
Patients with severe and profound hearing loss can be challenging to fit with amplification. Furthermore, our experience tells us that many of the advanced features implemented in modern hearing aids do not always adequately address the unique characteristics of severe hearing loss. This review article will attempt to unravel some of the issues associated with fitting severe hearing loss by examining recent clinical studies. Specifically, this article provides the busy audiologist with a brief yet substantive review of new and emerging trends in hearing aid selection and fitting as they relate to adults with severe hearing loss. Some of the latest technology designed to address the unique nature of severe hearing loss, such as frequency lowering, bimodal arrangements, and hybrid cochlear implants will also be reviewed. The reader will be able to take away practical hearing aid selection and fitting tips, or "clinical nuggets," that will contribute to greater clinical success in his or her daily practice.
Anecdotally, we know that patients with a severe hearing loss comprise a relatively low number of the total patient base for the typical clinical audiologist. Margolis and Saly (2008) described a database with over 23,000 records and only 10% were patients with severe to profound hearing loss. The relatively low percentage of patients we see with severe to profound loss is likely related to the fact that some have cochlear implants and others have decided to become part of the Deaf community. Although the typical practice's database consists of a relatively low number of patients with severe hearing loss, patients with severe to profound hearing loss using hearing aids depend on their devices more than individuals with a mild to moderate loss.
Although patients with severe to profound hearing loss only comprise about 10% of the typical clinic's workload, approximately 106 million people worldwide have a severe-profound hearing loss. Somewhat surprisingly, it has been reported that 50% of patients with severe loss use hearing aids, whereas 37% with a profound loss use hearing aids. (Global Strategic Business Report. October, 2005). Given the prevalence and penetration rates for this degree of loss, there appears to be an opportunity for addressing the unique needs of this population with new and improved technology.
The Fundamentals of Severe-Profound Hearing Loss in Adults
For discussion purposes we will focus on two different types of severe hearing loss commonly encountered in the clinic (Figure 1). Type 1 severe hearing loss is primarily in the high frequencies with normal or near normal thresholds in the low to mid frequencies. Type 2 severe hearing loss has a flat audiometric configuration. These labels are not used in the pertinent literature;however, they are used here to distinguish between significant clinical differences in types of severe hearing loss. As such, even though both types have many commonalities, the technology solutions for each type can sometimes vary significantly. 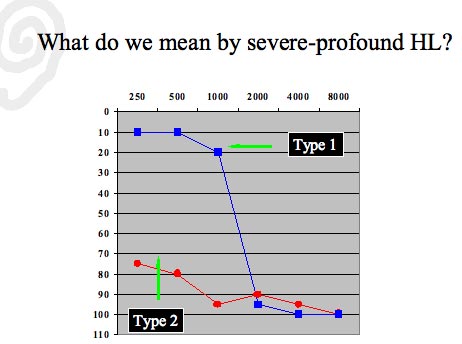
Figure 1. Two general types of sensorineural hearing loss discussed in this review article.
Regardless of the configuration of the severe hearing loss, there are several similar characteristics, such as broad auditory filters and poor speech understanding in background noise associated with a severe loss. Many of the unique traits associated with severe hearing loss are directly related to inner hair cell (IHC) damage. According to many published reports, IHC loss is present with pure tone thresholds of greater than 60 dB HL (see Turner, 1999 for a review). Recall that IHCs are tonitopically arranged on the basilar membrane and directly connected to the auditory nerve;therefore, it is believed that IHC damage results in auditory distortion. This distortion may be reported as "hissing" or "cracking" during pure tone testing. More precisely, damage to the IHCs is likely to result in poor word recognition scores and off-frequency listening.
Another hallmark of severe to profound hearing loss, which must be carefully considered when fitting hearing aids, is that it is very restricted, or it creates a narrow dynamic range. Because amplified sound needs to be placed into this restricted dynamic range, fitting patients with a severe loss is challenging. Compared to mild and moderate hearing loss, the audiologist has less residual dynamic range to place the important sounds of speech. For an example of the difference in residual dynamic range between a severe and mild to moderate hearing loss see Figure 2. 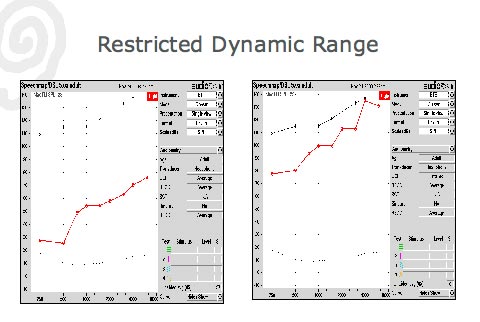
Click Here to View Larger Version of Figure 2 (PDF)
Figure 2. The residual dynamic range for a mild to moderate loss (left) compared to a severe hearing loss (right).
Another fitting challenge associated with a severe loss is poor speech understanding ability. Although speech understanding ability varies among adults with severe sensorineural hearing loss, there is a clear trend indicating that, as a whole, those with severe hearing loss have a difficult time understanding speech in quiet and noisy listening conditions. Compared to a mild to moderate loss performance-intensity (PI) functions for those with a severe hearing loss are quite steep, indicating that speech intelligibility is maximized within an extremely narrow intensity range. This steep PI function, which is often associated with severe loss on the audiogram, is illustrated in Figure 3. 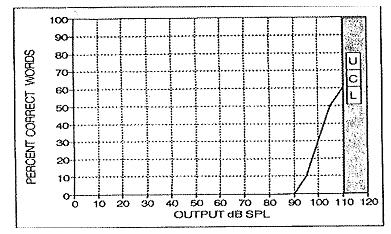
Figure 3. An example of a steep performance-intensity function for a severe loss. From Killion, M. & Fikret-Pasa, S. (1993). The 3 Types of sensorineural hearing loss: Loudness and intelligibility considersations. Hearing Journal (46)11, 31 -36. Reprinted with permission of The Hearing Journal and its publisher, Lippincott Williams & Wilkins.
Clinical Nugget: Research (e.g., Ching, Dillon, Katsch and Byrne, 2001) indicates that there is a wide range in performance on speech tests for patients with severe hearing loss, necessitating the need for careful testing using valid speech audiometry procedures.In the next section we turn our attention to one of the underlying components of severe loss, cochlear dead regions. Although not the sole characteristic of severe loss, cochlear dead regions are believed to present fitting challenges.
Cochlear Dead Regions
The complete loss of IHC function confined to a specific location along the basilar membrane is known as a cochlear dead region. These regions do not detect pure tones during routine audiometry;rather, adjacent regions of the basilar membrane are stimulated during pure tone testing. It is the response of these off-frequency regions of the basilar membrane that are recorded during routine pure tone threshold testing, which may be reported by some patients as 'hisses" or "cracking" sounds.
The existence of dead regions has been reported in the literature for more than a decade;however, a review of the literature suggests that the reported prevalence of dead regions varies. Vinay and Moore (2007) report a 59% chance that patients with hearing loss greater than 70 dB HL in the high frequencies have a cochlear dead region. Markessis, Kapadia, Munro and Moore (2006) suggest that 87% of adults with a steeply sloping moderate to severe hearing loss met the criteria for a dead region for at least one frequency. On the other hand, Preminger, Carpenter and Ziegler (2005) report that 29% of adults with a moderate to severe hearing loss had a dead region. This variability in prevalence data for adults with moderate to severe hearing loss is likely related to the differences in criteria used to measure dead regions using the Threshold Equalizing Noise (TEN) test.
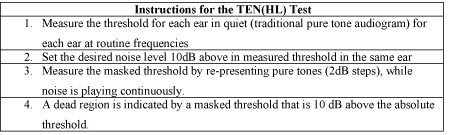
The TEN test is considered to be the gold standard for checking for dead regions in the clinic. Specifically, the TEN(HL) test, which can be obtained on CD directly from Brian C.J. Moore at the University of Cambridge in the United Kingdom, can be used to identify dead regions. According to the TEN(HL) instructions, the test can be completed in approximately 10 minutes. See Table 1 for a review of the TEN(HL) instructions.
Click Here to View Larger Version of Table 1 (PDF)
Table 1. Instructions for the TEN(HL) test
Based on a systematic review of the evidence, cochlear dead regions can occur at any frequency, but they are more likely to occur in the high frequencies at thresholds greater than 85 dB HL and when the slope is more than 40 dB per octave. This trend would indicate that many patients with suspected dead regions on the audiogram could be classified as having a Type 1 severe hearing loss, in which the severe loss is confined to the high frequencies. Considering the milder hearing loss in the low frequencies, patients with a Type 1 severe hearing loss described here should be managed differently than a Type 2 severe hearing loss.
Although cochlear dead regions are thought to be found in one-third to two-thirds of patients with severe hearing loss, there are two pragmatic questions for the busy clinical audiologist: 1) Do I need to use the TEN(HL) to identify dead regions? and 2) If I suspect a dead region, how does that change my hearing aid selection decision?
There is some debate regarding the clinical value of conducting a specific clinical test to identify cochlear dead regions. Summers (2004) suggested that experienced clinicians were as just as proficient at accurately identifying cochlear dead regions by looking at the thresholds of the audiogram compared to their interpretation of the results of on objective test used to find dead regions. Recently, however, Azah & Moore (2007) concluded that using the TEN (HL) test accurately identified several patients with dead regions that may have otherwise been missed by simply relying on the audiogram to find a dead region.
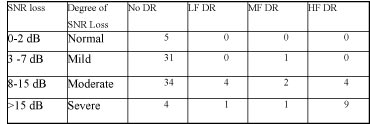
In one study, Preminger et al. (2005) compared 14 subjects with confirmed dead regions to 25 subjects without dead regions. All subjects in both groups had pure tone thresholds between 50 and 85 dB HL. Results of the study indicated that the majority of subjects with a confirmed dead region had severe SNR loss as measured on the Quick SIN (Table 2). Results of this study would suggest that the Quick SIN might provide some helpful insights into the identification of patients with possible cochlear dead regions.
Click Here to View Larger Version of Table 2 (PDF)
Table 2. The degree of SNR loss for those with no dead regions (No DR) compared to subjects with confirmed low frequency (LF), mid frequency (MF), and high frequency (HF) hearing loss.
Clinical Nugget: Although the TEN(HL) test is valid and useful, the Quick SIN can be used to screen for dead regions.Preferred Compression Parameters and Frequency Response for Severe Losses
Whether a dead region is carefully measured with the TEN(HL) test or suspected based on the Quick SIN score, an important consideration for any severe hearing loss is fine tuning the gain and frequency response of the hearing aids. Although some research indicates that providing amplification beyond the dead region is beneficial, other research indicates that limiting the gain for sounds around the dead region is better. There is some evidence suggesting that many patients - regardless of a suspected dead region - do poorly when high frequency audibility is restored through amplification (see Turner, 1999 for a review);however, other studies call these findings into question (Hornsby & Ricketts, 2006).
Given these conflicting reports, one possible approach to managing the hearing aid selection process for patients with a precipitously sloping severe high frequency hearing loss is to offer them one program with a broadband frequency response restoring high frequency audibility and a second program rolling off gain for sounds around the suspected dead region. Gordo and Martinelli-Iorio (2008) compared one group of subjects with no dead regions to another group with confirmed dead regions. Both groups were fitted with modern hearing aids utilizing two memories. Memory 1 had a broadband frequency response and memory 2 had no gain above 2560 Hz. For subjects with dead regions, the high cut response in the second memory was preferred and both groups showed significant improvements on the APHAB.
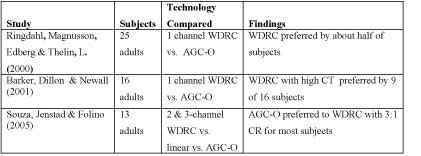
Clinical Nugget: If a high frequency dead region is suspected, fit the patient with a two-memory device, a broadband memory and a memory that rolls off amplification at about 2500 Hz. Allow the patient to choose the preferred gain and frequency response setting.Another important hearing aid fitting decision that needs to be made for adults with severe hearing loss is the type and amount of compression needed to maximize the audibility and comfort of amplified speech. Fortunately, there have been a number of studies examining compression preferences for patients with severe hearing loss. Table 3 reviews the key findings for three published studies for patients with severe hearing loss. Measures of patient preferences and speech recognition scores show no clear favorite among the three processing strategies compared.
Click Here to View Larger Version of Table 3 (PDF)
Table 3. Three studies comparing patient preferences for linear, AGC-O, and WDRC hearing aids for adults with severe hearing losses.
A review of the research indicates that there is no clear advantage for linear, AGC-O, or WDRC when fitting adults. Furthermore, these studies suggest that aggressive compression ratios are seldom preferred by adult subjects with severe hearing loss. Keidser, Dillon, Dyrlund, Carter and Hartley (2007) examined preferred compression ratios using a 2-channel WDRC with a compression kneepoint of 55 dB. Using a tournament approach, results suggested that the majority of subjects preferred linear amplification in the low frequency channel and a compression ratio of less than 2:1 in the high frequency channel. Given these findings, the clinician would be wise to choose a hearing aid with both WDRC and linear processing for soft and average input levels and to allow extra time to adjust the compression ratio.
Clinical Nugget: The preponderance of studies indicates that the majority of adults with severe hearing loss and previous hearing aid experience prefer compression ratios between 1:1 (linear) and 1.8:1.Frequency Lowering
Frequency lowering is another alternative for patients with severe high frequency loss. In simple terms, frequency lowering devices transpose high frequency sounds to a lower frequency region where there is less cochlear damage. Although by no means a new concept (the first clinical studies of frequency transposition were published in the 1970s), frequency lowering as implemented in modern hearing aids has enjoyed a resurgence in popularity the past few years, as there are currently three products commercially available employing some type of frequency lowering.
There are two different ways in which frequency lowering can be implemented in a modern hearing aid. One employs frequency compression and the second employs frequency transposition. Both types of frequency lowering schemes are available in a commercial hearing aid and are shown schematically in Figure 4. It is important to note that the most recent literature shows no advantage for either type of frequency lowering.
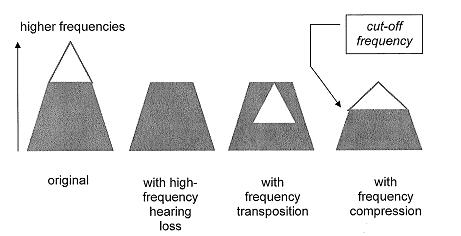
Figure 4. A schematic representation of two types of frequency lowering technology;high frequency information is represented by the open triangle. Adapted from Simpson, Hersbach & McDermott (2005).
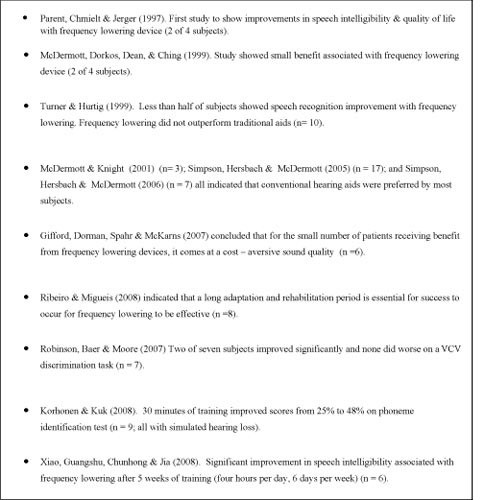
A detailed analysis of frequency lowering is beyond the scope of this review article;however, a review of the clinical effectiveness of frequency lowering in hearing aids for adults can be found in Table 4. Although frequency lowering holds great promise for adults, the preponderance of evidence suggests that the most current implementations of frequency lowering offer no additional benefit when compared to modern hearing aids without frequency lowering. For those adults that do benefit from frequency lowering, the evidence suggests that it comes at the cost of enduring aversive sound quality and an extended training period.
Click Here to View Larger Version of Table 4 (PDF)
Table 4. A review of the clinical effectiveness of frequency lowering in hearing aids for adults in peer reviewed literature.
Hybrid Implants
Cochlear implants have been a viable option for patients with a flat severe-profound hearing loss for decades. The majority of persons with severe hearing loss, however, are not candidates for cochlear implants because they have relatively good hearing in the low frequencies. Hybrid cochlear implants, which intergrate low frequency acoustic information with electrical stimulation of damaged high frequency regions of the cochlea, are currently undergoing clinical trials in the US. They soon may emerge as an option for patients with severe high frequency hearing loss (Turner, 2006).
Because hybrid cochlear implants allow the auditory system to continue to take advantage of low frequency voicing information, while concurrently improving high frequency hearing through electrical stimulation, they allow patients with severe high frequency hearing loss to overcome many of the distortional components associated with severe hearing loss. Turner, Gantz and Reiss (2008) reported that the Iowa/Nucleus Hybrid implant significantly improved speech recognition in noise relative to traditional cochlear implants. For more information on hybrid candidacy requirements, see https:// www.research.va.gov/programs/JRRD/45_5/turner.pdf
Bimodal Arrangements
Cochlear implants are an option for adults with severe to profound (type 2) hearing loss, and their effectiveness for the appropriate candidate is well documented. For patients with a bilateral severe to profound hearing loss, the typical approach is to fit a cochlear implant in one ear. For patients that opt for cochlear implantation, the benefits of binaural hearing remain elusive.
For patients who receive a cochlear implant in one ear and have residual hearing in the nonimplanted ear, binaural hearing can be achieved with a second implant or with a hearing aid in the opposite ear. Use of a hearing aid in the ear opposite an implant is referred to as a bimodal arrangement (Ching, 2005).
The objective of a bimodal arrangement is to provide the unilateral implant patient the benefits of binaural hearing. Over the past few years several studies (See Ching 2007 for a review) have indicated that localization and speech perception ability is improved in about 50% of the patients using a bimodal arrangement compared to those with a single cochlear implant only. The systematic review of the evidence by Ching (2007) suggests that bimodal fittings should no longer be considered as a special technique, but should be considered the management of choice for people who have one implant and a bilateral severe to profound hearing loss. Before a patient undergoes surgery for a bilateral cochlear implant, he or she must first undergo a trial with a bimodal fitting.
Clinical Nugget: Severe to profoundly deafened adults with bilateral impairment who currently wearing a cochlear implant in one ear are good candidates for a hearing aid in the contralateral ear. The success rate with a bimodal arrangement is approximately 50%., according to recent reports.Putting it all Together: Hearing Aid Selection Decisions for Severe Losses
For patients who are not cochlear implant candidates or are not interested in pursuing the option, there are many aspects of the hearing aid fitting that need to be carefully considered. One recently published retrospective study helps shed some light on hearing aid preferences for adults with severe or profound hearing loss. Keidser, Hartley and Carter (2008) investigated the long-term benefits of WDRC processing combined with directional microphones and digital noise reduction in adults with severe or profound hearing loss. The results of their retrospective study indicated that most of the subjects were satisfied with WDRC processing in everyday listening situations. In addition, the study found that benefit from the directional microphone and digital noise reduction was lower and more varied, thus suggesting that those features are best employed in the second memory.
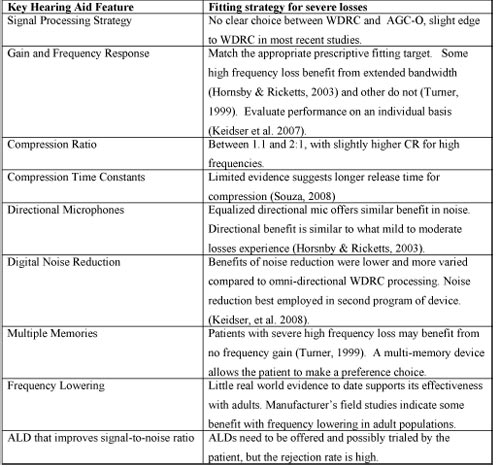
When the conscientious audiologist is making decisions in regard to setting the various electroacoustic parameters of the device, it is helpful to consider evidence that has been gathered in carefully controlled studies. Table 5 below is intended to summarize how various features can be selected and fine tuned when working with patients with severe hearing loss.
Click Here to View Larger Version of Table 5 (PDF)
Table 5. Summary of findings for fitting and fine tuning for severe loss.
Occam's razor
Occam's razor is a principle attributed to the 14th century English philosopher, William of Occam. Occam's razor states that the simplest solution is often the best solution for a complex problem. When it comes to selecting hearing aids for patients with severe or profound hearing loss, Occam's razor has some clinical utility. For example, basic principles like access to multiple memories, taking the time to set the preferred compression parameters, and getting the frequency response correct are simple, yet highly important factors contributing to the success of fitting patients with both types of severe losses outlined in this review article. Once these basic parameters are established value-added features like digital noise reduction and automatic program switching have the potential to make high gain devices easier to use in a wide variety of listening situations.
Occam's razor reminds us that we need to get the fundamentals right first (gain, compression and frequency response) using features that have been proven to give the severely impaired patient benefit in everyday listening situations before attempting to incorporate newer, more technically advanced features. Many of these newer features (frequency lowering, speech enhancement) have great potential, but as of today, have little or no evidence supporting their clinical effectiveness.
References
Azah, H & Moore, B. (2007). Dead regions in the cochlea at 4 KHz in elderly adults: relation to absolute threshold, steepness of audiogram and pure tone average. Journal of the American Academy of Audiology, 18(2), 97-106.
Barker, C., Dillon, H. & Newall, P. (2001). Fitting low ratio compression to people with severe and profound hearing loss. Ear and Hearing. 22(2), 130-141.
Ching, T., Dillon, H., Katsch, R. & Byrne, D. (2001). Maximizing effective audibility in hearing aid fitting. Ear and Hearing. 22(3), 212-224.
Ching, T. (2005). The evidence calls for making binaural-bimodal fittings routine. Hearing Journal. 58(11), 32-41.
Ching, T. (2007). Binaural-bimodal fitting or bilateral implantation for managing severe to profound deafness: a review. Trends in Amplification. 11(3), 161-192.
Chmiel, R. & Jerger, J. (1997). Factor analytic structure of auditory impairment in elderly persons. Journal of the American Academy of Audiology, 8(4), 269-76.
Gifford, R.H., Dorman, M.F., Spahr, A.J., & McKarns, S.A. (2007). Effect of digital frequency compression (DFC) on speech recognition in candidates for combined electric and acoustic stimulation (EAS). Journal of Speech, Language and Hearing Research, 50, 1194-1202.
Gordo, A. & Martinnelli-Iorio, M. (2007). Dead regions in the cochlea at high frequencies: implications for the adaptation to hearing aids. Rev. Bras. Otorrinolaringol, 73(3).
Hornsby, B. & Ricketts, T. (2003). The effects of hearing loss on the contribution of high and low frequency speech information to speech understanding. Journal of the Acoustical Society of America, 113,(3), 1706-1717.
Hornsby, B. & Ricketts, T. (2006). The effects of hearing loss on the contribution of high and low frequency speech information to speech understanding. II. Sloping hearing loss. Journal of the Acoustical Society of America,119 (3), 1752-1763.
Keidser, G., Hartley, D. & Carter, L. (2008). Long-term usage of modern signal processing by listeners with severe or profound hearing loss;A retrospective survey. American Journal of Audiology,17( 2), 136-146.
Keidser, G., Dillon, H., Dyrlund, O., Carter, L., Hartley, D. (2007). Preferred low and high frequency compression ratios among hearing aid users with moderately severe to profound hearing loss. Journal of the American Academy of Audiology, 18(1), 17-33.
Korhonen, P. & Kuk, F. (2008). Use of frequency transposition in simulated hearing loss. Journal of the American Academy of Audiology,29, 6.
Margolis, R. & Saly, G. (2008) Distribution of hearing loss characteristics in a clinical population. Ear and Hearing, 29 (4), 524-532.
Markessis, E., Kapadia, S., Munro, K.J., & Moore, B. (2006). Modification of the threshold equalizing noise (TEN) test for cochlear dead regions for use with steeply sloping high-frequency hearing loss. International Journal of Audiology, 45, 91-98.
McDermott, H.J., Dorkos, V.P., Dean, M.R., & Ching., T.Y. (1999). Improvements in speech perception with use of the AVR TranSonic frequency-transposing hearing aid. Journal of Speech, Language, and Hearing Research, 42, 1323-1335.
McDermott, H. & Knight, M. (2001). Preliminary results with the AVR ImpaCT frequency-transposing hearing aid. Journal of the American Academy of Audiology, 12(3), 121-127.
Parent, T.C., Chmielt, R. & Jerger, J. (1997). Comparison of performance with frequency transposition hearing aids and conventional hearing aids. Journal of the American Academy of Audiology, 8, 355-365.
Preminger, J., Carpenter, R., Ziegler, C. (2005). A clinical perspective of cochlear dead regions: intelligibility of speech and subjective hearing aid benefit. Journal of the American Academy of Audiology, 16 (8), 600-613.
Ribeiro, N. & Migueis, A. (2008). New potentialities of hearing aids: The frequency transposition in high frequency sensorineural hearing loss. Rev Laryngol Otol Rhino (France) ,129(1), 65-71.
Ringdahl, M. D., Magnusson, L., Edberg, P., & Thelin, L. (2000). Clinical evaluation of a digital power hearing instrument. Hearing Review, 7, 59-64.
Robinson, J., Baer, T. & Moore B. (2007) Using transposition to improve consonant discrimination and detection for listeners with severe high frequency hearing loss. International Journal of Audiology,46(6), 293-308.
Simpson, A., Hersbach, A. & McDermott, H. (2005). Improvements in speech perception with an experimental nonlinear frequency compression hearing device International Journal of Audiology,44(5), 281-292(12)
Simpson, A., Hersbach, A. & McDermott, H. (2006). Frequency-compression outcomes in listeners with steeply sloping audiograms. International Journal of Audiology, 45(11), 619-629.
Souza, P., Jenstad, L. & Folino, R. (2005). Using multichannel wide dynamic range compression in severely hearing-impaired listeners: effects on speech recognition and quality. Ear and Hearing,26(2), 120-131.
Souza, P. (2008). Severe hearing loss - recommendations for fitting amplification.
AudiologyOnline, Article 2181. Direct URL: /articles/article_detail.asp? article_id=2181 Retrieved January 9, 2009, from the Articles Archive on www.AudiologyOnline.com
Summers, V. (2004). Do tests for cochlear dead regions provide important information for fitting hearing aids? Journal of the Acoustical Society of America, 115(4), 1420-1423.
Turner, C. (1999). The limits of high frequency amplification. Hearing Journal. 53(3), 10-14.
Turner, C. (2006). Hearing loss and the limits of amplification. Audiology Neurotology, 11, Suppl, 2-5.
Turner, C.. Gantz, B.. & Reiss, L.. (2008). Integration of acoustic and electrical hearing. Journal of Rehabilitation Research & Development, 45(5), 769-997.
Turner, C.W. & Hurtig, R.R. (1999). Proportional frequency compression of speech for listeners with sensorineural hearing loss. Journal of the Acoustical Society of America, 106, 877-886.
Vinay & Moore, B. (2007). Prevalence of dead regions in subjects with sensorineural hearing loss. Ear and Hearing, 28(2), 231-241.
Xiao, X., Guangshu H., Chunhong Liu., & Jia L. (2008). Improving speech intelligibility of severely hearing impaired people by frequency lowering technique. Scientific Research & Essay,3(6), 259-266.

