
Question
When I create a new hearing aid fitting for a patient, why doesn't the simulated display in the fitting software match the actual output in my patient’s ear?
Answer
As hearing care professionals, we rely heavily on the fitting software to program, fit and fine tune today’s hearing aids. In the software, we can choose to fit to a variety of fitting rules and gain and target curves are quickly calculated and displayed, typically using a view that is meant to represent the response inside the ear. Fitting software has made creating new fittings a quick, automated process, and it’s easy to assume that what you see on the screen represents what the hearing aid is actually doing. But it’s important to remember that the display is a simulation of an in-ear fitting. There are many averages, calculations- assumptions, even- used by the fitting software to create the simulation, which can differ dramatically from the ear of any one patient.
Several studies have shown that fitting software displays do differ from the output measured in the ear. In general, the greatest deviation from simulated gain or targets is measured in the high frequencies (2-4 kHz) and is in reality lower than what is predicted by the fitting software, up to 10 dB or more (Hawkins & Cook, 2003; Aazh & Moore, 2007; Sanders et al, 2015). This pattern appears in similar ways across hearing aid styles, manufacturers and prescriptive fitting rules. In addition, measured output for softer inputs may be lower than prescribed targets, while louder inputs may be higher than prescribed targets (Sanders et al, 2015).
To understand why the simulated view in the fitting software might not replicate the gain or output in the patient’s ear, it’s helpful to understand where the displayed values come from in the first place. Let’s use an example patient (Mr. F) to help explain. Mr. F has a bilateral sloping sensorineural hearing loss and will be fitted binaurally with receiver-in-the-ear devices using medium power receivers. His hearing loss is very similar to the hearing losses used in the above cited studies and is of course very commonly seen in hearing aid patients.
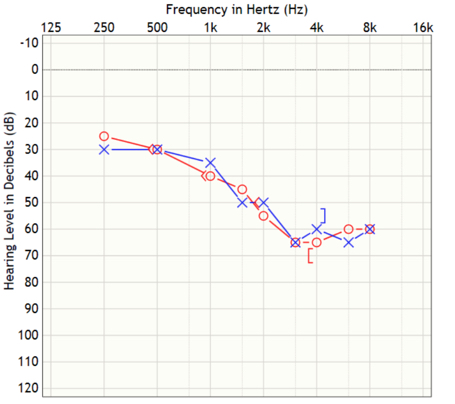
Figure 1. Mr. F’s audiogram
In the simplest sense, the fitting software relies on Mr. F’s pure tone thresholds to calculate his fitting, using the prescriptive fitting rule chosen by his HCP (which in this case is NAL-NL2). The result is a simulated fitting with prescribed target curves for each input level and the gain to match targets currently set in the hearing aid. This is the default fitting, and it is displayed below in Figure 2:
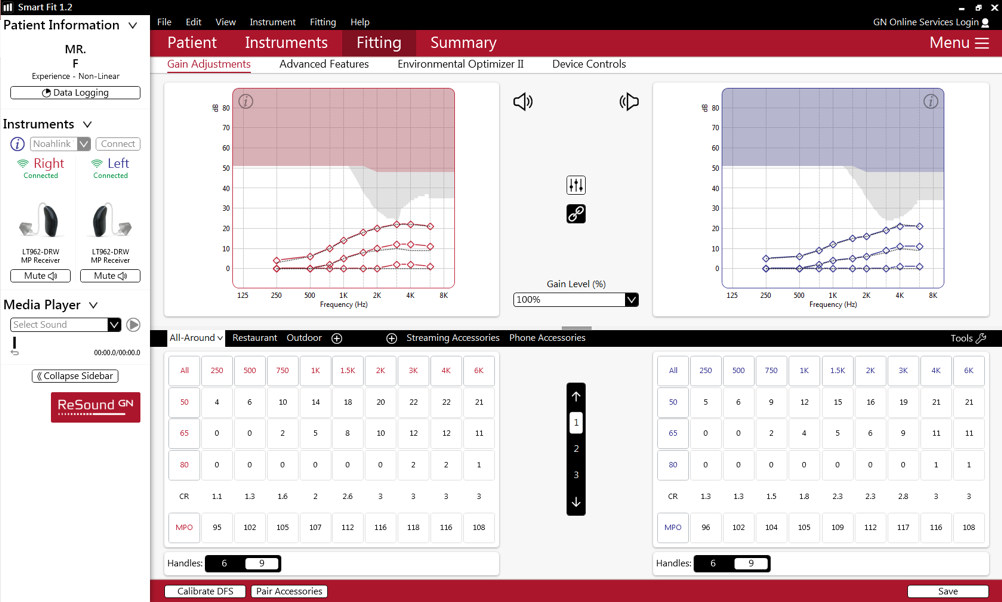
Figure 2. Mr. F’s default fitting in the software, using NAL-NL2 targets, in insertion gain view.
The display is only as good as “average”…
The default view for Mr. F’s fitting is insertion gain, which simulates the gain in the ear of the patient. Most HCPs use either insertion gain, or a simulated output view, in the fitting software display. This makes sense, since when HCPs fit a hearing aid, they mostly care about what a hearing aid is doing when it’s inside a patient’s ear. However, the design, measurements and verification of a hearing aid at the manufacturer are all done using couplers. This can include the calculation of gain or output for any given fitting in the fitting software. In order to make the jump between coupler gain to simulated real ear gain, a conversion must occur. This is the CORFIG, or COupler Response for Flat Insertion Gain (Killion & Monser, 1980). It is a set of offsets, in dB, required to convert between measurements from a coupler and a simulated real ear response.
CORFIG is comprised of three variables. These variables are real ear unaided gain (REUG), microphone location effect (MLE) and real ear to coupler difference (RECD) (Killion & Monser, 1980; Mueller, 2001).
- Real ear unaided gain (REUG): If we want to simulate what happens to hearing aid gain in the ear of a person, we need to start with the effect humans have on incoming sound. REUG allows us to account for the natural resonance effects of the ear, head and body on sounds entering the open ear canal in a free field.
- Microphone location effect (MLE): When sound presented in a free field enters a hearing aid microphone, it will undergo changes in its frequency response, and this response will differ depending on where the microphone is physically located on the person. The closer the microphone is to the eardrum, the more closely the hearing aid microphone response will match the open ear response. CIC instruments have the smallest MLE, while BTEs have the largest of ear-level hearing aids, since their microphone placement is so far away from the eardrum of the listener. Practically, separate CORFIGs must be created for each hearing aid model or style, in order to account for MLE.
- Real ear to coupler difference (RECD): If the same input is presented to a hearing aid inside a coupler and then inside a real ear, the output will differ. That difference across frequency, in dB, is the RECD. Utilizing the RECD alone in creating simulations of insertion gain will not work, as we are missing information on how sound is altered by the person wearing the hearing aid (REUG) and where sound is entering the system (MLE).
Although the definition of CORFIG is standard in the industry, how to obtain them is not (Fabry, 2003). CORFIGs can be calculated using standardized, published data or measured, using either KEMAR or a group of human subjects. There is not necessarily a standard set of data or measurement techniques used by everyone. What this means is that each hearing aid manufacturer uses their own implementation of CORFIG. This is clearly shown in Figure 3, where the CORFIG was derived for six receiver-in-the-ear hearing aids using low-power receivers, each from a different manufacturer. Every hearing aid was programmed with the same 20 dB insertion gain, then output was measured in a 2-cc coupler. When subtracting the 20 dB of insertion gain, we are left with the CORFIG. Even when utilizing similar hearing aids, there is as much as 14 dB of variation across the manufacturers at the lowest and highest frequencies measured, and 10 dB of variation at 3150 Hz. Since these are low-power receiver-in-the-ear devices, we can assume they will likely be fit using open domes, which means there will be even more variability around 2-4 kHz, depending on the individual REUG of the person wearing the hearing aid.
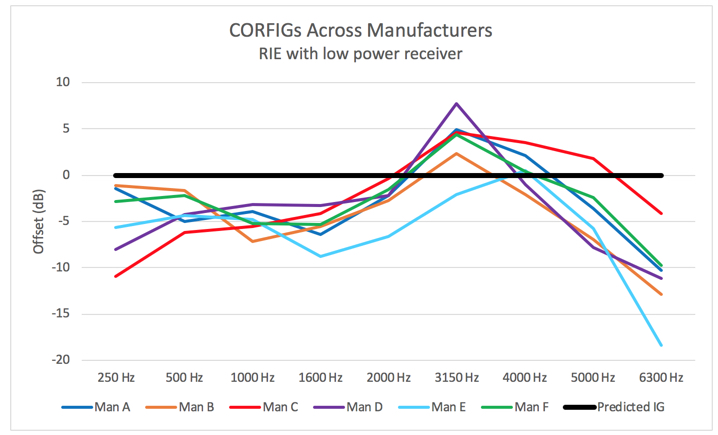
Figure 3. CORFIGs for low-power RIE hearing aids from six different manufacturers. Despite the similarity in terms of device type, there is quite some variation in the responses.
The CORFIG used by the creators of each validated prescriptive fitting rule also differs. When a manufacturer includes third party prescriptive rules in their software, they need to use a CORFIG from somewhere, which is likely to be the one that was developed internally, since third party CORFIG information isn't always available. This is going to lead to more variation in target and gain curves based on manufacturer and fitting rule.
…and it can’t tell the whole story
The CORFIG provides an average starting point for the fitting, but there are even more variables driving the fitting and they aren’t necessarily accounted for on the display at all. One common example are real-world fitting factors, such as the insertion depth and venting. Some fitting software displays will take these variables (if known) into account, while others will not. Of course, we know that regardless of whether or not the simulated display accounts for it, the actual real ear output will reflect these variables.
Recall that Mr. F’s fitting is based on the NAL-NL2 prescriptive rule. Going back to Figure 2, you may have noticed that not all the points on the gain curve (solid red/blue lines) match up perfectly with the target curves (grey dotted lines). Since this is the default fitting with no fine tuning, we would expect that gain and targets would be equal at all frequencies. What happened? We have run into a software constraint that prevents a “textbook” implementation of the fitting, and it is not so obvious based on the display.
This hearing aid fitting is calculated using pure tone stimuli as the input. So imagine for each frequency channel, a pure tone is presented, and the resulting gain to reach the desired output (which is determined by the fitting rule) is displayed. But there can be limits to what the fitting software prescribes and what the hearing aid can actually produce. For Mr. F’s fitting, there are a few channels where the difference in prescribed gain between input levels is too large. The hearing aid is limited to a 3:1 compression ratio, so the gain must vary slightly from the target in order to stay at or below this compression ratio. In addition, the compression kneepoints used in the fitting are not identical to those estimated by the creators of the NAL-NL2 prescription to achieve the targets. The difference in kneepoints are most often not visible on the screen. But when doing verification, the puzzling result can sometimes be less compression at the lower input levels than what the fitter was expecting. In other words, aided gain curves for the low and moderate input levels may be much closer to each other than was anticipated.
Mr. F isn't going to spend much time, if any, listening to pure tone stimuli in real life. He will instead be listening to lots of speech, music and other complex sounds. We could use a different view in the fitting software to help better understand how the hearing aid will behave in situations involving speech. This view converts the pure-tone generated targets and gains into those using a more broadband, speech-weighted stimulus. However, we're still looking at a simulation that was converted from the pure tone simulation so the match won’t be exact. The same is true going the other direction – if the default manufacturer view is based on a specific speech-weighted or speech-like signal, switching to a pure-tone based view can in the same way introduce small inaccuracies due to the conversion factors.
What it all comes down to
It is helpful to have the background knowledge on how fitting software displays are generated from the manufacturer, but in the end, you will still only be left with a simulation based on averages. Manufacturers may regularly update their proprietary CORFIGs as they continually try to improve the electroacoustic performance of their products, but there is currently no way to guarantee how much each of your individual patients will vary from the average. Validated prescriptive fitting rules can cause even more variation between the display and real life, simply because the variables in their creation can differ from those within any one manufacturer and how their products are designed. Based on surveys of clinical practice, manufacturers must assume that most fittings will not be verified using real ear measurements (Mueller & Picou, 2010). Therefore, it is pragmatic to veer those averages below rather than above meeting targets to prevent overshooting gain in a significant amount of ears. An exact match to average prescribed gain would result in 50% of fitted ears over target, a fitting result that can negatively affect sound quality and increase risk of feedback. Ultimately, this brings us to an important, not unexpected, and often made point: that in order to understand what is happening inside the ear(s) of your patient, you must measure it.
For more information, please visit www.resound.com or the ReSound Partner Page on AudiologyOnline.
References
Aazh, H. & Moore, B.C. (2007). The value of routine real ear measurement of the gain of digital hearing aids. Journal of the American Academy of Audiology, 18(8),653-664.
Fabry, D. (2003).Nonlinear Hearing Aids and Verification of Fitting Targets. Trends In Amplification,7(3), 99-115.
Hawkins, D. B. & Cook, J. A. (2003). Hearing aid software predictive gain values: How accurate are they? Hearing Journal, 56(7), 26-34.
Killion, M.C. & Monser, E.L. (1980). CORFIG: coupler response for flat insertion gain. In Acoustic Factors Affecting Hearing Aid Performance, G.A. Studebaker and I. Hochberg (Eds.) Baltimore: University Park Press.
Mueller, H.G. (2001). Probe-microphone measurements: 20 years of progress. Trends In Amplification,5(2), 3-39.
Mueller, H.G. & Picou, E.M. (2010). Survey examines popularity of real-ear probe-microphone measures. Hearing Journal, 63(5), 27-32.
Sanders, J., Stoody, T., Weber, J. & Mueller, H.G. (2015). Manufacturers’ NAL-NL2 Fittings Fail Real-ear Verification. Hearing Review, 21(3), 24.
Continued and its subsidiaries provide professional education authored by qualified Subject Matter Experts for continuing education purposes. These materials are intended for educational purposes and do not constitute medical advice or a substitute for individual clinical judgment. Continued is not a clinical healthcare provider; the licensed professional is solely responsible for ensuring that the application of any techniques or information presented is within their legal scope of practice and jurisdictional requirements.
