
Interview with Donald Schum, Ph.D., Vice President of Audiology & Professional Relations, Oticon

Don Schum, Ph.D.
CAROLYN SMAKA: This is Carolyn Smaka, and I'm talking with Dr. Don Schum, Oticon's Vice President of Audiology and Professional Relations.
Our topic today is a new product release from Oticon, Intiga, and research they have done on first-time hearing device users. Tell me about why Oticon conducted this survey of first-time users - what was the goal?
DON SCHUM: Oticon commissioned a web-based survey by Decision Labs of more than 1,400 adults in US, Canada, Germany, France and Italy. This included , both people who currently wore hearing devices, and those who suspected that they had hearing loss but had not yet entered the hearing device process.
SMAKA: What were the key findings?
SCHUM: There were many. One of the interesting facets to the data was the amount of time it took for people to take action. We classically talk about patients taking an average of seven years between the time they first notice hearing loss and when they actually take action. In our study, over half of those surveyed stated that they took action within the first three years of noticing their hearing loss. But another large group took ten years or more to enter the process. So seven years is truly an average.
This timeframe reflects a bimodal distribution rather than a bell curve. When a hearing loss is suspected, some people take action very quickly and some people wait a very long time before taking action.
SMAKA: Are there any differences between those two groups?
SCHUM: Yes, someone who notices a problem and takes action relatively quickly is approaching the problem differently than someone who is resistant to doing anything and waits 10+ years to take action.
When we consider first-time users, we find there is not a single profile of a typical first-time user. While there are some typical behaviors that may occur with first-time users, they are not the same behaviors in every individual.
The study also confirmed our traditional notion of the stigma associated with hearing loss and hearing aids. Patients are concerned about what a hearing device says about them. We also discovered that some patients are genuinely concerned about the time, effort and cost to get amplification. Oftentimes we may think this is just a cover story or excuse, when the truth is the patient doesn't want to wear hearing aids. But based on statistical analysis of our data, there are some patients who truly think there will be a lot of appointments, it will be a hassle, the hearing devices may not work as expected and it will cost a lot of money. They don't want to invest the personal resources in the whole process at this point in their life.
As professionals we have to consider that patients may resist hearing devices for very different sets of reasons, and adjust our processes accordingly.
SMAKA: The first thing that stood out to me when I reviewed this research is the term "at-risk". Don, what does it mean that first time users are always 'at-risk'?
SCHUM: The term 'at-risk' refers to the hearing device fittings with first-time users. Typical first-time users come in with a level of motivation to use hearing instruments that is often less than optimal. They most likely recognize that they have some hearing problems - or at least their friends or family may recognize that they're having hearing problems and encourage them to seek treatment - but they may not have totally come to terms with it. They may be very resistant to the idea of using the amplification for a variety of different reasons.
When someone says, "Sure, I'll try it" without the right mindset, the likelihood of failure - returns for credit, in-the-drawer hearing devices and dissatisfaction - is much higher. We want to focus on what it takes to get a person in a state we refer to as readiness. Success with hearing devices is driven, in part, by the person's level of motivation, cooperation and willingness to contribute to the whole fitting process. Readiness refers to the state of mind in which the likelihood of success with hearing devices is highest.
When we talk about Readiness Management techniques, we are not drawing not only from ideas that we have at Oticon, but also on the experience of many, many clinicians from around the world. Our goal is not to make ground-breaking new statements about patient counseling, but rather to try to organize observations and techniques that have proven to work well in clinical interactions.
If there's any take-home message around readiness Readiness Management, it's that each patient is an individual and that the counseling approach has to be based on the individual concerns, attitudes and mindsets of each patient.
SMAKA: If first-time users are at-risk that the fitting may not be successful, what are some of the reasons why that might happen?
SCHUM: One thing that holds back potential new users is their own perception of a hearing device. They have an image of what a hearing device looks like, and it is usually outdated. They also have an image of what a hearing device wearer looks like, and it is typically an older person. When people are challenged with the reality that their hearing is failing, that it may be age-related, and that the most effective treatment is amplification, they have trouble putting these two sets of realities together.
Although professionals focus on what went wrong with the fitting, oftentimes the first problem is simply that the patient doesn't see themselves as a hearing device wearer. As a result, anything negative that may occur in the fitting, even if it seems minor, tends to drive the fitting to a bad place. It could be that the patient has unrealistically high expectations. Perhaps the patient approaches the process as a consumer of a retail electronics purchase and not as a patient entering a health care process. In "consumer-mode", the patient may be very focused on features and benefits, striking the right deal and getting what he/she paid for, which is very helpful when making purchases as a consumer. However, if the professional is approaching the fitting as a health care issue, and making recommendations to improve the patient's quality of life, the two differing viewpoints may result in discussions that are not productive for either party.
Of course, sometimes a fitting simply does not go well. The settings are not adjusted well, the patient has side effects such as feedback or occlusion, or maybe there is not enough perceived benefit from amplification early on in the process. While all of these things can be challenges, they become more of a problem when the patient is not fully committed to the process from the start. If patients are not fully ready, they may not have the patience or the willingness to work with the professional to find a solution.
SMAKA: How does a clinician go about getting to the bottom of each patient's individual barriers?
SCHUM: One of the first things that is helpful for the clinician to do is to understand what is holding patients back. What is their set of concerns? To help hearing care professionals frame the mindset of the patient, we have created different categories of concerns that patients might demonstrate.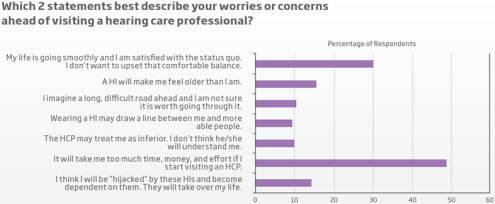
Responses of 749 non-users to the question, "Which 2 statements best describe your worries or concerns about visiting a hearing care professional?" from Oticon survey. For larger view, Click Here (PDF).
For example, the literature in other fields of healthcare that deal with older patients discusses the phenomenon of normalization. Normalization is when the patient says, "The health issue that I'm dealing with is 'normal for my age,'" meaning that it is an expected body change associated with aging. When confronted with a new health issue, these people will ask their provider "Is this something that's normal in someone my age?" Should they expect to have arthritis, vision loss, hair loss, sexual dysfunction, hearing loss, high cholesterol, etc.? When faced with an age-related body change, all they want to know is if it is normal. As soon as they're told that the issue is normal for their age, they tend to have a dismissive attitude, and believe they do not need to do anything about it.
The development of a clinically-significant condition like hearing loss may be in part age-related but that doesn't necessarily mean that the patient shouldn't be willing or interested in doing something about it. This is one example of a category of concern that you might see in a patient.
Another set of concerns that patients have entering the process is wariness about either hearing devices themselves or the process of being fit with amplification. As I mentioned earlier, our data show that some patients have a true concern that it is going to be a big hassle and a drain on their time, energy and possibly on their finances.
The third group of behavior is the classic conflicted behavior, when the patient says, "I know I'm having hearing problems, but I just can't accept the idea of using hearing devices as the solution." These patients are not dismissing their hearing loss but they won't wear hearing devices. They know they should do something but are unwilling to go for the most effective solution at this point in time. These are patients with whom the clinician's counseling skills come under fire, because you have to do the very best job you can to try to get them to a place where they're willing to accept amplification as a solution to the communication problems that they're having.
While these categories are not an end in and of themselves, they may help the clinician to recognize the true concerns that individual patients are expressing. When you start looking at individual concerns, you realize that the current person's concerns may be different than the person who was in your office an hour ago.
Identifying the different types of concerns that each patient has is only important if it also modifies the intervention approach that the clinician will use. Each concern needs to be dealt with in the appropriate way. For example, a patient who's wary or mistrustful about whether hearing devices will actually be a benefit should be getting a demonstration of hearing devices, either an in-office demonstration or an at-home trial. We want to show the person that hearing devices are a good solution for the hearing loss.
SMAKA: Going back to the issue of stigma, there are so many cosmetically-appealing devices on the market today. Why does this issue persist?
SCHUM: Stigma is a very important issue to discuss, because when we talk about the stigma of hearing devices, it's a self-imposed feeling that the patient has that, "If I wear hearing devices, what does that say about me? It says I'm old." The stigma is not related to whether or not a hearing-impaired individual is worthy or not, but it is about the symbolism that hearing devices carry - that is, if you wear hearing devices, your body has failed and you're older. This perception is what we believe is really holding people back. They're not comfortable with taking this tangible set of symbols, i.e., hearing devices, and putting them on every morning as a reminder that "My body has failed me. I'm getting older. I need help." Although it's a self-imposed stigma, it is still a stigma.
SMAKA: How can audiologists address this? Some issues are easy to address directly - cost, features, etc. But how do you address a perception or stigma that the patient is putting on himself or herself?
SCHUM: This is a challenge that draws upon the very best counseling skills that we have. For many patients, this is a major life change, and they need to come to terms with entering a new phase of their life. Clinicians who are too aggressive in the process may interact very poorly with this type of patient because they're not recognizing the emotional issue that the patient needs to work through before proceeding.
On the other hand, a clinician who's too passive may allow patients to continue to put off caring for their hearing. The key is to strike a balance between being sensitive to the emotional issue while not allowing the patient to minimize the problem, deny it or put off dealing with it.
One of the counseling approaches that has relevance to this issue comes out of the field of motivational interviewing. It is a counseling approach that developed ten years ago by two clinical psychologists, Miller and Rollnick. It focuses on helping individuals who need to make a behavioral change to improve their health uch as people with alcohol or drug addiction, smoking issues or weight loss issues but who are having trouble doing the things that are necessary to make that change.
We can draw upon motivational interviewing to help people who are so focused on the symbolism of amplification and what it says about them that they are having trouble moving forward. Motivational interviewing can help us to change patients' focus from the reasons why they want to stay where they are and not make a change to a focus on the good things that can happen in their life if they moved in the direction of amplification.
SMAKA: Where can professionals get more information about motivational interviewing?
SCHUM: Motivational Interviewing is a counseling approach that deserves an investment of time and energy to understand the specifics and to apply the techniques in an effective manner in the clinical setting.
The Ida Institute is a nonprofit organization funded by the Oticon Foundation, has created a great set of tools, two of which are called the Line and the Box that were very much inspired by concepts from motivational interviewing. They are designed to help patients who are having trouble dealing with the idea of hearing loss and coming to terms with it, in order to move them forward in the process. Information on these tools and the other resources that the Ida Institute has developed is available at idainstitute.com/
In addition, I presented an AudiologyOnline course entitled Motivating the Older Patient to Take Action, which goes into more detail about motivational interviewing. It's a very well-developed area of counseling, and I cannot really cover the entire topic here or even in the 1-hour seminar, so I'd encourage interested professionals to also visit www.motivationalinterview.org. There is an abundance of literature on the topic that clinicians can seek out for more information.
SMAKA: Oticon's new Intiga is billed as being "designed to meet the needs of first-time users." How does Intiga help to overcome some of the first-time user barriers we've been discussing?
SCHUM: From the initial meeting where we sat down to put together the feature set, we approached Intiga from the perspective of a first-time user. For example, we noticed that all hearing device fitting rooms have a mirror, and that's because the very first thing that a first-time user wants to know about their new amplification is how it looks.
So we started our design and development process by addressing the appearance. Intiga is our newest RITE product in Oticon's design category. First in this category was Delta, followed by Dual, and now Intiga. The shape of the device, the finish, the way the receiver wire is connected, the lack of external switches, the way the battery door discretely works into the body of the product, down to the colors it is offered in, all increase the acceptance on the part of first-time users so they can see themselves wearing it. We did everything possible to ensure that the appearance was such that patients could easily accept Intiga into their life.
Intiga's appearance is designed for immediate acceptance both on and off the ear.
Next, we considered the first-time user's experience with both the fit and the amplified sound. This is very important. From the first few minutes of wearing the hearing devices through the first day or so, what is the experience, i.e. how does it sound? How does it feel in the ears? In our development, we focused a great deal on the fit and the signal processing to ensure that patients experience nothing negative during their first wearing experience. We know that this is critical to acceptance. Most clinicians have had the experience in which a first-time fitting fails because the patients were surprised when the dog barked or the door slammed, or they heard other sounds they weren't expecting. These types of experiences can throw a first-time user off, and we wanted to minimize the likelihood of that happening.
There is a difference between a successful fitting and a successful first fit. The long-range goal of the audiologist is to provide a good audiological solution for patients based on their hearing loss and hearing needs. But that doesn't mean all has to be achieved on the day of the initial fitting. The most important thing on the day of the fitting is that patients are comfortable with what they're getting. It looks good, it sounds good, and they are comfortable giving it a try. There is time to make adjustments to the fitting to make it the best possible audiological solution for the patient, but there may not be time to correct a negative first impression if the patient rejects amplification. So with Intiga, we wanted to provide an immediate positive sound and tactile experience. We call this the "now" effect.
We also have to consider the benefit the hearing devices provide;they have to help the patient. While the highest priority on Day 1 is how the hearing devices look, how they feel, and the initial sound experience, once the patient gets comfortable with those things, it's all about how the signal processing solves the patient's listening problems. This was another important consideration for us in the development of Intiga.
SMAKA: I'm going to guess the Adaptation Manager has something to do with this?
SCHUM: It absolutely does. Oticon pioneered the use of adaptation management back in the late '90s when we released Digifocus. It was based on the philosophy that there's a difference between a good fitting and a good first fit. Our idea was that over the course of the first month or so the hearing device should be increasing the amount of amplification and gradually introduce more and more sound until it's providing the full prescribed settings. With Intiga, we determined the changes we could make with the Adaptation Manager that to make the first several weeks of hearing device use even more acceptable and more positive. The primary change was in the initial settings of the product that we call Step 1. These are the "going-out-the-door on the first day of the fitting" settings, and they are not intended for long term use. In Step 1, we've increased the amount of amplification for conversational speech but in many cases, reduced the amount of amplification for very soft sounds and very loud sounds in the environment.
Again, our goal is to make sure that patients are not experiencing any surprising or adverse sounds in their environment, while providing more gain for speech. We believe that patients tend to verify the performance of the device within the first few days based on face-to-face conversations they have, typically with their friends or family members.
SMAKA: Can Intiga be used with existing hearing device wearers?
Oticon Intiga comes in three performance levels to meet a wide range of needs and lifestyles: Intiga 10, 8 and 6. All are ConnectLine enabled for wireless connectivity.
SCHUM: Absolutely. We wanted to ensure that Intiga was right for patients who are wearing amplification and upgrading or replacing what they currently have as well. There are patients who were fit, for example, with design-based products such as Dual or Delta or those from other manufacturers, and are ready for new hearing devices. Intiga would certainly be a good choice for them. Intiga is built on the RISE 2 platform and includes technology that is as sophisticated as we've ever developed, especially in the top tier, Intiga 10. It includes Speech Guard, Spatial Sound technologies, wireless connectivity, and a host of other features designed for maximum performance.
SMAKA: Thanks for that overview of Intiga, and for more information, readers can visit www.oticonusa.com. Where can readers find more information about the survey?
SCHUM: We will publish various aspects of the study in a series of white papers that we'll be releasing over the next several months. The parts of that data set that are relevant to what the patient expects out of amplification and their hesitancies about taking action that we discussed today will be in an upcoming white paper on Readiness Management. Parts of the data that refer to what it takes to attract a patient to a practice will be in a white paper that's focused on traffic-building activities. This data set is huge and there are other white papers planned. There are so many good nuggets that we want to ensure that when we publish them we put them in context and make their relevance and importance very clear to professionals.
SMAKA: That sounds great. We'll look forward to those white papers. Thanks so much for all your time today, Don. It's been a pleasure.
SCHUM: Thanks for having me.
For more information, please visit www.oticonusa.com or the Oticon Web Channel on AudiologyOnline.


Donald J. Schum, PhD
Vice President of Audiology and Professional Relations, Oticon
Don Schum currently serves as Vice President for Audiology & Professional Relations for Oticon, Inc. Previous to his position at Oticon in Somerset, Don served as the Director of Audiology for the main Oticon office in Copenhagen Denmark. In addition, he served as the Director of the Hearing Aid Lab at the University of Iowa, School of Medicine (1990-1995) and as an Assistant professor at the Medical University of South Carolina (1988-1990). During his professional career, Dr. Schum has been an active researcher in the areas of Hearing Aids, Speech Understanding, and Outcome Measures. (B.S. in Speech & Hearing Science, University of Illinois M.A. in Audiology, University of Iowa Ph.D. in Audiology, Louisiana State University.)