
Editor’s Note: This text course is an edited transcript of a live webinar. Download supplemental course materials.
Dr. Francis Kuk: In terms of learning objectives, after this course, participants will be able to: list the physiological basis for poor speech perception at high input levels; list two hearing aid factors that may affect perception at high input levels; and, list two outcomes of the DREAM high input study.
Introduction
Today I want to talk about a common problem that hearing impaired patients tell us about. The problem is speech understanding ability at relatively high input levels, especially when they are wearing hearing aids. In a party situation, where a lot of people are talking at the same time and the music is loud, our patients say that they cannot understand what is going on. Worse yet, some of them may say they can understand better without their hearing aids. As a result, we may come to the conclusion that the hearing aids are the reason why patients cannot understand in noisy situations. We should ask ourselves if it really is a problem with the hearing aid, or if there are other issues that can relate to poor speech understanding in a loud, noisy situation?
Monosyllabic Word Recognition at Higher Input Levels in Quiet and Noise
Let's consider factors that could potentially affect speech understanding at high input levels. The first study that I would like to share with you is from Studebaker et al. (1999), which looked at monosyllabic word recognition at a relatively high input level. In this particular study, the authors tested NU-6 score recognition when the stimulus is filtered between 450 and 2300 Hz. Then these words were presented at eight different levels from 64 dB to 99 dB, and at various signal to noise ratios (SNRs) from -4 to 28 dB. In this test, all 72 normal-hearing listeners and 44 hearing-impaired listeners listened to these words at various levels, as well as at different SNRs.
The data in this study was reported as a rau score, which stands for rationalized arch unit. This score is a transformed score like the adjusted rau score, except it has been normalized on the two extreme sides so that it has equal variance. For our purpose, we can look at rau as a word recognition score, or a percentage.
Performance in Quiet
As far as performance in quiet, there was relatively stable performance for the hearing-impaired group, except above 90 dB, which showed a slight drop, even in the quiet condition. We see poorer performance as the SNR decreases from 28 dB to 24 dB and down. That decrease is not quite as dramatic when the SNR was around 20 dB. However, at a 6 dB SNR, the performance dropped from 64% at a conversational level down to around 40% at a high input level. As the input level increases and the SNR worsens, speech understanding gets poorer and poorer. As intensity increases, speech understanding does not always get better, and gets worse at a very high level.
Quiet performance improves with the input level, which makes sense in the hearing-impaired group. The extra input gives them better audibility, and they get better performance as input increases. Once the speech level reaches about 89 dB, performance plateaus, even up to 99 dB. As the SNR increases, you see a decrease in the overall performance. As the input intensity increases, we do not see quite as strong of an increase in performance when the SNR gets poorer. At a -1 dB SNR, the performance stays poor (around 10%) across the input range. As matter of fact, it starts to decrease when the input is at 99 dB, meaning that when the input increases, there is an increase in speech performance because of the extra audibility, but as it gets to a higher level, especially in a poor SNR, performance stays the same or could get poorer, even in the unaided situation. Subsequently, the authors notice that there was a decrease in performance, which could be related to the audibility or the hearing loss of the patient.
Results
They calculate the expected score and the measured speech score, and then normalized these patients so that what they report is the difference score for the two groups of patients. A zero would represent no difference in the expected score and the measured score. If speech understanding is simply a factor of the audibility of the speech cues, you should get zero across all input levels. On the other hand, if something happened that is beyond an audibility explanation, then you could potentially see a drop in speech performance as the input level increases.
Even the normal-hearing group experienced a drop in performance above an input level of 89 dB in both noisy and quiet environments. The performance of the hearing-impaired group is generally poorer than what is expected of them, and that has to do with the distortions within the auditory system. On top of that, as the input level increases from 69 dB to 79, 89, and 99 dB, it dropped from a level difference of -6% to about -25%, an increase in the degradation effect by about 20% as the input level increases.
As the SNR gets poorer, both the normal-hearing group as well as the hearing-impaired group showed similar decrease in speech performance. This means as sounds get louder, once it overcomes the audibility issues, both normal hearing and hearing impaired people show similar decrease in word understanding scores as a function of the input level.
There can be many reasons for this. From a physiological perspective, this may be due to the lack of specificity in stimulation. When there is a travelling wave stimulation to the basilar membrane at a low-input level, the peak of the excitation is at a particular frequency region. If I present a 4000 Hz tone at a low level, it will create a stimulation around the 4000 Hz area on the basilar membrane. On the other hand, when the input level is higher, it becomes like throwing a large rock into a pond of water. The excitation spreads across the frequency region. You can see that evidence in the firing rate of the neurons. As the input level increases to 70, 80 and even 90 dB, more of the frequency regions surrounding 4000 Hz are excited, even down to about 1000 Hz. It is also stimulative, where we see activity in those neurons.
This is saying that perhaps the reason that normal-hearing people have poorer speech understanding at a high input level is simply because of physics. At a higher input level, there is non-specificity of the stimulation, which results in poorer performance. This suggests that it may not be the patient, or other issues such as cognition. It simply has to do with the physics of sound and how the ear operates.
Louder is not Better
The take-home message for you and your patients is that speech understanding at a high input level, whether it is in quiet or noise, is poorer than that at lower input levels. Therefore, louder is not necessary better. That is very important. Many times, consumers want their hearing aid to be loud so they can hear every word. To a certain extent, that is true, but when it gets to be too loud, it would be worse for speech understanding. Again, this is true for normal hearing as well as hearing impaired people.
Poorer Performance in Aided versus Unaided Conditions
There are things that hearing aids might do to result in poor speech understanding at high input levels. In the literature, we have seen studies showing that speech understanding, especially aided speech understanding at high input level, is not as good as speech understanding at lower input levels or even when not wearing a hearing aid.
For instance, Fletcher and Wegel (1922) reported that when you amplify sounds, they are not very clear to the patient, especially when amplified greatly. We also saw in the 50’s and 60’s that there was a decrease in speech understanding in the aided condition when the input level exceeded a conversational level. We need to ponder if people’s speech understanding decreases as input increases, and for hearing-impaired people who especially need to hear at a higher input level, what is an optimal level at which we can present speech so they may get the benefit of the hearing aid without a negative result from the hearing aid? We may not help them understand better, but the worst thing we can do is to make it worse.
Hearing Aids at High Input Levels
Cox and Alexander did in a study in 1991 showing that listeners do not perform as well in hearing aids at high input levels as they do in the unaided condition. When they were testing three groups of matched subjects in three different environments using the Connected Speech Test (CST), which is a sentence test, they were seeing different performances at different input levels.
Of the three different environments that they used, one was a relatively easy environment, a living room setting (environment A), where speech occured at 55 dB on the A scale, and the noise was at 48 dB. Environment B was a more reverberant setting, where the speech was at a moderate level (63 dBA) and the noise was also around 55 dB. There was still a positive SNR, but slightly louder and slightly more reverberant. Then environment C had speech at 64 dBA and noise at 62 dBA, which by today’s standard is not that bad, but nonetheless, it has a poorer SNR and is slightly louder than the other conditions.
In the quiet environment, (A) there was a significant hearing aid benefit of 24% on the CST. The benefit decreased to about 7% in the more reverberant environment (B), and in environment C, the benefit went to -1%, meaning that wearing a hearing aid in general is poorer than not wearing a hearing aid in that environment. This is one of the first studies to suggest that the benefit of the hearing aid decreases and becomes negative as the input level increases.
What is the Reason?
Hearing aids from 20 years ago are different than the hearing aids today. Most of the hearing aids at that time were linear, behind-the-ear (BTE) style with an omnidirectional microphone. One thing we know about hearing aids now that we did not know then is that the omnidirectional microphone does not optimize the SNR, and perhaps the distortions with a hearing aid may have contributed to the poorer performance, although there was no real exploration into what type of distortion would have caused this. The idea is that perhaps there are more distortions with a hearing aid, and that is why the aided performance is poorer than the unaided performance.
When we talk about distortion, we would try to understand what exactly is causing the distortion. If the hearing aid does not distort, you will hear everything that goes into the hearing aid come out of the hearing aid. But when the hearing aid distorts, you do not hear exactly the same thing. You will hear output at other frequencies that were not present in the input.
Why Does this Matter?
Some of you might ask, “Why would I care about listening at a high input level, especially in light of the data that is available to show that the louder sounds do not occur that frequently?” In 2004, a study by Neitzel et al. showed that most of the sounds occurred at a relatively moderate to moderately-loud level. If you look at the distribution of sounds, only 20% of every-day sounds exceed a 70 dBA level; in other words, only 20% of sounds are louder than loud conversational speech, and only 1% of everyday sound exceeds 90 dBA.
How relevant are loud levels? Why should we care when these sounds do not occur that frequently? Even though they do not occur frequently in everyday life, these louds sounds are typically associated with socializing, entertaining, and transportation. The parties, restaurants, train, and bus may not be everyday situations, but when you do encounter them, you would like for them to be successful. I think this is an important reason why hearing aids should be able to handle those situations.
Sergei Kochkin (2010) did a MarkeTrak report and explained that if you look at a consumer’s satisfaction with a hearing aid, it is typically related to how many situations in which their hearing aid helped them. They may like a hearing aid that helped them only in five situations, maybe by 80%. On the other hand, if a hearing aid can help them understand better or perform better in 10 situations, they would like the hearing aid better. This means the more situations in which the hearing aids can help the user, the more likely the user will be satisfied with the hearing aid. If you can solve not just the conversational situation but also loud situations and soft situations, the hearing aid wearer will probably like the hearing aid more than if you do not that. That is why it is a good reason for us to help not only the conversational sounds, but also look in to different sounds and more challenging situations.
I have listed below four different areas that I think are important to make the aided performance better than the unaided. Because of time constraints, I will only be able to talk about the first factor. However, I will mention them all in order to show you the concept behind it.
1. Minimize distortions occurring at the input and output stages
- True input technology
- Adequate maximum power output (MPO)
- Binaural fitting
2. Reduce gain as input increases (keep output low)
- Wide dynamic range compression (WDRC)
- Gain target
- Noise reduction
3. Enhance SNR
- Directional mic
4. Broadband hearing aid with minimal vent
The fundamental concept is to make the aided performance better than the unaided. To do this, you want to minimize distortion or the risk of any distortions from occurring. If that is the fundamental principle, then everything else is easy to understand.
For instance, the first area is minimizing distortions occurring at the input and output stages. If you have a loud sound that goes into a hearing aid that caused distortion, then you would only have distorted sounds going through the hearing aid. The output stage would be the same. If you have too much output leaving the hearing aid, but the MPO on the hearing aid is not adequate, then you are creating distortion.
The second part has to do with gain. This is also easy to understand. If you have more gain in the hearing aid, it would be louder. However, more gain in the hearing aid would also lead to a higher instance of distortion at the output stage. A high input level with high gain reaches the limit of the hearing aid sooner. When the limit of the hearing aid is reached, it creates distortion. That is why a compression circuit would likely be less distorted than a linear circuit, but it would create distortions in other aspects. The gain target that you use would also create different amounts of distortion in the hearing aid.
The third has do to with SNR. This is where a directional microphone would work very well. If you put a good directional microphone on someone with a mild degree of hearing loss, their performance in noise can be better than normal-hearing individuals, simply because they have technology that gives them a SNR advantage. The aided performance could potentially be better than the unaided when using a broadband hearing aid with minimal venting. When there is a vent in the hearing aid, the loud outside sounds would pass through the vent and neutralize the processing of the hearing aid, giving you essentially the unaided performance and no benefit from the hearing aid processing.
Minimize Input and Output Distortion
Sounds in the environment vary from very soft to very loud (i.e., 100 to 120 dB). The sounds that can be picked up and processed by the hearing aid is what we call the dynamic range of the hearing aid. Today’s microphone has a noise floor of around 20 dB, meaning anything below 20 dB would not be picked up by the microphone. The output limit may be close to 115 dB, meaning anything above 115 dB would create saturation distortion. The hearing aid cannot differentiate anything above 115 dB.
Analog-to-digital converter. Ninety-eight percent of today’s hearing aids are digital. One important component in a digital hearing aid is the analog-to-digital (A/D) converter. This takes the analog input and converts it into a digital signal that can be processed more easily.
The A/D process is affected by many factors. How frequently you sample the signal and the bit depth (how many bits you use) in the A/D process would determine the efficacy of the signal that is processed afterwards. The number of bits within the device determines the dynamic range of that input device. A one-bit system can only go on/off; there are only two states. When there is more than one bit, there are more intervals. For instance, when there are 10 bits, it becomes 1,024 intervals or 1,024 different steps.
Each bit allows for a 6 dB dynamic range. When you have a 16-bit system, you have a dynamic range of 96 dB. This means that if the sounds vary within a 96 dB range, a 16-bit converter can capture and represent that. However, if you have sounds that vary more than the 96 dB range, a 16-bit converter would not work very well, and the representation of the sound will be compromised. If you have a range of sounds from very soft sounds on the bottom to very loud sounds at the top, but the A/D converter is limited, you will be sacrificing some sounds. If you want to save the loud sounds, then you sacrifice some of the softer sounds. On the other hand, if you want to hear the soft sounds, then you might have to sacrifice the loud sounds.
Most of today’s hearing aids have a16-bit A/D converter. In theory, they all have a dynamic range of 96 dB; a microphone only has about a 95-96 dB dynamic range. A 16-bit converter utilizes today’s microphone technology quite well. On the other hand, this 96 dB is a theoretical dynamic range. In real life, that dynamic range is not 96 dB because of the circuit noise floor; it only has 82 dB within this dynamic range. This means even though you have a 16-bit converter, it does not capture 96 dB. In many manufacturing processes, we have to adjust it to maximize what we hear from the softer sounds or maximize what we can hear from the louder sounds because the dynamic range is even more limited than what a 16-bit converter theoretically allows us to have.
Widex’s True Input Technology is able to keep the noise floor of the A/D device to the noise floor of the microphone, but is able to extend the input range/input limit from 103 dB in the Clear hearing aid up to 113 dB in a Dream hearing aid so that it fully utilizes the range that a conventional microphone allows us to do. In the process of doing that, we are also able to change the input dynamic range from the 82 dB to 94 dB. Now we increase the input range so that it can digitize as well as increase the input limit up to 113 dB before any sounds would become distorted.
Sound examples. The following demonstration gives you an idea of how this sounds with and without distortion. The first sound is from a handball game with a lot of noise. Pay attention to the sound quality first with True Input Technology.

This second sound clip has a compression limiter at the input stage. You can still hear the same sound, but the sound quality is different.
You can clearly hear in the second case with the compression limiter that everything is limited to approximately a 95 or 100 dB range. Even though the sound is still audible, it is very muffled and constricted. Much of the temporal variation was not easily detected when compression limiting is applied at the input stage.
You can also hear the difference when listening to music. I would like for you to listen to the music passage process with two hearing aids with different input limits; one is 103 dB and the other is 113 dB.
Now listen to the second one.
You probably noticed that the first sound clip, processed with a 103 dB input limit, contained crackling sounds from time to time. This means that the hearing aid is distorting because the input level reaches 103 dB. Because of that, you also do not hear a lot of low-frequency sounds. The quality of the first clip is not as good as the second. The second clip has a higher input limit and you hear a lot of the volume. There is no crackling sound. That has to do with the input limit of the hearing aid.
Preserving Directionality
Here is an important aspect to recognize. From one perspective, when you have a high input limit, many of the louder sounds can come in the hearing aid and be processed as is. The other aspect has to do with a signal processing algorithm within the hearing aid. The directional microphone depends on a SNR that goes into the hearing aid. In a Clear hearing aid with an adaptive directional microphone, the omnidirectional microphone is active when things are relatively soft or moderate. However, when there are varying levels of noise in the background, it changes its polar pattern, even at loud levels, but will show directional benefit as it changes the directional pattern.
On the other hand, if you go into a very loud input level, that level will saturate the hearing aid, and the effective SNR going into the hearing aid would not be as evident for the hearing aid to recognize how to set the directional pattern. It reverts back to an omnidirectional microphone mode, even though on paper, it is a directional microphone. In those situations, having a directional microphone may not benefit the patient any more than simply having an omnidirectional microphone.
We did a study many years ago showing that this could happen (Kuk, Lau, Korhonen, & Crose, 2014 ), but if you have True Input Technology where the input limit is increased to 113 dB, the directional pattern may still be maintained.
The study was replicated both at Washington University as well as with Marshall Chasin at the Musician’s Clinic in Canada (Chasin, 2014). We used 10 hearing impaired patients in our study, and none had musical training. Figure 1 shows the average audiogram of the participants. We compared our Clear hearing aid with the Dream hearing aid. These two hearing aids are identical in every aspect except that the Clear hearing aid has an input limit of 103 dB and the Dream has 113 dB. Any differences that we see would be an effect of the True Input Technology. These subjects were tested at a high input level.
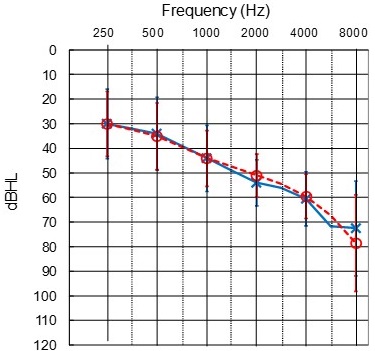
Figure 1. Average audiogram of study participants.
We first recorded the NU-6 stimuli through KEMAR in a soundfield. When we recorded the stimuli, we programmed the hearing aids to a flat 50 dB hearing loss with an omnidirectional microphone and no noise reduction in one situation, and in another situation, we activated the adaptive microphone with noise reduction. Speech was presented from the front with noise at the sides and back at +3 SNR. We tested subjectively as well.
Interestingly, even though the input is high at 110 dB, the true output of the hearing aid is not much higher because of gain processing and compression in the hearing aid. The output at 110 dB input only ends up being only 1 or 2 dB higher than the input level. To further minimize the potential of any over-amplification or temporary threshold shift, we tested the patient under headphones while they adjusted the level of the sound to be loud, but not uncomfortable. At no time were they at risk of sounds being damaging. We used a double-blind design study and we tested them.
Sound examples. To give you an example of the sound that we hear, listen below. The first is the example with Clear hearing aid. See if you can identify the word.
The next is the sound with the Dream hearing aid.
In the second example, the word was “bass”, and it was much clearer than the first one. This is because of the True Input Technology.
In Figure 2, the triangle represents the performance with the Dream, and the circle represents the performance with the Clear hearing aid at +3 SNR. The dotted line shows the omnidirectional microphone without any noise reduction and the solid line shows the performance with the noise reduction and the directional microphone. First, look at the Clear hearing aid with the directional microphone and noise reduction. You can see without the directional microphone or noise reduction that the performance is quite poor across SNRs. Even at a +3 dB, we are only getting 7% performance. Directional microphones do work. You can see that the directional microphone and noise reduction brings the Clear performance up to about 13% at +3 SNR. While the percent-correct score is doubled, performance is still relatively poor, even when there is a directional microphone over there.
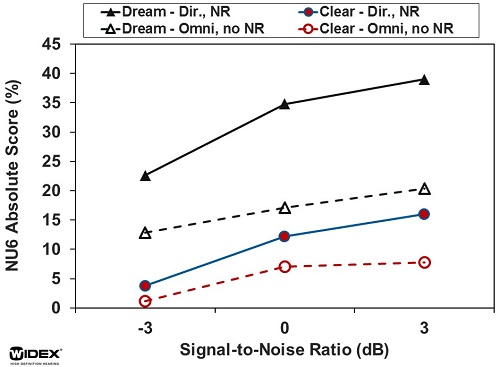
Figure 2. Comparison of Clear and Dream hearing aids with directional microphone and noise reduction options.
In the Dream hearing aid with omnidirectional mode without any noise reduction, the performance at any SNR is higher than the Clear hearing aid with the noise reduction and with directional microphone (Figure 2). That tells us how important it is that the input going into the hearing aid remains distortion-free. If there is a distorted signal going into the hearing aid, even though it has a directional microphone and noise reduction, you still get poorer performance than an omnidirectional microphone.
When we further provided the directional microphone and noise reduction in the Dream hearing aid, performance at a +3 SNR went up to 40%, instead of the 10% with the Clear. The directional microphone works better when the input SNR is favorable and when distortion is low. It demonstrates that the input limit is important. It also demonstrates that the directional microphone and noise reduction features are important in a hearing aid.
We also did subjective evaluations looking at the preference at a high input level (above 110 dB) and a conversational level, when we indicate a lull using speech and music. When we used speech, there was no difference in preference at the softer level. The Clear and the Dream were equally preferred. However, at a high input level for speech, the Dream was more preferred than the Clear (70% to 30%, respectively).
The preference ratings for music were taken from Dr. Chasin’s clinic in Canada (Chasin, 2014), so his test subjects were all musicians, which differs from our sample. For the high-level testing, we see an 80% to 20% benefit in favor of the high-input technology. Even for the lower input at a conversational level, there was a statistically significant preference for the Dream over the Clear hearing aid. This is possibly because the little distortion that we as non-musicians could not detect were detected by these musicians. That is why they prefer the higher input technology. From that perspective, True Input Technology could also make a difference in the outcome.
The take-home message is to make sure you have a hearing aid with a high input limit and hopefully a large dynamic range so that the hearing aid can process sound and give a good sound quality.
Importance of Adequate MPO
We discussed the input of the hearing aid and will now talk about output, specifically MPO. In Figure 3, I show the output of a hearing aid connected to three different receivers: the HP receiver, the P receiver, and the M receiver. You can see the output limit of each for moderate to severe degree of hearing loss.
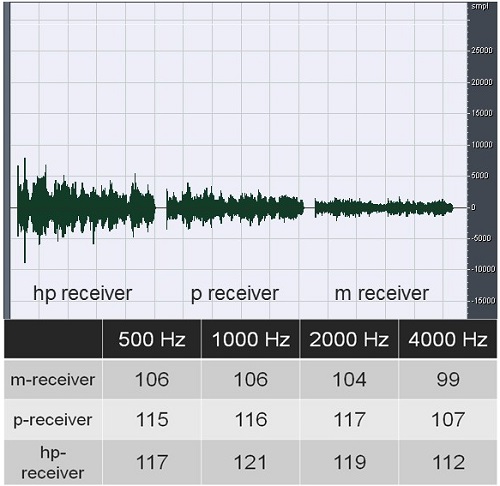
Figure 3. MPO of three different-power receivers from 500 to 4000 Hz.
Even though the gain on the hearing aids is set exactly the same for this hearing loss, the MPO on the hearing aid could make a difference in terms of the overall loudness of that particular sound. Let’s listen.
The first one you will hear is the output for the HP received, followed by the P receiver, followed by the M receiver.
Hopefully you can hear that the overall loudness of the three noise backgrounds is very different. The HP receiver has a higher output limit, which gives more sounds, whereas the M receiver for the moderate to severe hearing loss was not giving an adequate output. That is why things get softer and more muffled.
Because of that, we conducted a study several years ago looking at the effect of the MPO on speech understanding in noise (Kuk, Peeters, Lau, & Korhonen, 2011). We wondered if we fit someone who is a candidate for the HP receiver with an M receiver, meaning we did not give him an adequate output, if there would be poor speech-in-noise performance.
We tested 11 patients with moderate to severe degrees of hearing loss at two different input levels. We set the MPO, one to the default level for the hearing loss of the patient and the other at the default minus 10 dB. This means that the MPO is not enough for the patient in cases where the limit of a hearing aid is being pushed.
Results
The coupler output for a 60 dB input and 70 dB input were exactly the same. At a 90 dB input level, the MPOs were slightly different, but only at a high input level and not at a conversational or soft level. We tested participants using the HINT test. I would like to focus on the off condition where there is no noise reduction; this is simply a result of the default MPO or the lower MPO (MPO -10).
With the default MPO, the SNR that was required was about 9 dB. When we lowered the MPO, it increased to 10.5 dB. This means that when the MPO is adequate, you get a certain SNR, which equates to a certain level of speech-in-noise performance. However, when the MPO is compromised and is too low, speech understanding in noise would be poorer.
The implication is that when it comes to selecting a hearing aid for take-home use, you often see manufacturers indicating that a particular amount of hearing loss fits into a static fitting range. Sometimes we may see that a patient likes a small hearing aid and the manufacturer fitting range says their hearing loss fits, and we go ahead with it, even though the hearing loss is barely above the bottom of the fitting range. That would be a mistake. Even though the patient can hear speech comfortably, they likely will not do well in noise when the MPO is reached so close to their hearing thresholds. The dynamic range is too small.
When you are selecting a particular model of hearing aid for a patient using the fitting range guide, do so when the hearing loss falls somewhere in the middle or even two-thirds down. However, when it is in the lower one-third of that fitting range, it is likely not acceptable from a speech-in-noise perspective.
Do Hearing Aids Work at High Input Levels?
If we now consider making perfect both the input limit and the MPO of the hearing aid, do we get better aided performance in a loud noisy situation?
In this next study, we had 10 subjects with moderate sloping to severe hearing loss and five subjects with normal hearing (Kuk, Lau, Korhonen, & Crose, 2015). We tested speech in quiet and speech in noise at 65, 85, and 100 dB SPL with speech in front and noise in back. We wanted to see how they performed comparing aided performance to unaided performance, and how that compared with normal-hearing people.
On the input/output curve of the hearing aid, the input did not go into compression limiting until 113 dB. A static input/output curve has a relatively flat slope, meaning there is a lot of linearity in the hearing aid, and the compression ratio is quite high from this perspective.
Performance for Normal Hearing
Performance of the normal hearing subjects is shown in Figure 4 for 50 and 65 dB inputs. As we expected, they do very well at 95 to 100% on this scale.
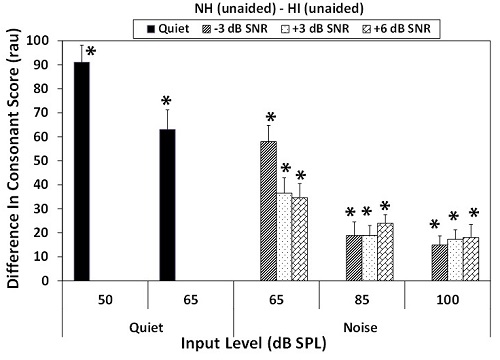
Figure 4. Scores for normal hearing subjects in quiet and in noise.
Performance on the Nonsense Syllable Test at the different SNRs (+6, +3 and -3) was fairly good for 65, 85 and 100 dB for the normal-hearing group. There was no significant improvement in speech understanding from 65 to 85 dB. As a matter of fact, when we increased the input level to 100 dB it decreased performance. What about the hearing-impaired people?
Performance for Hearing Impaired
As you would expect, there was poorer performance at softer inputs in the unaided condition. The performance increased as the input level increased. The input level increased above 85 dB, and then there was a slight decrease. That might also have to do with the spread of excitation, meaning when the sound is loud, it causes more stimulation and less specificity in terms of what happens with the input.
In the aided situation, performance improved in quiet, but performance of the aided condition in noise stays at a relatively constant level. At +6 dB, the score stays at around 60% across the three input levels. When the SNR decreased to -3, there was a slight decrease. In general, there is a dramatic improvement in quiet as well as the noisy conditions.
Now we can compare the difference in score between normal listeners and hearing impaired in the unaided condition.
Comparison of Normal Hearing and Hearing Impaired
The major difference between the normal hearing and hearing-impaired group is the soft sound in quiet situation. As the situation gets louder from 65 to 100 dB, there is less of a difference. Although it was statistically significant, the magnitude of that difference decreased between the normal and the unaided condition - about 20% at a loud, noisy level.
What kind of benefits do we get with the hearing aid? Any positive difference would suggest that the hearing aid provides benefit. In quiet situations, there is 60% of benefit at 50 dB. Interestingly though, the benefit noted before decreases with input level because their performance was not bad to begin with. However, once we have captured the true input limit as well as the adequate MPO, the hearing aid was giving a statistical benefit even at a 65, 85, or 100 dB input level. This means that a 10% improvement is statistically significant compared to the unaided condition. A properly fitted hearing aid can give aided benefit at loud input levels. It does not have to be poorer than not wearing a hearing aid.
When you compare this to normal hearing people, the difference between normal hearing and hearing impaired shows still a bit of difference for soft or conversational sounds, which is something that a hearing-impaired patient can control. They would have a remote control to adjust the volume to minimize that difference. When you compare normal-hearing and hearing-impaired aided performance at 65, 85, and 100 dB, the difference is typically less than 10%.
Other than this condition where there is still statistical difference, there is no difference among the three conditions with the normal-hearing group. This means when the hearing aid is fitted properly, aided hearing can be as good as normal hearing at loud input levels. Bear in mind that the normal-hearing subjects we used were 20-year-olds, and the test subjects we used were 70-year-olds. We are unfairly penalizing our conclusion from that perspective. If we were able to get older normal-hearing subjects, we may see a slight difference in terms of the performance.
Conclusion
Our conclusion is that when you fit hearing-impaired people properly, you can get performance similar to what normal hearing people can achieve under the same conditions that we have shown you. We can also see that the preference for the aided sound decreases as input level increases, as we expected. The preference for the unaided increased as the input level increased, which is true for both music and speech, and the cutoff point is around 80-85 dB.
From this study, we should recognize normal hearing people have difficulty with speech understanding in loud, noisy situations. The Dream hearing aid does provide benefit even at high input levels, and aided performance can be similar to normal-hearing listeners.
Maximizing Speech Understanding at High Input Levels: Take Home
I think it is important that you chose a hearing aid with a high input limit so that the natural sounds, especially those loud ones, can enter the hearing aid without creating any distortion, Make sure that the hearing aid that you choose fits the real range of hearing loss of the patient so that you do not have an MPO or output limiting issue. You simply cannot have a lot of gain from the hearing aid and a very low MPO; it will compress all of the signal.
Broad frequency response is important because it gives all the nuances, high-frequency sounds, as well as low-frequency sounds. A compression hearing aid is important because it minimizes distortions. Noise reduction is important, as are adaptive directional microphones.
If possible, you should choose an occluding ear mold because it better allows the patient to hear the output of the hearing aid and not the input, which leaks through the vent into the hearing aid. With some vented ear molds, there may be sounds in the ear canal that are entirely different from what the processed sound is. In essence, wearing a hearing aid with an open ear mold or a highly vented ear mold results in similar performance as the unaided condition.
Setting Expectations for Patients
Setting the right expectations for patients is very important. As a clinician, I measure speech in quiet and speech in noise as part of the clinical protocol. Speech in quiet allows me to know their potential. If I can make all the noise go away, what is the likelihood of the patient achieving a certain performance level? It does not tell me how much difficulty the patient has, but gives me an idea of their potential. Measuring speech in noise gives me an idea of how much difficulty they have. That also gives you an idea of the technology you would recommend.
It is important to let the patient be aware of the decrease in intelligibility even in normal-hearing listeners. Oftentimes, when patients have a hearing loss, they think that the problem they experience is only their problem and not a universal problem. That would allow you to do better counseling with your patient.
Beware of the issue of effective audibility. Louder does not always mean better or more intelligible. When the sound at the ear is more than 100 dB, it starts creating distortions. Hearing impaired patients do need to hear sounds at a higher input, so that is why we cannot expect them to have the same speech understanding scores as normal-hearing people at a lower input level. But if we keep increasing the output of the hearing aid, it simply does not make it better for them. Sometimes lowering the overall gain of the hearing aid is a much better way of achieving better intelligibility than turning up the volume in the hearing aid.
Be aware of the hearing aid features that could benefit speech in noise at a high level. I think the results of our current studies would help you in counseling your patients.
References
Chasin, M. (2014). A hearing aid solution for music. Hearing Review, 21(1), 28-30.
Cox, R., & Alexander, G. C. (1991). Hearing aid benefit in everyday environments. Ear and Hearing, 12(2), 127-139.
Fletcher, H., & Wegel, R. L. (1922). The frequency-sensitivity of normal ears. Physical Review, 19(6), 553. doi: 10.1103/PhysRev.19.553
Kochkin, S. (2010). MarkeTrak VIII: Customer satisfaction with hearing aids is slowly increasing. Hearing Journal, 63(1),11-19.
Kuk, F., Lau, C., Korhonen, P., & Crose, B. (2014). Evaluating hearing aid processing at high and very high input levels. Hearing Review, 21(3), 32-37.
Kuk, F., Lau, C. C., Korhonen, P., & Crose, B. (2015). Speech intelligibility benefits of hearing aids at various input levels. Journal of the American Academy of Audiology, 26(3), 275-288. doi: 10.3766/jaaa.26.3.7
Kuk, H., Peeters, H., Lau, C., & Korhonen, P. (2011). Effect of maximum power output and noise reduction on speech recognition in noise. Journal of the American Academy of Audiology, 22(5), 265-273. doi: 10.3766/jaaa.22.5.3
Neitzel, R., Seixas, N., Olson, J., Daniell, W., & Goldman, B. (2004). Nonoccupational noise: exposures associated with routine activities. Journal of the Acoustical Society of America, 115(1), 237-245.
Studebaker, G. A., Sherbecoe, R. L., McDaniel, D. M., & Gwaltney, C. A. (1999). Monosyllabic word recognition at higher than normal speech and noise levels. The Journal of the Acoustical Society of America, 105(4), 2431-2444.
Cite this Content as:
Kuk, F. (2015, July). Improving aided hearing at high input levels. AudiologyOnline, Article 14423. Retrieved from https://www.audiologyonline.com

