
From the Desk of Gus Mueller
![]() As audiologists, we’re pretty good at conducting behavioral testing that assesses our patients’ complaints regarding hearing and communication. Problems with hearing soft sounds? We conduct pure-tone threshold measures. Problems with understanding speech in background noise? We conduct tests such as the QuickSIN, BKB-SIN or the WIN. Problems understanding in background noise despite normal hearing thresholds? Maybe we conduct some speech tests that are sensitive to auditory processing problems. But what about the complaint of excessive listening effort—the patients who say that they just feel “drained” and fatigued after extended listening? Do we have tests to measure this?
As audiologists, we’re pretty good at conducting behavioral testing that assesses our patients’ complaints regarding hearing and communication. Problems with hearing soft sounds? We conduct pure-tone threshold measures. Problems with understanding speech in background noise? We conduct tests such as the QuickSIN, BKB-SIN or the WIN. Problems understanding in background noise despite normal hearing thresholds? Maybe we conduct some speech tests that are sensitive to auditory processing problems. But what about the complaint of excessive listening effort—the patients who say that they just feel “drained” and fatigued after extended listening? Do we have tests to measure this?

Gus Mueller
We could simply ask our patients to rate their listening effort for various situations, but it seems like there should be better ways for getting at the problem. There are, and that’s what this month’s 20Q is all about. The test procedures are not quite “ready-for-the-clinic” just yet, but research efforts have shown encouraging findings. Our guest author reviews what cutting-edge procedures are being developed and validated.
Erin Picou, AuD, PhD, is a Research Assistant Professor in the Department of Hearing and Speech Sciences at Vanderbilt University Medical Center. Dr Picou also is involved with teaching and mentoring AuD students at Vandy.
As part of the Vanderbilt Dan Maddox Hearing Aid Research Laboratory group for the past six years, she has been awarded numerous industry and federally funded research grants. As you know from her many publications, her research interests are primarily related to hearing aid technologies for adults and children, with a specific focus on speech recognition and listening effort.
I happen to know that Erin likes all things outdoors, like running, biking, and swimming—sometimes all on the same day (ouch). Watch for ESPN headlines highlighting the Vanderbilt Picou-Ricketts-Hornsby triathlon team. And by the way, if you happen to have reason to address Erin formally as Dr. Picou, you might struggle as I have, regarding pronouncing Picou—Pick-Oh? Pee-Que? Erin tells me it’s Pick-Who, said quickly with a soft “w.”
Fortunately, you don’t have to know or pronounce any French words to read and appreciate this excellent review article written by Erin. And, it might just enhance your clinical savoir-faire.
Gus Mueller, Ph.D.
Contributing Editor
August 2013
To browse the complete collection of 20Q with Gus Mueller articles, please visit www.audiologyonline.com/20Q
20Q: Listening Effort - We Know It’s a Problem But How Do You Measure It?

Erin Picou
1. I’m glad that you agreed to have this talk about listening effort, but I’m not exactly sure I even know what it means?
Well I’m glad to have the talk, too, as it’s something I’ve been working with the past few years. Listening effort certainly has received a lot of attention in the journals and at conferences lately. Defining “listening effort” can be a little tricky, and the definition might be different depending on who you ask. I like to think of it as that feeling of being tired when you have to work really hard to understand what’s being said. You might have experienced this in a crowded restaurant, over a crummy cell phone connection, or in a big lecture hall. Researchers have suggested more formal definitions. The one I like is that listening effort reflects the cognitive resources necessary for speech understanding (Hicks & Tharpe, 2002). That is, increased listening effort means more brain power is needed to recognize and understand speech. While the relationship between listening effort and fatigue is complex, many believe it is this use of additional cognitive resources that leads to the feeling of being mentally tired or drained when trying to understand speech.
2. That’s interesting, but how do you think my patients might describe it?
You’ve probably heard patients complain they are tired from straining or working to hear. They might use words like “exhausted” or “drained” when trying to listen in noisy places like restaurants. These experiences of working hard to hear in noise can add up over time, leading patients to feel tired all day long, or at the least, at the end of the day. Indeed, researchers have found that people with hearing loss may need more time at the end of the day to rest and recover from working so hard to hear (Nachtegaal et al., 2009). Clearly, listening effort has some direct relevance to our patients. So, we’re trying to figure out why they have to work so much harder, and if there’s anything we can do to make things better.
3. You say, “make things better”—I assume that background noise increases listening effort?
Exactly. Using several kinds of measurement tools, we’ve seen repeatedly that the presence of background noise increases listening effort. It could be noise from other people in a restaurant or from distortion over a telephone connection. So, that feeling in a crowded restaurant that you have, the one where you’re tired because you’re listening so hard, that’s listening effort. When it’s harder to hear, people have to recruit extra cognitive resources to help understand speech. What is especially interesting though, is that there can be a change in listening effort even in cases when speech understanding does not change. This opens up interest in interventions like specific types of hearing aid processing that may have benefits to listening effort, even if this very same processing does not directly improve speech recognition.
4. It would make sense that people with hearing loss have increased listening effort. Is this true?
We’ve definitely seen that people with hearing loss demonstrate more listening effort than those with normal hearing. It doesn’t take much hearing loss, either. Several researchers have reported that even mild hearing loss causes increased listening effort (Rabbitt, 1991; McCoy et al., 2005). This means that most of our patients are probably experiencing more listening effort than people with normal hearing. This may have significant consequences on their energy level, how much recuperation time they need at the end of the day, and even their absenteeism at work (Nachtegaal et al., 2009).
5. That’s not good. Can we fix this with hearing aids?
I’d like to tell you that, but it may not be that simple. It does appear, however, that for many patients hearing aids do indeed help. Theoretically, any technology that makes it easier to hear should improve listening effort. Back in 1982, Downs published a study that demonstrated that hearing aids can improve not only speech recognition, but also listening effort. More recent evidence also supports that hearing aid use may reduce listening effort (Gatehouse & Gordon, 1990; Hornsby, 2013; Picou, Ricketts, & Hornbsy, 2013).
In addition, some investigators have reported that specific hearing aid features, like digital noise reduction, may reduce listening effort (Sarampalis et al., 2009; Ng, Rudner, Lunner, Pedersen, & Ronnberg, 2013). Other investigators who evaluated different technologies, like directional microphones, have not confirmed these same benefits (Hornsby, 2013). These mixed results aren’t surprising. The extent to which hearing aid technologies improve listening effort will vary by feature, study design, and likely the individual patient. Moreover, how specific technologies are implemented varies among manufacturers; therefore, there could be manufacturer-specific effects on listening effort. In addition, I believe one of the reasons results have been mixed may be limitations of the test methods. We need reliable and valid measurement tools that are also highly sensitive to assess listening effort, and to accurately evaluate hearing aids technologies.
6. I was just about to ask how you measure listening effort. I assume you can’t just ask the patients how hard they are trying?
Well . . . actually that is one approach that has been used. But you’re right, it can be difficult to measure listening effort and its interaction with “cognitive resources.” People have tried lots of different things. Generally, there are four kinds of approaches: subjective, physiologic, recall, and reaction time based paradigms. The measurement tool is to ask someone how much effort they put in or how tired they feel, which gives you a subjective rating of listening effort. Researchers have done this by using informal questions like “how tired do you feel now?” or “how much effort did you put into listening?,” and then have the patients rate their responses on something like a Likert scale. Some use questionnaires that have been developed especially with listening effort in mind. For example, the Speech, Spatial and Qualities of Hearing Scale (SSQ; Gatehouse & Noble, 2004) includes some questions about listening effort. The most relevant one is, “Do you have to put in a lot of effort to hear what is being said in conversation with others?” A patient would rate their effort on a scale of 0 to 10, where 0 means “lots of effort” and 10 means “no effort.” Finally, some researchers have used more general scales of physical effort or work, and applied it to listening effort. For example, Borg’s CR-10 scale of physical exertion (Borg, 1990) has been applied to listening effort (Hallgren, Larsby, Lyxell, & Arlinger, 2005; Larsby, Hallgren, Lyxell, & Arlinger, 2005). In this case, patients would rate their perceived mental exertion on a scale of 0 to 10, where 0 means “nothing at all” and 10 means “maximum exertion.” A rating of 10 would indicate the most effort or exertion a person has ever experienced.
7. Those seem like easy ways to measure listening effort—something I could easily use with my patients. Why wouldn’t everyone use those techniques?
You’re right - it’s very easy to ask someone to rate their subjective perception of listening effort. Clinically, this is quick, easy, and seems to be directly related to what we’re after. However, subjective measures may not be the most reflective of “increased cognitive resources”—something that I mentioned earlier. Consider that if the effort does not result in the use of added cognitive resources, then maybe we don’t care as much about the effort. There is emerging evidence from several laboratories that the subjective ratings of effort are not correlated with objective measures of effort (Hicks & Tharpe, 2002; Sarampalis et al., 2009; Fraser, Gagne, Alepins, & Dubois, 2010; Mackersie & Cones, 2011).
There are many potential explanations why subjective and objective measures aren’t strongly related. For example, patients may have trouble being introspective and unbiased. Specifically, you might ask your patient how much effort they exerted while listening to some sentences in quiet. They might reply that they exerted a lot of effort, even though it’s early in the test session and the sentences should be relatively easy to hear. The reason for this response may be that the patient was tired because of something unrelated to listening, like a restless night’s sleep. In addition, the patient may not have yet experienced a difficult listening condition in your office, and has to re-calibrate his/her response after listening to something more challenging. Similarly, patients may have trouble remembering perceived effort over the course of the test session. Finally, patients may be rating their perceived performance and not perceived effort. In some cases, ratings of effort more closely align with speech recognition performance than measures of true listening effort. Regardless of the reason, these results tell me that asking people to rate effort may be an unreliable measurement tool in the laboratory. However, we certainly shouldn’t discount it completely. We just need to be aware that subjective and objective measurements may give us different results.
8. By objective measures of effort, do you mean the other three kinds of tests you mentioned?
Yes. The three general types of objective measures of listening effort include physiologic, recall, and reaction time based paradigms. Physiologic paradigms rely on the bodily responses that are thought to occur when listening is tough. Briefly, researchers measure the body’s response and how it changes when listening is more difficult. For example, investigators have measured pupil dilation (Zekveld, Kramer, & Festen, 2010) and also heart rate and skin conductance (Mackersie & Cones 2011). If you’re interested, check out these papers—they both have more details about these measures.
9. So what kind of tests do you use to measure listening effort?
We have used two different objective measures: recall and reaction time based paradigms. Both of these capitalize on the fact that human cognitive capacity is fixed; that is, each individual has a finite amount of cognitive resources. So, if you have to use more resources to understand speech, there are fewer resources available to do other things. It is then reasonable to assume that if cognitive resources have been diverted toward speech understanding, they must have been directed away from something else.
In the case of a recall paradigm, resources are directed away from rehearsal and recall. In this case, recalling fewer items is interpreted as increased “listening effort.” One recall paradigm that we used recently was based on the work of Pichora-Fuller and colleagues (Pichora-Fuller, Schneider, & Daneman, 1995). During testing, the patient listens to sentences and is instructed to repeat the last word in each sentence. After a certain number of sentences have been presented (e.g., 8 sentences), the patient’s task is to recall all of the last words in that block (e.g., 8 final words).
10. I think I understand how a recall task might work, how do reaction-time based paradigms measure listening effort?
Like recall tasks, the assumption is that during situations of increased listening effort, fewer resources will be available for other things. In this case, the “other things” involve a physical response. The simplest form of this kind of task is to measure how long it takes to begin repeating a word or sentence. More complicated tasks involve pressing a button whenever a light appears or asking a listener to trace a circle on a computer screen while simultaneously performing the speech recognition tasks.
11. So many tasks to choose from, how do you pick the best one?
Fortunately, all of the tasks seem to be valid measures of listening effort. As a field, it’s good that we have people using them all. It strengthens our understanding because we have converging lines of evidence that help us understand listening effort. But certainly each task has strengths and limitations. As I mentioned, subjective ratings are easy and make logical sense. However, they don’t relate well to these other kinds of measures I mentioned. Remember, it’s not clear that asking people about the experience and testing them related to the experience will give us the same answer.
Physiologic measures have upsides and downsides, too. On the plus side, they measure something involuntary, so we don’t have to trust that the patient is being honest or is trying as hard as possible. The downside is that it takes considerable expertise and specialized equipment to make these measurements. It’s not something you’d likely do in the clinic. In addition, it’s not clear what role emotion plays regarding these responses. We know that responses to emotional stimuli may influence these involuntary responses. For example, emotional stimuli have been shown to increase pupil size (Partala & Surakka, 2003) and skin conductance (Meyers & Smith, 1986; Bradley, Greenwald, Petry, & Lang,1992), which are the same expected effects of increased listening effort (Zekveld et al., 2010; Mackersie & Cones, 2011).
Recall tasks seem to have solid face validity. What I mean by that is, people in daily life are often confronted with the task of listening to speech and remembering what they heard. It makes some sense to ask people to do something with the speech they heard in order to get an idea of how much brain power they’re using. Also, recall tasks are easy to administer with standard audiometric equipment. However, these tasks may be especially sensitive to ceiling and floor effects. When listeners recall too many or too few items, the results can be less meaningful.
Reaction time tasks have the advantage of being relatively easy to implement, although you will need a reliable method to measure response time. In addition, reaction time measures make sense theoretically. However, they lack some face validity. Often participants ask me, “how does me pressing this button tell you anything about my hearing? My vision is fine!” In addition, reaction time measures may be pretty variable within and across patients. Also, they tend to be sensitive to learning and fatigue effects. That is, people are a little slow at first, get better at the task over time so they get faster, and then slow down again as they get tired of being tested.
12. Are there any considerations for special populations? For example, what about testing listening effort with older adults?
Good point. Since the prevalence of hearing loss increases with age, we definitely have to consider that these measures need to be useful for the elderly population. Let’s look at the viability of each measure in turn. First, I don’t think subjective measures need special considerations when working with an elderly population. So, that’s easy. In terms of physiologic measures, there may be interactions with aging. For example, pupil size generally decreases with advanced age. Therefore, it may be more difficult to measure changes in pupil size. Measures of skin conductance may also be more difficult with the elderly since their skin may be more dry or wrinkled.
Recall paradigms may also be susceptible to the effects of aging. Older adults may have more difficulty remembering in general, even in the absence of hearing loss. This increased difficulty with memory may lead to floor effects if the recall task is too difficult. Making the task easier to avoid floor effects for older adults may make the task too easy for patients who are younger or have normal hearing, leading to ceiling effects in this population. Thus, it’s a balancing act to find a task difficulty level that would be appropriate for comparing adults with normal hearing to adults with hearing loss when using a recall paradigm.
Reaction time paradigms also require consideration when testing adults who are older. In addition to the reduction in memory ability with age, older adults’ reaction times tend to be generally slower than younger listeners’, regardless of hearing status. One way to get around this is to use a baseline measure and subtract this baseline from performance during the reaction time task.
Remember that these are all simply considerations for testing an older population. Researchers are pretty good about controlling for these factors for investigations of listening effort. In all cases, if the researcher is interested in within-participant effects (background noise, hearing aid use), each participant serves as their own control. That is, the absolute pupil size, recall performance, or reaction time is less important than the difference between conditions. It’s a little more difficult to report on the between-participant effects, such as age or degree of hearing loss.
13. Wait, are you saying we don’t actually know if hearing loss has an effect on listening effort?
No, not exactly. What I’m saying is, as with other areas of hearing science, separating the effects of age and hearing loss is tough. The prevalence of hearing loss increases with age, so studies investigating the effects of hearing loss also usually include age effects. The exceptions are those studies that have successfully tested listeners with normal hearing who are older or listeners with hearing loss who are younger. I’m not saying this invalidates the research findings, I’m only suggesting that we have to be careful when drawing conclusions.
14. Are there also considerations for testing listening effort in a pediatric population?
Testing the pediatric population does require some careful thought. The task has to be easy enough for a younger population, but hard enough to tap into their cognitive resource pool. If the task is too difficult, younger listeners may focus on the secondary task, letting speech recognition performance decline (McFadden & Pittman, 2008). This shift in cognitive resources from speech recognition to the secondary task means that you’re not actually testing listening effort anymore. So, the choice of methodology is important. It’s not clear what is the best way to measure effort in kids. However, a few research laboratories have used reaction time based paradigms (Hicks & Tharpe, 2002; Howard, Munor, & Plack, 2010).
15. I’m still not sure you answered my earlier question. How do you know which measure to pick?
Using carefully designed studies, appropriate equipment, and keeping the technological considerations in mind, all types of listening effort measures can be successfully used to tell us interesting things. Because I’ve had the most experience with recall and reaction time paradigms, those are my favorite. Specifically, we recently developed a reaction time paradigm that I think offers a nice balance between the face validity of speech recall tasks (asking a patient to do something with the speech they heard), but still avoiding the floor effects of a recall paradigm.
16. So . . . let’s hear about it.
Sure. It’s a reaction time measure and a dual task paradigm. During testing, the patient repeats monosyllable words, presented in either quiet or in noise. These words are spoken by a female talker and are a mix of nouns, verbs, adjectives, and adverbs. The words are the same words as those contained in the word lists you are already familiar with, like the NU#6, W-22, and PBK words. The patient’s task is to always repeat the word heard, but if the word is a noun, the patient presses a button on a keypad as quickly as possible. Like other reaction time measures, longer reaction times are interpreted as indicating increased listening effort. Thus, the patient performs word recognition, but also processes the speech heard and presses a button.
17. How is this different from the other measures you discussed?
While it’s similar to some of the other measures before, it is a little different. I think this new test is actually more sensitive to the things we know affect listening effort than some other tests. To verify this, we are testing two groups of adult listeners; one group has normal hearing and the other has hearing loss. The four measures we are using are: 1) the recall paradigm I described earlier (repeating back the last 8 words), in addition to three reaction time measures; 2) a Simple Dual Task paradigm; 3) a Complex Dual Task paradigm, and 4) the new paradigm I just described that I’ll call the Semantic Dual Task paradigm.
All three reaction time based, dual task paradigms use the same monosyllable words spoken by the female talker for the primary task (speech recognition), and they vary by secondary task (always reaction time measure). In all cases there are probe and non-probe trials. During non-probe trials, the participant’s only task is to repeat the word presented. During the probe trials, the participant is expected to repeat the word stimuli, but also to press a button in response to a probe stimulus. For the Simple paradigm, during a probe trial, a red box appears on a computer screen and a participant’s task is to press a button as quickly as possible. Probe trials occur 25% of the time. This task was based on an early study by Downs (1982), and was used later by Hicks and Tharpe (2002).
During the Complex paradigm, which was based on the work of Sarampalis et al. (2009), the secondary task was more complicated. During a probe trial, a number appears on either the left or the right side of computer screen. A participant is instructed to push one of two buttons, based on whether the number is odd or even and whether the number appears on the left or right side of the screen. Probe trials occur approximately 25% of the time.
Finally, during the Semantic paradigm, a participant’s job is to press a button if the word presented was a noun. Approximately 40% of words are nouns, but the exact number will depend on whether or not the patient correctly heard the word.
For all paradigms is this study, we are testing participants in quiet and in noise. In this manner we can evaluate the effects of noise. In addition, comparisons between participant groups allowed us to calculate the mean effects of hearing loss. But remember, there was an age difference between the participants, so the effect of “hearing loss” also included any effects of aging, since our listeners with normal hearing were also younger than the listeners with hearing loss.
18. So what did you find?
As I mentioned, we are testing these participants on all four measures of listening effort. So far, we have preliminary data collected for 20 participants, 10 participants have normal hearing (mean age 24 years) and 10 participants have hearing loss (mean age 57 years). With the recall paradigm, we ran into floor effects for the listeners with hearing loss. By floor effects, I mean that, even in the easiest condition, participants could only remember a couple of words. When we made the condition harder by adding noise, they still could only remember a couple of words. Although this result could mean that adding noise did not affect recall performance, it could also mean the task was too difficult. The words the participants could recall were typically the most recent words presented (words 7 and 8 in a set). We would expect everyone to remember these words, no matter how difficult the condition, unless they couldn’t hear the words. Therefore, it’s more likely that we were seeing floor effects rather than seeing no effect of noise. However, I haven’t discounted this task entirely as I think it provides some valuable insight into listening effort. But, I’m not convinced it’s the right choice for evaluating factors that will have potentially smaller effects on listening effort, like hearing aids or specific hearing aid technologies.
The results with the reaction time based, dual task paradigms are more encouraging. Figure 1 shows the calculated effects of noise for the 20 participants for each of the dual task paradigms. Positive values indicate that noise improved listening effort, while negative values mean that noise made listening effort worse. As expected, the results demonstrate the expected effects of background noise, especially for listeners with hearing loss. However, the sizes of the effects vary with paradigm. When using the Simple and Complex paradigms, the effect of noise was not significant for listeners with normal hearing, and only listeners with hearing loss were affected by background noise. Furthermore, performance with the Complex paradigm was significantly less consistent and more variable.
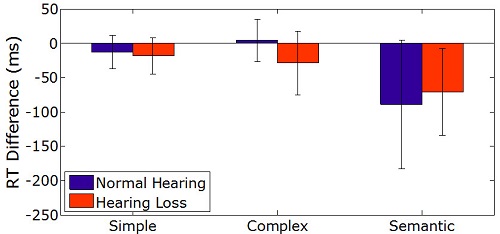
Figure 1. Mean effects of noise for three dual task paradigms for listeners with normal hearing (blue bars) and hearing loss (orange bars). Negative values indicate that noise increased listening effort. Effect of noise was statistically significant for listeners with hearing loss using all three tasks, and for listeners with normal hearing using the Semantic Paradigm. There was no significant difference between performance for listeners with normal hearing and hearing loss using the Semantic Paradigm. Error bars represent ±1 standard deviation from the mean.
The Semantic paradigm revealed significant effects of noise on listening effort for both groups of listeners. Indeed, Figure 1 demonstrates a potentially surprising finding - the listeners with normal hearing may have been more affected by background noise than listeners with hearing loss. We typically think of listeners with hearing loss as experiencing more difficulty in noise than listeners with normal hearing. However, this effect was not statistically significant and this trend may disappear as more data are collected. Conversely, this trend may become statistically significant as additional data are collected, in which case the effect may be related to the age difference between participants. Recall that the listeners with hearing loss were also older. Because this task is heavily language dependent, it may be that older listeners, who have more language experience, are more resilient to background noise using the Semantic task, which requires knowledge about language. This result, if significant, would be consistent with some other previous findings that older adults can use their language expertise to resist some peripheral auditory effects, like background noise (Pichora-Fuller, 2008).
In addition to the effects of background noise, we see a significant and consistent effect of hearing loss using all three reaction-time based dual task paradigms (Figure 2). Although all three paradigms revealed significant effects of hearing loss, the Complex paradigm revealed the largest effect. This effect is likely due to two outliers whose performance on the Complex paradigm was substantially poorer than other participants with the Complex paradigm, although they were not outliers using the other paradigms. This suggests that the Complex paradigm may be particularly challenging for some older listeners. Indeed, several older participants reported that understanding the task was difficult. However, once we collect additional data, this effect may no longer be significant. In addition, once we test more participants, we will better understand if these participants are true outliers or if their data are representative of some older listeners.
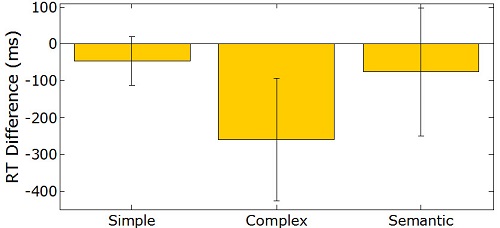
Figure 2. Mean effect of hearing loss for three dual task paradigms. Negative values indicate more listening effort for listeners with hearing loss. Performance from all three paradigms revealed significant effects of hearing loss; size of the effect was significantly larger with the Complex paradigm than with the Simple or Semantic paradigms. Error bars represent ±1 standard deviation from the mean.
19. Interesting, but what does all that mean?
These results suggest that the Semantic paradigm is a reliable measure and we plan to use this task in future studies investigating the effects of hearing aids and hearing aid technologies on listening effort. It has pretty good face validity because we’re asking listeners to make use of the language they hear. In addition, it’s not sensitive to the floor effects of recall tasks because it is a reaction time measure. Hopefully I can have some more answers for you in the future about what a clinician can do to help their patients who struggle with fatigue as a result of increased listening effort throughout the day.
20. Is there a take-away message out of all of this that I can implement in my practice?
I think the take-away message here is that listening effort probably affects many of our patients. It becomes particularly apparent in background noise or in other difficult listening situations. We think that hearing aids, and probably some hearing aid features, may improve listening effort. However, we don’t know for sure what kind of hearing aid technologies will be most effective, since we’re still developing a methodology to test listening effort that is as sensitive as possible. In our lab, we have developed a test that looks promising, so keep your eyes out for new results using this Semantic Dual Task paradigm.
References
Borg, G. (1990). Psychophysical scaling with applications in physical work and the perception of exertion. Scandinavian Journal of Work, Environment & Health, 16, 55-58.
Bradley, M. M., Greenwald, M.K., Petry, M.C., & Lang, P.J. (1992). Remembering pictures: Pleasure and arousal in memory. Journal of Experimental Psychology: Learning, Memory, and Cognition, 18, 379-390.
Downs, D. (1982). Effects of hearing aid use on speech discrimination and listening effort. Journal of Speech and Hearing Disorders, 47, 189-193.
Fraser, S., Gagne, J-P., Alepins, M., & Dubois, P. (2010). Evaluating the effort expended to understand speech in noise using a dual-task paradigm: The effects of providing visual speech cues. Journal of Speech, Language, and Hearing Research, 53, 18-33.
Gatehouse, S. & Gordon, J. (1990). Response times to speech stimuli as measures of benefit from amplification. British Journal of Audiology, 24, 63-68.
Gatehouse, S. & Noble, W. (2004). The Speech, Spatial and Qualities of Hearing Scale (SSQ). International Journal of Audiology, 43, 85-99.
Hallgren, M., Larsby, B., Lyxell, B., & Arlinger, S. (2005). Speech understanding in quiet and noise, with and without hearing aids. International Journal of Audiology, 44(10), 574-83.
Hicks, C., & Tharpe, A. (2002). Listening effort and fatigue in school-age children with and without hearing loss. Journal of Speech, Language, and Hearing Research, 45, 573 - 584.
Hornsby, B. W. (2013, February). The effects of hearing aid use on listening effort and mental fatigue associated with sustained speech processing demands. Ear and Hearing, published ahead of print.
Howard, C. S., Munro, K., & Plack, C.J. (2010). Listening effort at signal-to-noise ratios that are typical of the school classroom. International Journal of Audiology, 49, 928-932.
Larsby, B., Hallgren, M., Lyxell, B., & Arlinger, S. (2005). Cognitive performance and perceived effort in speech processing tasks: effects of different noise backgrounds in normal-hearing and hearing-impaired subjects. International Journal of Audiology, 44, 131-143.
Mackersie, C. L. & Cones, H. (2011). Subjective and psychophysiological indices of listening effort in a competing-talker task. Journal of the American Academy of Audiology, 22, 113-122.
McCoy, S., Tun, P., Cox, L., Colangelo, M., Stewart, R., & Wingfield, A. (2005). Hearing loss and perceptual effort: Downstream effects on older adults’ memory for speech. The Quarterly Journal of Experimental Psychology Section A, 58, 22-33.
McFadden, B., & Pittman, A. (2008). Effect of minimal hearing loss on children's ability to multitask in quiet and in noise. Language and Speech Hearing Services in Schools, 39, 342-351.
Meyers, M., & Smith, B.D. (1986). Hemispheric asymmetry and emotion: Effects of nonverbal affective stimuli. Biological Psychology, 22, 11-22.
Nachtegaal, J., Kuik, D.J., Anema, J.R., Goverts, S.T., Festen, J.M., & Kramer, S.E. (2009). Hearing status, need for recovery after work, and psychosocial work characteristics: Results from an internet-based national survey on hearing. International Journal of Audiology, 48, 684-691.
Ng, E. H. N., Rudner, M., Lunner, T., Pedersen, M.S., & Ronnberg, J. (2013). Effects of noise and working memory capacity on memory processing of speech for hearing-aid users. International Journal of Audiology, 1-9.
Partala, T., & Surakka, V. (2003). Pupil size variation as an indication of affective processing. International Journal of Human-Computer Studies, 59, 185-198.
Pichora-Fuller, K. M. (2008). Use of supportive context by younger and older adult listeners: Balancing bottom-up and top-down information processing. International Journal of Audiology, 47, S72-S82.
Pichora-Fuller, M.K., Schneider, B.A., & Daneman, M. (1995). How young and old adults listen to and remember speech in noise. Journal of the Acoustical Society of America, 97, 593-608.
Picou, E. M., Ricketts, T.A., & Hornsby, B.W. (2013, February). How hearing aids, background noise, and visual cues influence objective listening effort. Ear and Hearing, published ahead of print.
Rabbitt, P. (1991). Mild hearing loss can cause apparent memory failures which increase with age and reduce with IQ. Acta Oto-Laryngologica, 111, 167-176.
Sarampalis, A., Kalluri, S., Edwards, B., & Hafter, E. (2009). Objective measures of listening effort: Effects of background noise and noise reduction. Journal of Speech, Language and Hearing Research, 52, 1230-1240.
Zekveld, A.A., Kramer, S.E., & Festen, J.M. (2010). Pupil response as an indication of effortful listening: The influence of sentence intelligibility. Ear and Hearing, 31, 480-490.
Cite this content as:
Picou, E.M. (2013, August). 20Q: Listening effort - we know it’s a problem but how do you measure it? AudiologyOnline, Article 12032. Retrieved from: https://www.audiologyonline.com

