
Interview with Amanda Cerka Mroz, Au.D., CCC-A, Otometrics

Amanda Cerka Mroz
CAROLYN SMAKA: Hi Amanda, nice to speak with you today.
AMANDA CERKA MROZ: Great to be here, Carolyn.
SMAKA: Our topic today is maximizing the patient experience using PC-based audiometry. I always thought PC-based audiometry had benefits for the professional;I never thought about benefits to the patient. How does PC-based audiometry benefit the patient?![]()
MROZ: One of the main benefits of PC-based audiometry for the patient, and this benefit extends to the professional as well, is in patient retention of information.
Dr. Robert Margolis has done work on what patients remember during counseling. He reviewed healthcare literature and found that overall patients remember about 50% of the information their provider tells them (Margolis, 2003). In addition, he cites another study that indicates of the information patients do remember, only half is remembered correctly. This means that patients really only correctly remember about 25% of what we tell them.
Those of us who have worked in a clinic know how important this area is - misunderstanding clinical information can lead to a lack of follow-up, unrealistic expectations, misuse or nonuse of amplification and overall dissatisfaction. When patients understand the information we communicate to them, there is more potential for compliance with recommendations, better outcomes, higher satisfaction and greater efficacy of treatment.
PC-based audiometry can have a significant impact in this area. They say a picture is worth 1,000 words. Dr. Margolis (2004) indicates that patient recall can be enhanced by supplementing verbal information with written and graphical material such as cartoons and pictures. On a PC, you can add displays to the patient's test results, for example, what is the normal range of hearing and what is usable and unusable for the patient based on their audiogram. You can also look at results from both ears together if everything's symmetrical, or choose to display the ears separately to point out differences between them. Some patients really connect with the speech sounds;most adults can look at the speech sounds overlaid on an audiogram and see, "Okay, the /sh/ sound is up here." Visual learners, or perhaps those patients whose first language is not English, might prefer pictures. On a PC-based audiometer, you can display the pictures of familiar sounds on the audiogram and show patients how their hearing compares to sounds such as an airplane, for example. You can customize the information based on each patient's individual needs, simply by a few clicks of the mouse.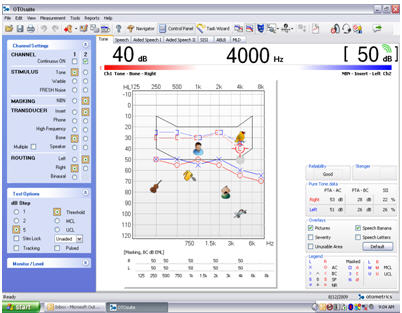
Familiar sound pictures superimposed on the speech banana is an example of how on-screen overlays can be used to enhance patient counseling.
SMAKA: I'm thinking of how we have our drawers crammed full of those plastic overlays that get bent or dirty. Or, we keep copies of the audiogram of familiar sounds, and it gets kind of worn and a little crooked on the sheet because it's been copied so many times. Using a PC-based audiometer for this purpose seems more efficient and professional.
MROZ: Exactly. It promotes professionalism, which benefits all of audiology. How does it look to the patient as you're digging through your drawers or file cabinet, as compared to walking over to your computer and clicking to select the overlay you want?
Another great way to use PC-based audiometry to enhance your professionalism, and the patient experience overall, is by the use of a second monitor with a touch screen in the sound booth. So, your computer resides in the testing area, and there is a second monitor in the sound booth that you can flip on to bring up all the patient's test results on a colorful screen. With a simple touch or by using a stylus, you can click those overlays on or off or maybe bring up a previous audiogram to compare. Think of someone who may be going through chemotherapy and is undergoing ototoxicity monitoring to determine if their hearing is worsening. That individual wants to see a comparison of hearing thresholds as soon as possible. With a touch screen in the booth, you can compare today's results with previous results while you're counseling. It displays the results in a clear, basic way that's also colorful and engaging.
A clinician at one of our sites was telling me about how they use the Astera and the OTOflex immittance device in their clinic. After they talk about the audiometric results on the touch screen in front of the patient, they get out the immittance bridge and they just keep talking the patient through the process as the patient watches the results of the testing on the screen. It demystifies the process, and engages the patient. It's very seamless and very easy to pull the patient in and to keep their eye contact because you're not constantly looking down and doing things they can't see.
SMAKA: It seems like it makes the patient more of an active participant in the process.
MROZ: Exactly;that's what keeping the patient engaged is all about.
I'll give you another example from a colleague who is a consultant with Otometrics and uses our PC-based audiometer with the Probe Microphone Measurement System. She feels that by having the audiometer and probe mic system all PC-based she can keep the patient more engaged in the process. She works at her computer, and uses a second large monitor screen behind her. She seats the patient across the desk from her so that the patient sees exactly what she's doing by watching the large screen while she explains it to them. They watch as she pulls up the audiogram from her networked NOAH software and she counsels them about how she will use the audiometric data to fit a hearing aid. The visual information reinforces the verbal message. Again, it demystifies the process and as you said, keeps the patient actively engaged in treatment.
PC-based technology has flexible set-up configurations that allow clinicians to network computers and counsel patients from more than one computer monitor.
Another clever thing you can do if your PC-based system includes a hearing loss simulator is display the audiogram results in dB SPL right from the initial counseling session. Typically, we counsel the patient about their audiogram in HL, and then conduct our hearing aid fitting and verification in SPL. It's very confusing to the patient when we flip things around. At the diagnostic session we teach them that normal hearing is up at the top of the graph and their hearing levels are below. Then, a few weeks later, we bring them back for a hearing aid fitting and say, "Okay, now here's normal and it's at the bottom of the graph and here's the amount of sound I'm trying to give you so we can be above your thresholds."
With a PC-based system that includes a hearing loss simulator, you can use an SPL view from the initial session. You can display the patient's audiogram in the hearing loss simulator and avoid the confusion of flipping from an HL to SPL explanation of hearing loss.
SMAKA: You know, sometimes I think the SPL view makes more intuitive sense because we're aiming up to hit targets.
MROZ: Right. Now, that's kind of getting a little deeper than just PC-based audiometry;that's using a whole PC-based platform. In our case, the OTOsuite Software provides an audiometry module, an immittance module, and a counseling and simulations module that includes speech mapping. If you're using NOAH and another PC-based probe mic system, you could also work that to your advantage by pulling up the audiometry data from OTOsuite into another manufacturer's hearing loss simulator and you could counsel that way. It's interesting to think about the different ways you can use the PC to your advantage with the other equipment, tools and resources you have in your practice. It's no longer just x's and o's on a piece of paper with a blue and a red pen.
SMAKA: You mean no more having to re-write audiograms because you picked up the blue pen when you were testing the right ear?
[laughter]
MROZ: Right!
You know, things are much more streamlined when you can use the PC and it prints off beautifully every time.
Speaking of printing results, Margolis indicates that to support retention, patients should be given written information, even when you think they've absorbed everything. I think as audiologists, most of us are already providing patients with written results, but think of how much easier and effective this can be with PC-based audiometry.
With PC-based audiometry, you can use the report template options to customize your reports for the patient. For some patients, maybe that means just using the template with the basic audiogram and an overlay showing the levels of hearing loss severity as you had discussed in your counseling session, along with some simple notes that you've typed along the top. Now the patient has a visual tool to use as show-and-tell with the rest of the family as well as a simple summary to refer to later.
Then, once they leave, you can print out a different template that doesn't include the severity overlay but does include speech testing results. You can then write a more extensive report along the top. Perhaps the physician likes the results of each ear separately so you would choose the template that displays right and left ears separately on your report. You're not changing any of the results, but you're choosing a report template that is most appropriate for the intended person.
SMAKA: It's funny, as you were saying that I was thinking about the times I looked at a handwritten audiogram and was like "Hmm, is that bone symbol on the line or between the lines? Because if it's here we kind of have an air bone gap but if it's here we don't." PC-based audiometry does away with those little errors and inaccuracies that handwritten results can cause.
MROZ: That's true. Along those same lines are problems with Xeroxing and faxing. How many times do you make a copy of an audiogram and find it gets progressively harder to read because you've copied it so many times, or you've made a copy of a copy of a copy?
Or received faxes of audiograms that are nearly impossible to read? With PC-based audiometry, you can print a clean copy of your test results each time, and you can also save your reports to PDF before you even print a hard copy. Even if you're not officially using an electronic medical record (EMR) yet, you can just make a PDF and keep your own electronic records. Then instead of Xeroxing or faxing a report to a physician, you could send a nice clean, clear PDF via email. It's very professional.
SMAKA: You mentioned several benefits of the PC-based system from the initial diagnostic session through reporting. Overall, it seems that would enhance the whole patient experience.
MROZ: I agree. A PC-based audiology office could make the difference between simply relaying test results and having an impactful consultation.
Think about the patient purchasing hearing aids. You're asking them to make a significant investment in hearing aids. When they walk into your clinic and they can see you value technology and you're comfortable using it in your everyday dealings with patients, it will seem logical that they'll be investing in a pair of high-tech hearing aids that you'll be programming on your computer. It really instills confidence that you know what you're doing. You've created a professional, state-of-the-art experience from your first appointment with the patient.
SMAKA: For the Baby Boomer and the younger demographic, I would think this technology in the office would be expected.
MROZ: That's a good point. The same test results and outcomes could be achieved by either method but you're going to have a much lower patient perception of the experience if you're hand writing the audiogram and manually inputting it into your computer for programming. The norm now is computers doing everything. The Snellen eye chart is no longer a chart. It's a projection on the wall, and the optometrist can select whatever display they need for each patient with the click of a mouse.
SMAKA: Exactly. I go to a network of medical providers, and with a click of the mouse, they can look at my results from any provider in their network, bring it up on the screen to discuss with me, connect to my pharmacy, etc.
MROZ: And we should all be providing the same kind of patient experience.
That brings up something a little more complex but an excellent use of PC-based audiometry, and that's networking within a practice. You can access audiometry through NOAH in one room, and then you can move the patient to another room. In the second room, you can open up NOAH on your networked computer, bring up the same patient data, and go through the whole counseling process with all the same results at your fingertips. And then you're ready to go into the NOAH fitting module and customize a hearing aid fitting without any duplication of effort - you can't do that with paper and pencil.
SMAKA: We had Gyl Kasewurm on the site a few weeks ago, and she cited a study (Wong, Hickson & McPherson, 2009) that found patient satisfaction ratings were influenced more by the way that patients were treated than by the performance of their hearing aids. I think it speaks to the fact that we need to look at the whole patient experience.
MROZ: Yes, that's a good point. As healthcare becomes more and more consumer-driven, the audiologists who provide the best patient experience will be the ones who bring the most patients into their clinics.
Along those same lines, the most recent MarkeTrak indicated that patients who had more counseling did better with their hearing aids, regardless of the kind of hearing aids they received. It's a matter of spending time engaging with the patient. If you have saved even five minutes by using a PC-based audiometer because everything's all cued up for you when you're ready to test, then you can use those five extra minutes for counseling, administering the COSI, or even asking them how their day was. That gets back to the memorable experience, and eventually to better outcomes - getting patients to wear their amplification and benefit from the treatment we provide.
SMAKA: Amanda, after our conversation today, I wonder why everyone isn't already using PC-based audiometry?
MADSEN Astera is a clinical audiometer that combines the best of traditional audiometry with the best of PC based audiometry.
MROZ: Our PC-based audiometer, the MADSEN Astera, has been very successful. We have the audiometer control panel that mimics the traditional interface and so it's very comfortable and it's very easy and quick to learn. You can sit down at it and it looks like an analog device. But you know, times are tough and when an older piece of equipment goes down, sometimes the thinking is that the easiest thing to do is to try and replace it with the same thing. What better opportunity to move ourselves forward as a profession than to use new technology to our advantage?
Another question we hear is, "Is PC-based technology going to be outdated much sooner than an analog audiometer? In reality, analog audiometers are working off of a PC chip which is generally pretty old. Think about how quickly hearing aid technology changes. How often do we expect our patients to have to replace their hearing aids - 5 years? Then why do we expect our audiometer technology to not be obsolete after 20 years?
SMAKA: Are upgrades possible with PC-based audiometers?
MROZ: Absolutely. Astera has been out for roughly two years and we've had three or four software upgrades in that time. We've taken customer input, and as we're making changes to the platform to add new languages and such, we've been able to incorporate some of the customer input into new enhancements. Software upgrades can incrementally improve your audiometer without having to buy a new one. In the future, we could even envision optional upgrades or modules with further speech tests or specialty tests, for example. With a non-PC-based piece of equipment it tends to be, drop it off, plug it in, and you're stuck with that version for as long as you own that equipment.
SMAKA: Where should we refer readers for more information on Astera and PC-based audiometry?
MROZ: I would refer readers to our website, www.otometrics.com or to the dedicated Astera website, myaudiometer.com.
SMAKA: Thanks, Amanda, great speaking with you as always!
MROZ: Thanks for having me, Carolyn.
For more information about Otometrics, visit the Otometrics web channel on AudiologyOnline.
References
Margolis, R. H. (2004, August 03). Boosting memory with informational counseling: Helping patients understand the nature of disorders and how to manage them. The ASHA Leader.
Margolis, R.H. (2004, January 24). Informational counseling in health professions: What do patients remember? Retrieved December 14, 2010 from www.audiologyincorporated.com
Wong, L.L.N., Hickson, L., & McPherson, B. (2009). Satisfaction with hearing aids: A consumer research perspective. International Journal of Audiology, 48(7), 405-427.

