aid fitting, the children were either doing the same, improved or greatly improved in all areas. In areas specifically related to auditory areas, all children improved. Children liked their hearing aids, parents were happy and wished their children had been fit earlier.
Phonak Solutions for Unaidable UHL: CROS II with Sky V
With severe to profound unilateral hearing loss (a.k.a., single sided deafness), where the hearing-impaired ear is unaidable, the goal of amplification is to bring sound from the impaired ear to the normal hearing ear. Phonak offers two different solutions for this type of hearing loss: CROS II with the Sky V for a more everyday solution, and the Roger Focus receiver used with a Roger transmitter as a solution for noisier situations, such as classrooms and schools. CROS stands for Contralateral Routing of Signal.
CROS II Benefits: Performance
One consideration in CROS fittings is that the child needs to be old enough to recognize the dynamics of the acoustic environment. That is the child needs to determine where the sounds and noise are coming from. A trial period is helpful. The CROS II with Sky V is the best solution for children wanting to wear a CROS, although the CROS II can also be used with Roger, for more challenging listening situations, such as a classroom.
CROS II is on the Venture platform, which provides several performance benefits as compared to earlier versions of CROS. StereoZoom is available for speech in noise. Directional microphones on the CROS transmitter mean we can use Binaural VoiceStream Technology (BVST) for better listening. It has a lower noise floor, which is important for normal hearing listeners using CROS II. It also offers 30% better battery life.
Directionality
There is directionality in all three performance levels of CROS II (Figure 2). The levels of the Sky hearing aids are V50, V70 and V90. On the hearing aid side of the CROS II fitting (i.e. the receiver side), you will have the same directionality that you would have on the aid if you weren't using the CROS II. On the CROS II side (i.e., the transmitter side), if you are using the 50 level, you will have Real Ear Sound; the 70 and the 90 levels give you access to StereoZoom.
StereoZoom is the program that narrows the directional beam to directly in front. In the 70 level hearing aid, StereoZoom can be activated by a manual button in both the hearing aid as well as the transmitter. In the 90 level, the transition to StereoZoom occurs automatically, based on the noise level in the environment.
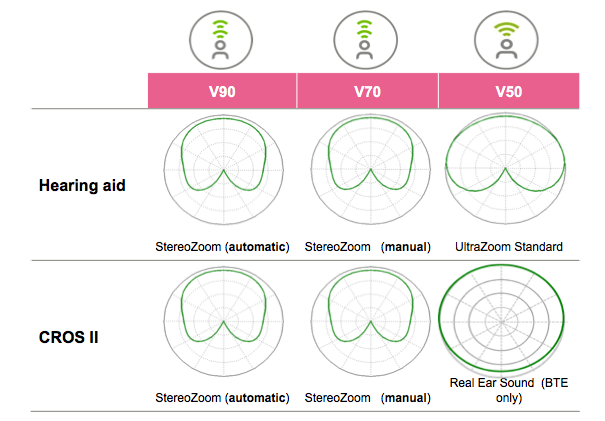
Figure 2. Directionality in Sky V 50, 70 and 90 performance levels.
Better Battery Life
CROS II provides a 30% better battery life than previous versions of the CROS. With the 312, that adds two days; with the 13, it can add up to three days of battery life as compared to prior models.
StereoZoom and Phonak CROS II
With Sky V 70 and 90, you will be able to have directionality on both sides of the CROS II fitting. Again, Sky V90 automatically goes into the directional program (i.e., StereoZoom). It does that at the lower noise floor when you're using the CROS II than it does when you have two hearing aids. When you're using the CROS II with the Sky V90 level, it will go into StereoZoom whenever the environmental noise gets above 58 dB; that is a little earlier than it would go into directional in a fitting with two hearing aids.
Low Noise Floor
Figure 3 shows a comparison of Phonak’s low noise floor to some of the competitive CROS systems as measured at the Phonak Audiology Research Center (Phonak, 2015).
The graphs show the noise floor levels by frequency for the Phonak (green) and the competitor (grey) CROS. Frequency lowering, feedback cancellation and any sound cleaning features were disabled. Standard tubing and an occluded standard earmold without venting was selected in both Phonak Target and the competitor’s software. For the measurements, the CROS devices were programmed for 0 dB hearing thresholds in the better ear. Adobe Audition was used to record noise floor levels and stimuli through KEMAR.
The noise floor, or 0 dB HL (normal hearing), is represented by the red line. Ideally, the noise floor should be as close to (or below) normal hearing as possible, so that the wearer doesn’t hear any noise in quiet settings. The graph shows that the Phonak CROS II system revealed a lower noise floor. With CROS candidates often presenting with thresholds better than 20dB HL, noise levels between 20 and 35 dB SPL as seen with the competitive device, would certainly be audible and possibly interfere with audibility for soft sounds. With Phonak CROS II, CROS users would not have any audibility of the noise floor thus experience better audibility of soft sounds.
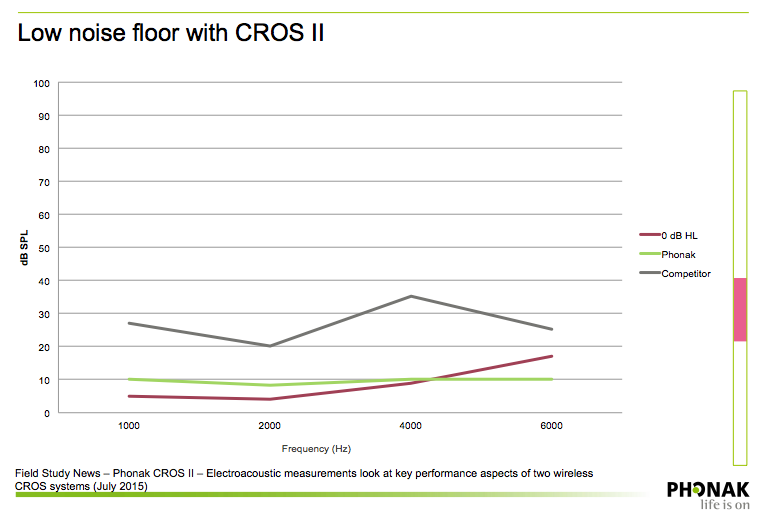
Figure 3. Noise floor: CROS II versus competitive CROS system.
Directional Microphone Benefit
Figure 4 shows the results of a comparison between the Phonak CROS II (left) and the competitor’s CROS product (right) as measured by the Phonak Audiology Research Center. You can see that there is more separation between speech from the front and noise from the side with the CROS II, and that the directionality is active at a lower level as compared to the competitive product.
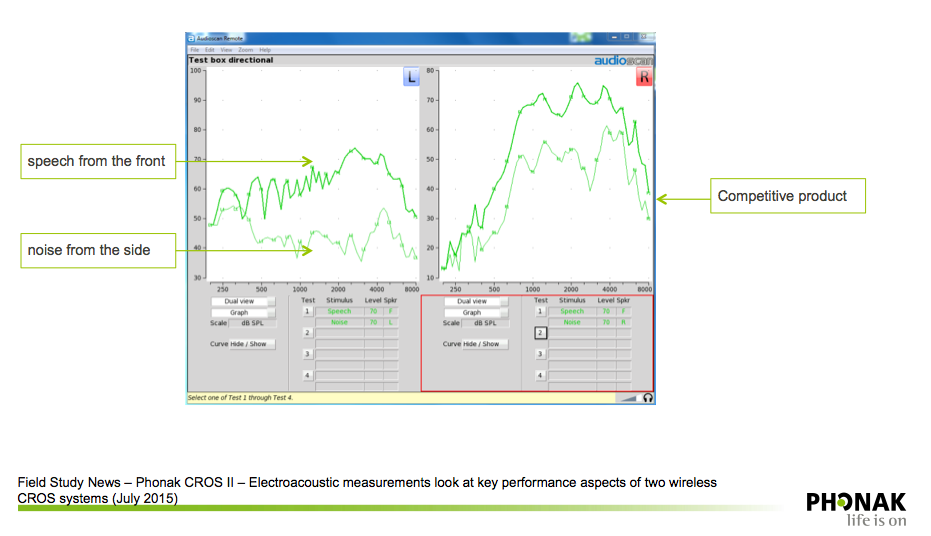
Figure 4. Directional microphone benefit: CROS II versus competitive CROS system.
CROS II Benefits: Ease of Use
Many of the improvements that Phonak implements are based on feedback from professionals. This is evidenced by some of the differences between the CROS and the CROS II. Some improvements as they relate to ease of use include automatic switching to Roger with Sky V RogerReady, as well as a simplified fitting approach.
RogerReady. The Sky V product line has a feature called RogerReady. With RogerReady, the hearing aid will be able to go back and forth between the Roger program and the automatic program, or the CROS program. In the classroom, whenever a teacher speaks into the microphone, it will switch to the Roger program within 400 milliseconds. It's fast and effective because it happens 100% of the time. When a student goes out to the playground or the cafeteria, or anytime it stop getting the Roger signal for 50 seconds, it will switch back into the other programs (e.g., with CROS II, it would switch to the CROS program). It will switch back and forth between CROS and Roger without having to press a button. Therefore, CROS II is easier to use with Sky V than ever before. You don’t have to rely on a young child or a teacher pushing a program change button on the hearing aid or remote control. It happens automatically.
CROS II: Simplified Fitting Approach
When performing a CROS II fitting in Junior Mode, you will see a screen similar to the image in Figure 5. You won't have to add in a Roger program, but the default for Junior Mode fittings is to start up in the Roger program. If you are fitting CROS II, you'll change the startup program to AutoSense Sky OS, which is the automatic program. If you don't want to use the automatic program, you can have it start up in Calm (or your preferred start up program). As you can see in Figure 5, there is a check box for RogerReady in the lower right corner. RogerReady is defaulted to “On” in all Junior Mode fittings. With RogerReady on, it will automatically switch back and forth between the Roger program, and the program of your choosing for the startup, based on whether someone is speaking into the Roger microphone.
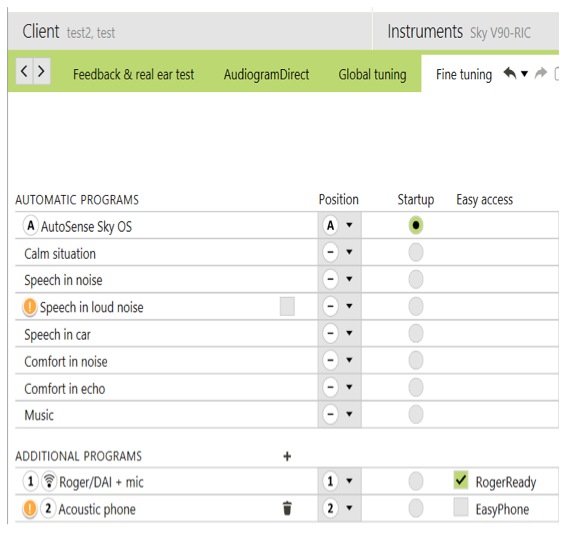
Figure 5. CROS II fitting in Junior Mode.
As compared to previous CROS fittings, fitting CROS II is easier because with iCube II, the CROS is live during the fitting. With iCube, you won't have to connect and then disconnect everything, then reconnect everything again to return to the programming. The CROS II is during the fitting as long when using the iCube II.
If you don't fit CROS very often, and you want to brush up on it, the Phonak CROS Solution Fitting Guide is a great resource available on our website. You'll notice that it refers to fitting the CROS II or the CROS B. The CROS B is for the Audeo B. It has all the same features as the CROS II, just a new housing. The CROS B works with all of the Audeo B devices, except for the rechargeable device.
CROS II Benefits: Look and Feel
Another difference between the original CROS and the CROS II is the new housings, new housing colors, as well as the ability to use the CROS Hook.
BTE Choices
CROS II is available with either a size 13 battery or 312 battery (Figure 6). With the size 13, you can use a CROS Hook, which is just a regular tone hook, so that you can put a traditional ear mold in the ear. This is helpful for those little ears where you can't keep the SlimTube in the ear because it always falls out. When you use an ear mold on the normal hearing side with the CROS, its purpose is retention. You want to make sure that it is as open as possible, for comfort reasons. You can also use the SlimTube. You can still use the CROS Tip, which is also shown on the hearing aid on the far right in Figure 6. The CROS Tip is a hollowed-out kind of sleeve mold that attaches to the end of the SlimTube.
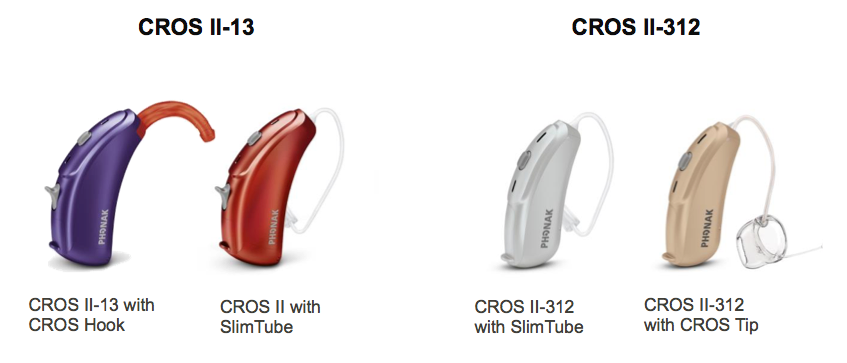
Figure 6. CROS II BTE choices.
New housing color choices. Previously, with CROS, color choices were limited for the hearing aid side. Now, we have all of the pediatric colors to match the CROS (Figure 7).

Figure 7. Phonak CROS II-13 new colors.
Phonak CROS II-13 with CROS hook: Child friendly design. The child-friendly design includes: BTE size 13 housing; IP67 rating; 18 housing colors; seven CROS Hook colors to mix and match with Sky V; a push button and volume control; high-tech composite material; tamperproof door available. Using the CROS Hook and Sky V-P tamperproof battery door will meet the IEC standards for small children.
To put the ear hook on, simply push the pin towards the center of the hearing aid out. That will allow you to remove the spine. Then you'll just replace that spine with the ear hook, and then push the pin back into place.
Verification of CROS II: Setup and Procedure
Set up. First, position the client in front of the speaker. Next, program the hearing instrument and the CROS II transmitter in the Target software. If you are using the iCube II, hang the iCube II around the client’s neck to allow for instant adjustment based upon verification feedback.
Measure the aided response for the “better hearing ear.” Place the reference microphones on both ears. You'll place reference mics on both ears, but you'll only put the insert probe microphone in the better ear. Place both the hearing instrument and the CROS II transmitter on the ears. Ensure that the instrument is programmed and active. Select “on ear measure,” and record the response at either 55 or 60 dB SPL with the speaker directly facing the better ear (as shown in Figure 8).
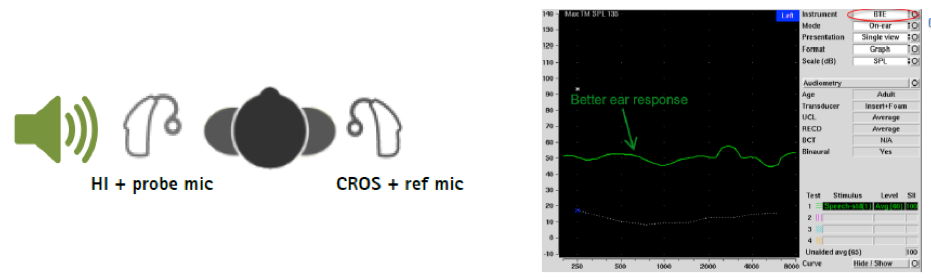
Figure 8. Measuring the aided response on the better hearing ear. The better ear response is the green line on the graph (right).
Measure the aided response in the poorer ear. Don't change the positions of the probe microphone, the reference mic, or the CROS system. Ensure that the hearing instrument and the CROS transmitter are still turned on. Change the hearing instrument selection to “CROS.” Rotate the client so that the speaker directly faces the poorer ear, and then record the response (Figure 9).
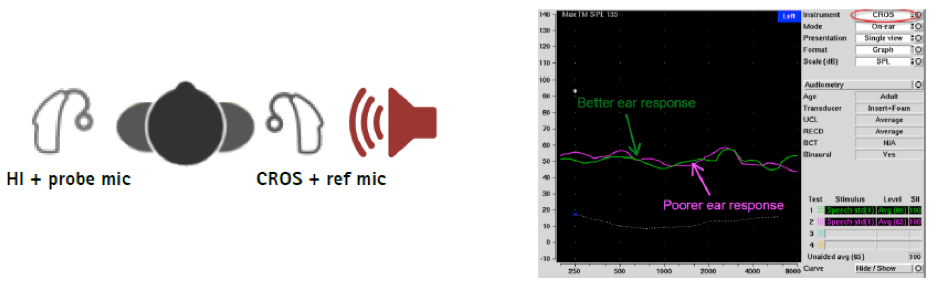
Figure 9. Measuring the aided response on the poorer hearing ear. In this case the better ear response (green line on graph) and poorer ear response (pink line on graph) are similar.
Ideally, the “better ear” and the “poorer ear” responses should be within 2 - 3 dB of each other. If they differ greatly, fine-tuning may be required to allow them to match as closely as possible. If they are very different, always check the position of the speaker when you're switching sides to ensure that the placement of the speaker to the ear is identical. Check the position of the instrument on the ear. Check the position of the hearing aid and the CROS to make sure they're sitting on top of the ear in the same way. Verify that the programming of the CROS is balanced and comfortable. If you are unable to match the two responses, check the CROS system to ensure it is functioning properly. If the CROS system is not working or the transmitter is faulty, you may see very different responses, similar to the ones pictured in Figure 10.
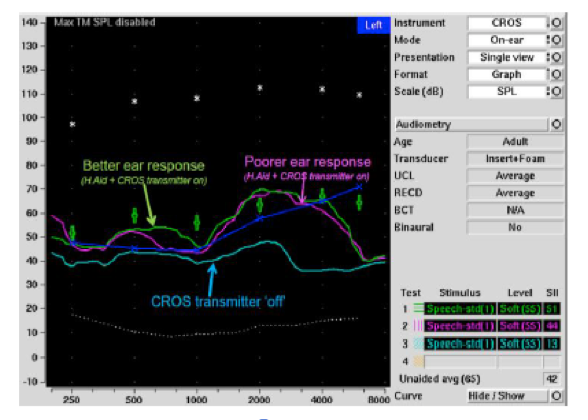
Figure 10. Better ear response (green line) and poorer ear response (pink line) are not within 2-3 dB of each other. This indicates that the CROS system or transmitter may be faulty.
Phonak Solutions for Unaidable UHL: Roger Focus
The second option for children with SSD or unaidable UHL is to wear a remote wireless microphone system like the Roger Focus. For children with severe to profound hearing loss, Roger Focus increases the signal-to-noise ratio (SNR) to the normal hearing ear. It is beneficial not only in classrooms, but also in cars, at social settings, and anytime where noise or distance makes it difficult to hear well.
The Roger transmitter will transmit the signal directly to the Roger Focus providing a better SNR. It's an easy and comfortable receiver (Figure 11). It has a push button volume control, which you can deactivate by pressing and holding the volume control down for five to seven seconds. It is a ready-to-wear design, using a SlimTube and dome. It uses a 312 battery, and opening and closing the battery door will turn it off and on.
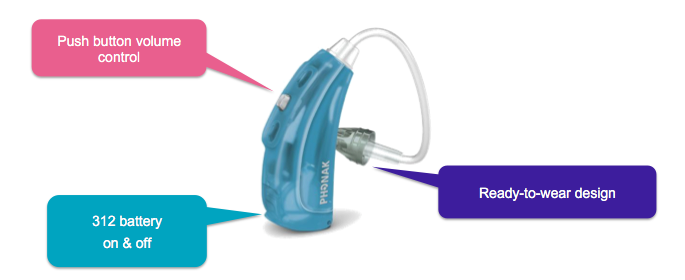
Figure 11. Roger Focus easy and comfortable receiver.
SlimTubes are available in four sizes (0-1-2-3) and domes are available in three sizes. At start up there is minimum volume, and you can increase volume by increments of two decibels until it reaches the maximum volume, using the push button volume control. At maximum volume, pressing the volume control will revert down to the minimum volume. If you don't want the child to have control of the volume, press and hold the volume control button for a few seconds to disable the volume control.
When fitting an ear-level wireless receiver like Roger Focus that is used on a normal hearing ear, you should leave the ear canal as open as possible. The child should be able to hear environmental sounds and speech normally from the good side. SlimTube is standard, but Roger Focus can also be used with an ear hook and an open ear mold. If you do have to go with an ear mold, use a regular tone hook and ear mold with as big a vent as possible. SlimTube is standard, but Roger Focus can also be used with an ear hook and an open ear mold. Roger Focus is available in 17 colors.
All Roger microphones and media transmitters are available with Focus (Figure 12). These include the Roger Touchscreen Mic with the Roger Pass-around and Multimedia Hub; you can also go with a Roger Pen, or even the Roger Clip-On microphone.
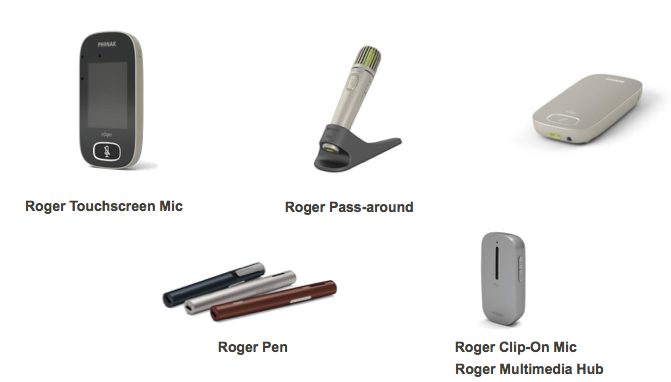
Figure 12. Roger microphone and transmitter choices.
Maximum Performance Using the Roger Focus
In 2014, Jones and team at the Phonak Audiology Research Center (PARC) conducted a study using 15 school children who were previous users of iSense (our FM solution similar to the Roger Focus) or MicroEar (Figure 13). The goal of the study was to obtain speech-in-noise testing results using no device, and then compare that to results using the Roger device. Some of the children (e.g., subject numbers 2, 4, 12 and 14 in Figure 13), went from being able to hear almost nothing in a noisy situation with no solution, to close to 100% when using the Roger Focus. The data show a wide variety of benefits that can be realized with Roger Focus. This relates back to the importance of fitting children individually, because each child is uniquely affected by his or her unilateral hearing loss. There is not a “one size fits all” management approach when it comes to UHL.
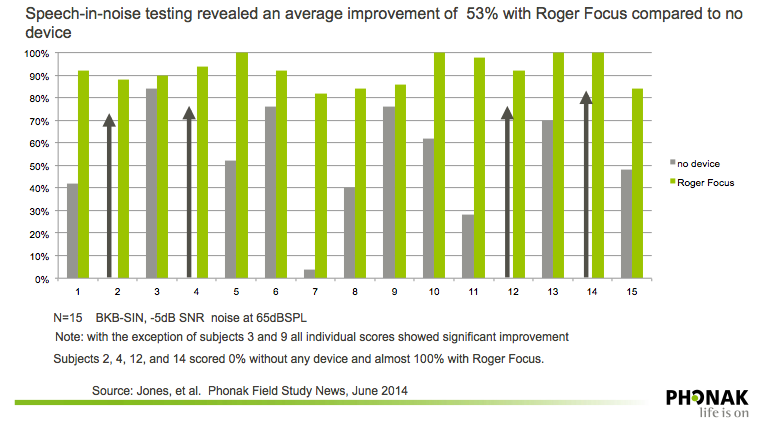
Figure 13. Speech-in-noise testing with Roger Focus as compared to no device. Source: Phonak Field Study News (2014).
Verification of the Roger Focus
In 2008, AAA suggested procedures for fitting remote microphone hearing assistance devices like the Roger Focus, including in the ear probe microphone measures. Schafer and colleagues (2014) conducted a stody to validate the AAA guidelines and recruited 26 normal hearing children. Their goals of obtaining real ear measures for RMHA (remote microphone hearing assistance) were:
- To verify the measured output for prescribed-gain targets from 1 to 4 kHz for speech stimuli
- To confirm that the RMHA volume did not exceed predicted loudness discomfort levels
- To assess changes to the real ear unaided response (REUR) when placing the open sound delivery system in the ear
They found that on average, prescription targets were met from 1 to 4 kHz within +/-3 dB, although at times the high frequency targets at 3 and 4 kHz could not be met. Maximum power output (MPO) of the RMHA never exceeded MPO limits and overall, was significantly less than estimated uncomfortable loudness levels (UCLs). Some change in the REUR due to the open sound delivery system were noted, but the differences were small.
Procedure. To assess changes in REUR, follow this procedure.
1. Insert the probe tube
2. Select 'on ear measures', real ear insertion gain, BTE.
3. Record the client's REUR for a moderate stimulus level (e.g., 65 dB SPL)
4. Insert the RMHA into the ear but leave the device turned off. Select “REAR” (real ear aided response), and present the stimulus at the same level used in Step 3.
If the REUR is similar to REAR1 (i.e. curves overlay one another), it means that the REIG (real ear insertion gain) is approximately 0 dB. This implies minimal disruption of residual hearing function by the presence of the open fit sound delivery system.
Verification of RMHA output. To verify output of the RMHA, follow these steps. Refer to the handout that accompanies this course for supplemental photos of these steps.
1. Enter the pure tone audiogram into the verification system.
2. Select “FM” from the hearing instrument menu.
3. Select the “on-ear” mode.
4. Switch the transmitter into its verification mode and place it in the test box with its mic aligned iwth the reference mic. For dynamic FM, switch into omnidirectional mode. For the Inspiro, you only need to ensure the lapel microphone is in the test box.
5. If the device has a manual volume control, set this to maximum and select the 'MPO' stimulus. If required, adjust the receiver settings to ensure the MPO isn't exceeding targets at this maximum volume setting. If there is no manual volume control, skip this step.
6. At user volume, select Std-Speech (1) or (2) and choose 'FM chest' or 'FM Boom' for level, depending on which type of microphone you are using. Record the speech curve and check against targets in the 1 to 4 kHz region.
7. If desired or required, adjust the RMHA gain setting to try to meet targets from 1 to 4 kHz.
Note: You can only adjust Roger Focus gain with the Roger Inspiro transmitter. For iSense micro, you can use the FM Successware.
8. Re-run the MPO at the user volume setting after any gain adjustments have been made, to make sure that it is not exceeding MPO.
Roger DigiMaster 5000 & 7000
Sometimes, you might not be able to use the Focus because you can't use an on-ear system. For example, if the child has draining ears, sensory issues (they don't like things in their ear), or ear malformations, you may be unable to put a device in the ear. In cases like these, you can use a Roger DigiMaster 5000 or 7000, which are sound field solutions for classrooms.
Summary
Porter and colleagues (2016) stated: “With the known struggles of children with unilateral hearing loss, the most professionally responsible approach is recommended. That is, all children with hearing loss should be provided with the tools necessary to help them reach their full potential"
Phonak can help children with UHL be ready for success with the Phonak Sky V, the Phonak CROS II with the Sky V, and the Roger Focus. The Roger solutions in noise include adding Roger to the CROS II or the Sky V. We also have design-integrated Roger solutions for cochlear implants, as well as bone-anchored hearing aids.
I'd like to leave you with this quote from Krishman and Van Hyfte (2016): “With infants being identified with UHL at a very early age, it is time for clinicians to consider all intervention avenues available, and to take the opportunity to positively impact the development of children with unilateral hearing loss to help them reach their maximum potential.”
Questions and Answers
Who chooses whether the FM is in directional or omnidirectional? Is that chosen by the audiologist or in programming, or through the Roger transmitter?
That is done through the Target software. When you're programming the hearing aid, you can go to Program Options in the Roger program options and choose Omni, Real Ear Sound, or Fixed Directional.
Can a child utilize the function of a CROS while also utilizing FM?
Not at the same time. We would like to be able to hear the CROS as well as Roger FM at the same time, but we're not there yet. We can stream from aid to aid, and we can also stream from Roger to the hearing aid, but not at the same time. so we are still working on that. But the CROS II is more easily used than the previous versions of the CROS.
I usually have the student take off the CROS piece when using the DM. Should it be left off?
You can leave the CROS piece on. With the previous version, they didn't switch back and forth, so you had to change the program. Then if you took the CROS piece off, you might be able to save battery. I would leave the CROS on, that way when it switches back and forth. It will work appropriately, and if you take the CROS off, the CROS won't be active until you put it back on.
Is there any way to use the CROS II on a child with atresia or microtia? I have parents who want non-surgical options at home.
They use the Focus at school for these students. You can use the CROS II if there is a way to attach it. I don't know about using a soft band; I've never seen that used in these cases. Just like a hearing aid, you do have to somehow be able to attach the CROS II.
What is the default setting when you use the Sky plus Roger program? Does it start up in Omni, Real Ear Sound, or Fixed Directional?
It will depend on the age of the child. If you go in Target, you can look at all of the default settings. I think from birth to three, it's Omni. For the next age range of four to eight, the default is Real Ear Sound. Above age 8 years it is Fixed Directional, but you can also change the default settings in the Target software.
Is there a solution for putting an FM system on a toddler without removing the tamper-proof battery door?
You can get an integrated Roger receiver that has a tamper-proof solution attached to it. The receiver itself becomes the battery door, and it is tamper-proof. If you need tamper-proof, go with an integrated receiver.
Is there research available addressing the Roger Focus versus classroom amplification?
There is research comparing ear level amplification to sound field amplification but not specifically that I'm aware of with unilateral hearing loss, or specifically to the Roger Focus.
When using the Roger with the CROS II, should you leave the CROS II on the profound ear so the RogerReady can take its place?
With CROS fittings, you'll always have a hearing aid side and a CROS side. When you program, you're actually programming the hearing aid, and letting it know that the CROS II is there. The CROS II would always go on the poorer ear, and then the hearing aid would go on the better ear.
Selected References
American Academy of Audiology (AAA). (2008). American Academy of Audiology Clinical Practice Guidelines: Remote Microphone Hearing Assistance Technologies for Children and Youth Birth-21 Years. AAA Supplement - Supplement A. Fitting and Verification Procedures for Ear-level FM. Available from author: www.audiology.org
Bess, F.H., Dodd-Murphy, J. & Parker, R.A. (1998). Children with minimal sensorineural hearing loss: Prevalence, educational performance, and functional status. Ear & Hearing, 9, 339–354.
Borton, Sarah A., (2007). Quality of life in children with unilateral hearing loss: a pilot study. Independent Studies and Capstones, Paper 201. Program in Audiology and Communication Sciences, Washington University School of Medicine. https://digitalcommons.wustl.edu/pacs_capstones/201
Culbertson, J.L. & Gilbert, L.E. (1986). Children with unilateral sensorineural hearing loss: cognitive, academic, and social development. Ear & Hearing, 7, 38-42.
English, K., & Church, G. (1999). Unilateral hearing loss in children: An update for the 1990’s. Language Speech & Hearing Services in Schools, 30, 26-31.
Gravel, J. (2004) Minimal hearing loss in children. Presentation at Phonak Satellite Conference, NHS. Available from phonakpro.com
Keller, W.D., & Bundy, R.S. (1980). Effects of unilateral hearing loss upon educational achievement. Child: Care and Health Development, 6(2), 93-100.
Lewis, D.E. (2016) An update on children with unilateral hearing loss: What do we know and where do we go? Presentation at 2016 Pediatric Audiology Conference, Boys Town National Research Hospital, Omaha, NE.
Lewis, D., Schmid, K., O’Leary, S., Heinrichs-Graham, E., Spalding, J. & High, R. (2016). Effects of noise on speech recognition and listening effort in children with normal-hearing and children with mild bilateral or unilateral hearing loss. Journal of Speech Language Hearing Research, 59(5), 1218-1232. doi: 10.1044/2016_JSLHR-H-15-0207
Lieu, J. (2004). Speech-language and educational consequences of unilateral hearing loss in children. Arch Otolaryngol Head Neck Surg, 130(5), 524-30.
Lieu, J.E.C., Karzon, R.K., Ead, B. & Tye-Murray, N. (2013) Do audiologic characteristics predict outcomes in children with unilateral hearing loss? Otol Neurotol 34(9), 1703–1710.
Lieu, J.E.C., Tye-Murray, N., Karzon, R.K. & Piccirillo, J.F. (2010) Unilateral hearing loss is associated with worse speech-language scores in children. Pediatrics, 125, 2009-2448. doi: 10.1542/peds.2009-2448
McKay, S. (2002, July 22). To aid or not to aid: Children with unilateral hearing loss. AudiologyOnline. Retrieved from www.audiologyonline.com
Phonak Audiology Research Center, PARC-SEDOL Experimental Roger Laboratory. (2014) Roger Focus Validation. Phonak Field Study News.
Phonak. (2015). Phonak CROS II – Electroacoustic measurements look at key performance aspects of two wireless CROS systems. Phonak Field Study News.
Porter, H., Bess, F.H., & Tharpe, A.M. (2016). Minimal hearing loss in children. In A.M. Tharpe and R. Seewald (Eds.), Comprehensive handbook of pediatric audiology (p. 903). San Diego, CA: Plural Publishing.
Prieve, B., Dalzell, L., Berg, A., Bradley, M., Cacace, A., Campbell, D.,...Prieve, B. (2000). The New York State universal newborn hearing screening demonstration project: Outpatient outcome measures. Ear & Hearing, 21(2), 104 –117.
Schafer, E., Bryant, D., Sanders, K., Baldus, N., Algier, K., Lewis, A.,...Amin, A. (2014). Fitting and verification of frequency modulation systems on children with normal hearing. J Am Acad Audiol, 6, 529-40. doi: 10.3766/jaaa.25.6.3
Shield, B.M., & Dockrell, J.E. (2004). External and internal noise surveys of London primary schools. Journal of the Acoustical Society of America, 115, 730-738.
Watier-Launey, C., Soin, C., Manceau, A. & Ployet, M.J. (1998). [Necessity of auditory and academic supervision in patients with unilateral hearing disorder. Retrospective study of 175 children]. Ann Otolaryngol Chir Cervicofac,115(3),149-55. [article in French]
For further references, refer to the handout that accompanies this course, or contact Phonak.
Citation
Bowers, D. (2017, May). Unilateral hearing loss: Impact and solutions. AudiologyOnline, Article 19953. Retrieved from www.audiologyonline.com

