
Editor's note: This is an edited transcript of the live expert e-seminar presented on 9/29/10.
Introduction
Mark Ross said, "Appropriate amplification is the most important habilitative tool available for children with hearing loss." As audiologists, this means that selecting, fitting, verifying and validating amplification is one of the most important things we do for children with hearing loss. Looking at the specifics of speech perception performance can help us with these important clinical tasks in ensuring that each child we see receives the maximum benefit from his or her technology.
Goal of amplification
Our main goal in fitting technology for children is to assist them in hearing conversation at average and soft listening levels in both quiet and in competing noise. We want to maximize their auditory functioning to enable children to fully participate in every aspect of communication that occurs in their daily lives. Most children with hearing loss today are mainstreamed in regular classroom settings. That means that they have to use audition to learn. By contrast, 15 - 20 years ago, many children were educated in special education settings, especially those children with more significant hearing loss. That is not the case today, and therefore children with hearing loss must receive the maximum benefit with amplification in order to learn alongside their normal hearing peers.
To determine if we have succeeded in fitting technology appropriately we must assess it. We need to assess children's ability to hear normal and soft conversation in quiet and in competing noise otherwise there is no way of knowing if we've met our goal. With adults, you can use subjective reports, to a degree, to assess how they are doing with amplification. This is not the case with children. Asking how they are doing or if they are doing well in school does not assess what a child is hearing or exactly what he or she is not hearing.
Many audiologists fit technology using real-ear verification for hearing aids and using a computer program for cochlear implant mapping. Real-ear measurements provide valuable, objective information about sound pressure levels at the tympanic membrane. This is an important first step to fitting amplification, but it is only a first step. Real-ear measurements do not provide information about what the auditory brain is receiving or how the auditory brain is interpreting the information it is receiving. Real-ear measurements do not tell us what a child is actually hearing or how they are performing.
Real-ear prescriptive targets are based on the audiological information that we enter into the computer or real-ear system in order to program hearing aids. If the audiological information is limited, as it often is with young children, prescriptive targets will also be limited.
I recently participated in a consulting project where I saw 22 children who were using hearing aids fit appropriately as determined by real-ear measurements, but, when tested, were not performing well with their hearing aids.
We conducted speech perception testing and obtained noise band thresholds with each child in the sound booth and modified the hearing aid settings accordingly, and in each case we improved their overall performance. This demonstrates that in order to determine what a child is actually hearing with his or her amplification, we must measure it using speech perception testing.
Why test speech perception?
The purpose of speech perception testing is to assess the child's ability to both perceive and discriminate speech information. This has many clinical uses. First, we can assess the benefits of their technology. Information from speech perception testing can also be used to both plan and monitor habilitation. Lastly, information from speech perception testing will help us assess the child's auditory processing skills.
Using speech perception testing to measure outcomes with amplification
In my experience, speech perception testing is not typically used to assess outcomes with amplification. Speech perception is routinely tested under earphones when a child has a hearing evaluation. It is only occasionally tested after a child is fit with technology. Why would it be more important to measure speech perception with earphones than to measure speech perception with the technology that children live with everyday and rely on for communication? Unaided speech perception testing with earphones provides us with some information to help us select technology, but it does not predict how the technology will perform. Unless we test speech perception with the technology, we are not in a position to know how a child is hearing with amplification, how the amplification is performing, and what we must do as audiologists to ensure that each child is receiving the maximum benefit from amplification.
Speech perception testing can tell us about the benefit of hearing aids, cochlear implants, FM systems or a combination of technology. We want to know if the amplification is appropriate, if it is functioning, and if it is adequately performing. It may need to be modified in some way such as making programming changes to hearing aids, changing cochlear implant maps, or we may need to change the technology altogether. If a child is using hearing aids, he or she may need to move to power or superpower models, or perhaps a cochlear implant evaluation is in order. Maybe an FM system is needed.
Speech perception testing can also tell us how each ear performs with its amplification individually and how the ears perform together in the binaural condition. If testing is only conducted binaurally, we will not know if the child is getting more from one device than the other. The ears should be matched whenever possible, as it is our goal to have children be binaural listeners. We want them to use both ears and to be hearing the same in each, if possible. This is critical for localization and for understanding speech and in noise. We must test each ear separately in order to obtain this information.
Using speech perception to plan and monitor habilitation
Speech perception testing demonstrates the child's habilitative or rehabilitative needs. How is the child performing in the classroom? What are the situations in which we can expect him or her to be struggling in the classroom? It can give us information such as specific phoneme perception areas that can be very helpful for the teachers, parents and the auditory listening therapist. It also assists in selecting the appropriate educational environment. If a child can rely on hearing, we know we can keep that child in the mainstream. If she cannot, we either need to adapt the environment or find a different placement.
Speech perception testing can also be used to tell us what is happening over time. Audiologists are in an advantageous situation to determine how children are progressing over a period of time. The classroom teacher, parents, speech language pathologists, and auditory verbal therapists generally see children at least weekly and in many cases several times a week. As audiologists, we may see children every three or four months. This puts us in a much better position to determine if in fact, a child is making progress, and to monitor progress over time. Speech perception testing can identify problems that develop over time, such as when speech perception deteriorates. This could be due to equipment failure, a change in hearing or other reasons. For example, if there is something wrong with the cochlear implant microphone that distorts the signal, you will see this on speech perception testing where you may not see this with mapping. Speech perception testing with amplification will give us quantitative data to determine if progress is being made, and if not, it will provide us with the information necessary to intervene.
Using speech perception to examine auditory processing ability
Speech perception testing can indicate whether a child may be having auditory processing issues - both children with hearing loss and those with normal hearing. Although the focus of this course is on speech perception testing with amplification, speech perception testing can also be conducted with children with normal hearing who are suspected of having auditory processing issues. In this case, I conduct the testing in three conditions using four-talker babble noise: 50 dB HL with + 5 signal-to-noise ratio (SNR); 50 dB HL with 0 SNR; and 35 dB HL with 0 SNR. When I was at Long Island College Hospital a number of years ago, we tested approximately 187 children with normal hearing in those three conditions and they all scored 88% or better in all three conditions. So we know typically hearing children hear at 88% or better in these conditions, and significantly lower scores indicate the child is functioning below normal limits.
The answer to the question "Why test speech perception", can be summarized this way: If you do not test children's speech perception performance you do not know what the child is actually hearing and most importantly, you do not know what the child is not hearing. You do not know whether there has been a change in the child's perception ability and you do not know if there is something that you can do to improve auditory functioning.
Questions such as:
- Is the child receiving the maximum benefit from amplification in each ear?
- If not, why not?
- Are changes to the amplification settings in order?
- Do we need to change the amplification altogether?
- Is an FM system needed?
- Is this child getting what they need to hear and learn in school?
- Do they need assistance to hear better in school?
- Do we need to modify their educational program?
- What kind of auditory processing issues is the child having?
can be better addressed with information from speech perception testing.
Goals of aided speech perception testing
Speech banana or string bean?
We have established the fact that we need to test perception with amplification, and now we need to establish a goal for each child so we will know if they are optimally performing with their technology. Is 90% aided speech perception adequate? What about 50%? Does our goal depend on the hearing loss?
Some audiologists, and certainly most parents, look to the speech banana when it comes to aided benefit. We are all familiar with the speech banana, the banana-shaped area of the audiogram where typical speech sounds occur. The speech banana is typically used in counseling parents and teachers to demonstrate which speech sounds are audible and which are not due to a child's hearing loss.
What we need to consider, however, is that the speech banana was created to cover typical conversational speech which covers a wide range of intensity levels. Some phonemes of soft speech may occur at 15 dB HL, while some phonemes of speech at a normal conversational level may occur at 50 dB HL.
Therefore, your perception of those phonemes will vary greatly depending on exactly where within that speech banana your hearing thresholds fall. If you hear along the top (lowest intensity levels) of the speech banana, you will hear 90% of what is said in typical conversations. However, if you hear along the bottom (highest intensity levels) of the speech banana, you will only hear 10% of what is said in typical conversations. And if you hear somewhere along the middle of the speech banana, you will hear approximately 50% of what is said.
Traditionally, I think many audiologists and certainly most parents believe that if a child's aided responses fall anywhere within the speech banana, then we have achieved our goal with amplification. However, that is not the case. No one would accept hearing 10% of typical conversation as adequate for a child who is developing speech and language, and trying to learn via audition in a classroom setting. Unless a child is hearing along the top (lowest intensity levels) of the speech banana, he or she is missing a lot of what is being said, which is going to make it difficult to manage in a classroom.
Another tool that illustrates the importance of audibility is the Killion and Mueller "Count the Dots" audiogram that was developed in 1990 and recently updated (Killion & Mueller, 2010). Using the count the dots method we can estimate the audibility of speech inputs based on a child's hearing thresholds.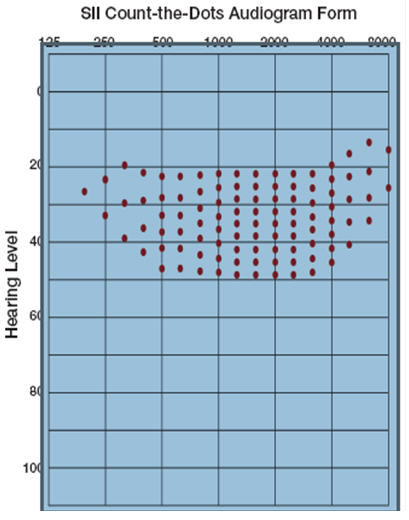
Figure 1. SII Count-the-dots Audiogram Form (Killion & Mueller, 2010).
There are 100 dots on the audiogram in Figure 1. If you overlay a child's hearing thresholds and count the dots that are within that child's range of hearing, you have an estimate of what percentage of speech is audible to that child (90 dots would be 90%, etc.). You can also use a child's aided thresholds to determine what percentage of speech is audible to the child when he or she is using amplification. Since each dot is worth 1%, you can also easily see that by missing only a few dots, a child is at a significant disadvantage.
In summary, our goal for aided performance is for every child to be at the top of the speech banana. I suggest we change the speech banana to a string bean. The top line of the speech banana - that is, the intensity levels where 90% of normal and soft conversational speech is audible across the frequency range - is our goal with amplification. If a child is hearing with their technology at this level, they are going to manage using audition, and if not, they are going to struggle.
Speech perception testing - who, when
Speech perception should be assessed with every child with a hearing loss on a regular basis both in the unaided and aided conditions. Whenever a child is seen for an audiological re-evaluation, speech perception should be assessed to monitor unaided performance. Aided performance should be assessed as well, both on a routine basis and whenever a change is made to the amplification. If the hearing aids need re-programming, or the cochlear implant map needs adjusting, speech perception testing needs to be conducted to ensure that those changes were beneficial, and not detrimental, to the child's performance.
Speech perception testing - how
Testing conditions
What are we looking for when we test speech perception with amplification? We want to know whether the child is hearing enough speech information with their technology and if they are hearing it at a soft level (35 dB HL) as well as at a normal conversation level (50 dB HL). If they're not hearing soft speech they are not going to hear someone who is standing more than 6 feet away, and their auditory bubble is going to be very small. That means that in many classroom situations they are going to be missing a lot.
During an audiological evaluation, speech perception testing is typically done at 40 dB above the SRT or PTA because we want to know how the child performs at optimal (loud) levels. It is not as useful to test speech perception performance for loud speech stimuli, because it is not representative of how they the child will perform in real-world situations such as in school. The only exception is when you have a child who has considerable difficulty understanding normal conversation. In this case, I may test at a louder level, such as 65 dB HL, to determine if the child will do better. In this way, I can determine if it is a perception problem or a problem that can be solved by making adjustments or changes to the technology.
We also want to know if the child is hearing throughout the frequency range and most importantly, in the high frequencies. The high frequencies are critical not only for the perception of consonants such sibilants and fricatives, but also for hearing important grammatical markers, such as /s/ which signals plural, possession, and contractions. Thus, hearing these sounds is not only important for understanding what is said, but also for speech and language development, and for academic skills such as reading.
In addition to testing speech perception at normal and soft conversational levels, we also need to measure how children hear in noise. Some children with hearing loss do well in noise and some do not, and we cannot predict or assume performance; we must measure it. For testing in noise, I recommend using a +5 signal-to-noise ratio (SNR) as it is typical of a classroom setting and will help us to understand how a child hears in school.
In terms of testing conditions, testing at a normal conversational level in quiet indicates how the child will function under optimal listening conditions. Testing at a soft conversational level provides a more realistic situation as compared to daily listening situations, while a normal conversational level with competing noise is most typical of everyday listening situations that children encounter.
Why do we need to test in more than one condition? Because we need to know how the child hears in a variety of situations and in noise and in quiet. To have the whole picture of how the child hears, we need to test in a variety of listening conditions.
Selecting materials
The key to selecting materials for speech perception testing is to select materials that are linguistically appropriate for the child, that is, that are neither too easy nor too hard.
I am frequently asked to review evaluations from children who have been seen at other facilities in my community and in other facilities around the world. Frequently, I notice that the tests used are too easy for the child. The Northwestern University - Children's Perception of Speech test or NU CHIPS (Elliot & Katz, 1980), for example, has vocabulary appropriate for children age 3 5 years. I have seen many children at a third or fourth grade level (8 or 9 years old) who were tested using the NU CHIPS. Older children will do very well with the NU CHIPS and then their test results will not be reflective of how they are actually hearing and discriminating age-appropriate vocabulary in their third or fourth grade classroom.
It is important that we know what the child's language level is and we select a test that is appropriate for that level. We want to know what their linguistic vocabulary is using audition only without the use of sign or speechreading since that is what we are trying to manage. We also need to know the child's cognitive level. As mentioned, a nine year old should not be assessed using a test that was that was designed for a four year old unless that nine year old is cognitively functioning at a four year old level.
Level of complexity
In addition to selecting a type of test, there are different levels of complexity in the tests that we use. Sentence tests are the easiest because you don't have to hear all the stimuli to understand the message. With sentence stimuli, what we are really testing is a person's ability to fill in the missing pieces. It is not necessarily providing accurate information about exactly what a person hears.
Monosyllabic words are a much more accurate measure of what a child hears because there are limited cues. The number of phonemes that the child has to remember or repeat are very few. Typically, three phonemes are used, in a consonant-vowel-consonant (CVC) word that the child has to identify either by pointing to pictures or repeating back the word.
Phoneme testing or phoneme scoring (scoring based on the number or percentage of correct phonemes of nonsense syllables however is the most reliable measure to use if we want to know exactly what a child hears. It is the most accurate measure of auditory perception as there are very few cues.
Open set v. closed set
In closed set measures, there are a limited number of choices. This is very useful with young children because their vocabulary is restricted. Closed set measures are also useful when you cannot understand the articulation of the person who is being tested. However, having a set number of responses to choose from can inflate performance so it is important to recognize that. We also have to be concerned about inappropriate use, or using closed set tasks with children who can perform open set tasks. For example, using picture pointing tasks such as Word Intelligibility by Picture Identification (WIPI) (Ross & Lerman, 1970) and NU CHIPS with older children in the mainstream as discussed earlier. Open sets are more challenging. The stimulus possibilities are unlimited and the results are more representative of what the child is likely to encounter in an everyday situation.
Speech perception tests for children
Once you have established the child's cognitive level and auditory vocabulary level, which test should you start with? If you are testing a child whose auditory language age is less than 2 years, the Early Speech Perception (ESP) test (Geers & Moog, 1989) is a good place to begin. If they have an auditory language age of 2 to 5 years, the NU CHIPS is a good place to begin. If a child has an auditory language age of 4 to 6 years, the WIPI is appropriate and if it is 5 up to 8 years, the Phonetically Balanced Kindergarten (PBK) (Haskins, 1949) list is appropriate. If the child has an auditory language age of 8 years and above they should be using adult materials such as CNC (consonant-nucleus-consonant) lists or the Northwestern University Auditory Test Number 6, commonly known as NU 6 lists.
Let me describe these tests briefly. The ESP, NU CHIPS and WIPI are picture identification tasks. The NU CHIPS is a four-alternative forced-choice test using monosyllabic words, and the words are not similar. The WIPI has six pictures to choose from for each stimulus, and the words are very similar, with usually only a consonant or vowel difference in at least four of the six words. This makes it a much more difficult test than the NU CHIPS. With the PBK, the child has to use audition alone and repeat the words, as with the CNC or the NU 6.
Presentation of stimuli
The way we present test stimuli can influence the test results. Results from stimuli presented via monitored live voice can be affected by rate and quality of the person speaking, which makes it highly variable from test session to test session. Therefore, it is difficult to determine test/retest reliability and to compare across sessions to see if perception is improving or deteriorating. It is sometimes useful with young children or others where flexibility is needed during the testing. However, using recorded stimuli is the goal and we can do recorded testing with very young children. Obtaining recorded NU CHIPS test results with a four-year-old is possible! You need to have your finger on the stop button of your CD player so you can stop it if the child gets distracted, but it can be done.
Putting it all together - developing a protocol
When you develop a test protocol, you need to keep in mind the purpose of your testing. The purpose is not to have the child obtain the best possible score. If that was your goal, you would use the easiest possible test and the most optimal test conditions. However, if the purpose of your testing is to monitor the child's technology, to determine if the amplification settings need to be modified, determine areas of need for habilitation/rehabilitation, and plan for educational placement as we have been discussing, then you need to select a more complex test protocol.
The general test protocol I recommend includes testing at normal conversational level (50 dB HL), soft conversational level (35 dB HL) and at normal conversational level in competing noise (50 dB HL with speech babble at +5 SNR). The following figures are adapted from the chapter on Speech Perception in Pediatric Audiology: Diagnosis, Technology and Management that I wrote with Carol Flexer (Madell & Flexer, 2008). The general test protocol is outlined in Figure 2.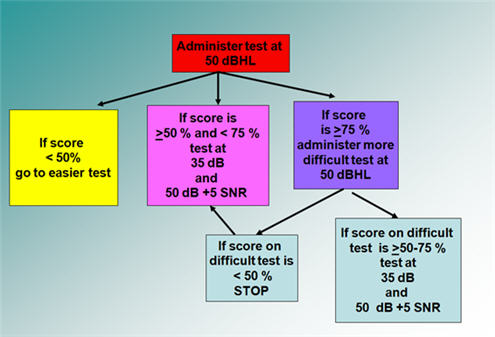
Figure 2. Speech perception testing protocol - general concept. Adapted from Madell & Flexer, 2008.
Begin by presenting the test at 50 dB HL with the child wearing his or her technology.
- If the child's score is less than 50% correct, you likely have picked a test that is too difficult for this child's level and you need to move to an easier test. If the child continues to perform poorly even after moving to an easier test, you can stop testing at that point.
- If the child's score is between> 50% - 75%, then you have picked a test that is appropriate for the child. Next, test at 35 dB HL and at 50 dB HL with +5 SNR using four-talker babble.
- If the child's score is more than 75%, the test is probably too easy. Administer a more difficult test. For example, if you have used the NU CHIPS change to the WIPI, or if you started with the WIPI go to the PBK. Or, if you used the WIPI or NU CHIPS and it is too easy, administer it in an open set manner without the pictures. Have the child repeat back the words, since you know they have the vocabulary level for the test. You may be surprised to know that many three-year-olds can complete an open set NU CHIPS. The NU CHIPS' vocabulary is appropriate for a three-year-old, and an open set task will give you a better sense of what they are hearing.
If the score on the difficult test is> 50 - 75% (see Figure 2, purple box) next test at 35 dB HL and at 50 dB HL with four-talker babble at a +5 SNR. If the child performs poorly in these conditions, you may either stop testing there, or try the easier test under these same conditions, 35 db HL and 50 dB HL with + 5 SNR.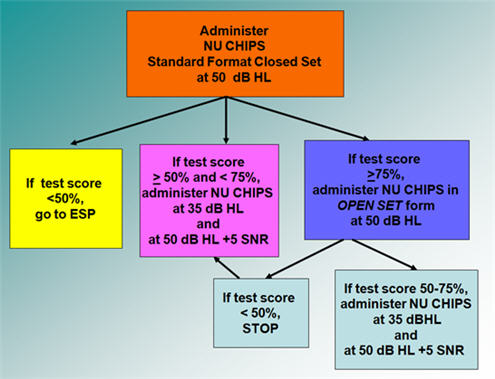
Figure 3. Speech perception testing protocol example using the NU CHIPS as the initial test, adapted from Madell & Flexer, 2008.
Figure 3 is an example protocol beginning with the NU CHIPS. In this case, you start testing by administering the NU CHIPS at 50 dB HL in the standard, closed set format.
- If the child performs poorly (< 50% correct), next administer the ESP because it is an easier test.
- If the child scores between> 50% and < 75%, next test at 35 dB HL and at 50 dB HL with + 5 SNR.
- If the child does well on the NU CHIPS (score> 75%), try the NU CHIPS in an open set format at 50 dB HL. If the score is> 50% - < 75%, then use the open set NU CHIPS for testing at 35 dB HL and at 50 dB HL with + 5 SNR. If they do poorly with an open set NU CHIPS at 50 dB HL, go back to the NU chips in a closed set format to test performance with soft speech and speech in noise.
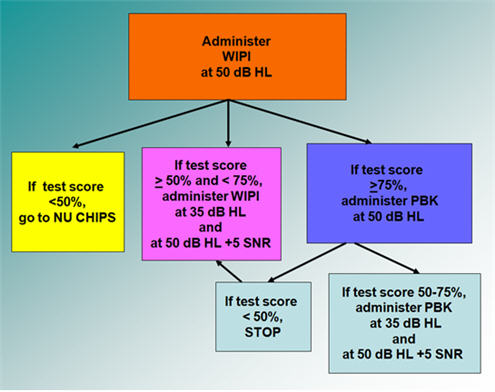
Figure 4. Speech perception testing protocol example using the WIPI as the initial test, adapted from Madell & Flexer, 2008.
Figure 4 is a similar example using the WIPI as the initial test. In this case, if the child does poorly on the WIPI, move to the NU CHIPS. If the child does well, test at a soft speech level and at normal conversational level with noise, and so forth. The protocol is the same as previously discussed, while the measures will differ depending on which one you select as your starting point. Figure 5 shows the same protocol with the PBK as the starting point.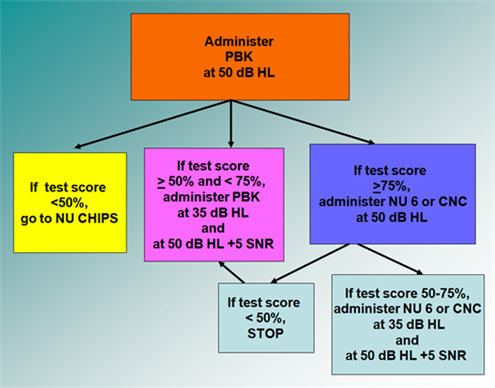
Figure 5. Speech perception testing protocol example using the PBK as the initial test, adapted from Madell & Flexer, 2008.
When you begin testing with the NU 6 or CNCs as shown in Figure 6, there is no need to move to more difficult tests if the child does well since the same materials are used to test adults. Once a child passes a second grade level, we should be using these measures instead of those designed for children.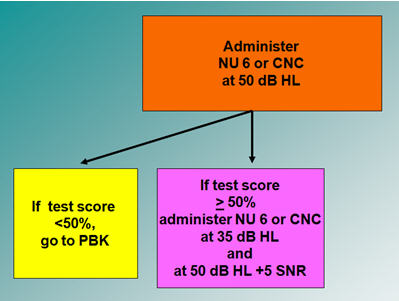
Figure 6. Speech perception testing protocol example using the NU 6 or CNC words as the initial test stimuli, adapted from Madell & Flexer, 2008.
Let me discuss a few more details about these protocols. As you can see, I recommend monosyllabic words as the primary test stimuli. Sentence testing will not provide any further information to help me figure out how to adjust the technology and will take valuable clinic time. I do not do sentence testing except when required for determining cochlear implant candidacy.
Earlier I stated that we need to know how each ear hears individually, and how the child hears in the binaural condition. Therefore, speech perception testing should be conducted in right only, left only and binaural conditions at a normal conversational level of 50 dB HL. Soft speech (35 dB HL) and speech in noise (50 dB HL +5 SNR) should be tested in at least the binaural condition.
Table 1 shows you the form I use for testing and recording speech perception test results. It has a lot of test conditions, and you do not have to fill in every box. However, the more you fill in, the more you will know about the child's auditory functioning. The more you know about functioning, the better chance you have to improve functioning by improving technology settings, providing information to the habilitation team about what to work on, assisting the school in knowing what to expect and how to plan to maximize functioning, and determining the need to change technology.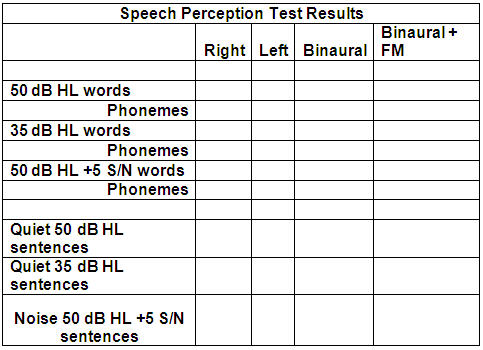
Table 1. Sample form for speech perception test results.
Normative data
All of the measures discussed here were normed on children with normal hearing. That, after all, is our goal; we want to know how the child we are testing compares to peers with whom they have to compete in their classroom. There are not different standards in my mind for speech perception performance for a child with a hearing loss. A child with hearing loss who is mainstreamed has to hear the same thing that every other child in the same classroom has to hear. My responsibility as the pediatric audiologist is to maximize the child's auditory performance.
Results of speech perception testing
Table 2 shows speech perception test results for one child.
Table 2. Binaural speech perception test scores for one child in a variety of test conditions.
If this child had been tested only at normal conversational level in quiet, we may have assumed that he is doing well, since the score was 84%. However, when you test this child in quiet and in competing noise, the scores dropped to 56% and 58%, which is poor performance.
So by testing in more difficult conditions, we can obtain a more realistic picture of every day performance. We can make better decisions about candidacy for technology. We can make better indications about the child's habilitative needs and make better educational placement recommendations. We can also provide better research and raise expectations for what people with hearing loss can do.
Factors to consider when reviewing results
When you look at test results, you need to consider the many factors that will have influenced those results, such as stimulus presentation, test format, presentation level, and listening condition.
In terms of stimulus presentation, the first thing to note is whether the test was performed using monitored live voice or recorded stimuli. You also want to know the level of difficulty of the test, and if it was appropriate given the child's level of functioning. Also note whether phoneme scoring or whole word scoring was used.
In terms of testing format, you need to know whether it was an open set or closed set format. Regarding presentation level - was it a normal, soft or loud conversational level, and was testing done in quiet or with competing noise? Lastly, determine if the testing was done with the child's right ear technology, left ear technology, binaurally with technology and if an FM system was also used. All of these factors will influence test results and need to be taken into account when assessing outcomes and making management decisions.
Other factors that may affect speech perception results include: degree of hearing loss, audiometric contour, length of hearing loss, auditory processing ability, experience using technology, primary language, language level, etiology of hearing loss, hearing aid settings or cochlear implant map strategy and rate, demands on audition in the family and educational setting, and finally, the experience of their audiologist or cochlear implant team.
Case studies
Case 1: David, age 6 years
Table 3 shows test results from David, a 6-year-old child with a profound hearing loss.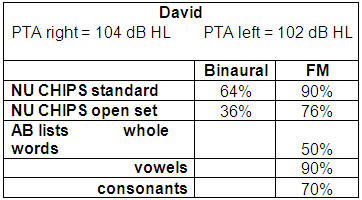
Table 3. Speech perception test results from 6-year-old child with profound hearing loss.
With this child, we started with the NU CHIPS because we determined it was appropriate for his level. He scored 64% on the standard NU CHIPS in the binaural condition, but when we used an open set format with no clues his score was 36%. With his FM system, however, his score was 90% in the standard format and 76% in an open set format. In this case we also used the AB list (Boothroyd, 1968), which is a CVC list scored by whole words, vowels correct and consonants correct. You can see by David's scores that he is getting all almost all the vowels, and although he is getting 70% of the consonants, he cannot put it together as he is only scoring 50% for whole words.
Case 2: Danny, age 7 years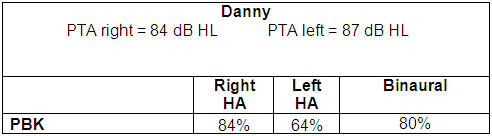
Table 4. Speech perception test results from 7-year-old child with severe hearing loss.
Table 4 shows test results from Danny, who is 7-years-old and has a severe hearing loss. If I had not tested speech perception results with his hearing aids in each ear separately, I would not have detected a problem. The disparity in his aided results - 84% in the right ear and 64% in the left ear - indicates that I need to try and improve the left ear technology so that he hears better with the left ear. If I cannot improve the left aided results, then I need to recommend to his therapist that he works on listening with the left hearing aid alone to build the skills and improve speech perception. In addition to working on left hearing aid listening in therapy, he should spend at least an hour or two a day after school listening with the left aid alone. In my experience over the years, I have seen that when we improve speech perception in the poorer performing ear, we improve the binaural speech perception as well.
Case 3: Miryam, 7 years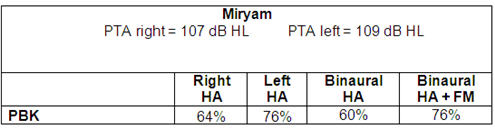
Table 5. Speech perception test results from 7-year-old child with severe hearing loss.
Table 5 shows results from a child whose poorer hearing right ear brought down the binaural score. She eventually got cochlear implants. However, had you only looked at the binaural score, you would not have known that the left hearing aid was doing better than the right. The individual ear information is very important clinical information that we need to obtain and use to plan intervention.
Case 4: Savy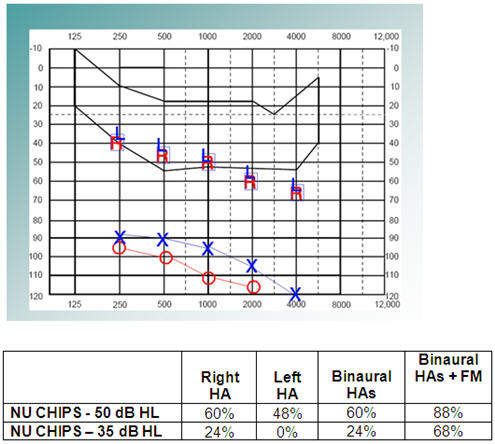
Figure 7. Savy, age 3 years. Aided and unaided thresholds on audiogram, and speech perception test results.
Figure 7 shows test results for Savy, a 3-year-old child with a profound hearing loss who uses hearing aids. As you can see, she is not getting a lot of benefit from her hearing aids, as aided thresholds are at the bottom of the speech banana. She was struggling with both her right and left hearing aids and performing especially poorly for soft speech. With both her hearing aids and FM she was doing well for normal conversation, but still struggling for soft speech.
Savy is now a teenager. At age 10, her right ear was implanted and she did much better, especially with sentences, but she still was having trouble with soft speech and struggling. She continued to wear a hearing aid on her left ear, and eventually, at age 16, her left ear was implanted. (Note: If this child's hearing loss were identified now she would likely have received binaural implants sooner.) Figure 8 shows her aided audiogram and speech perception test results post cochlear implantation.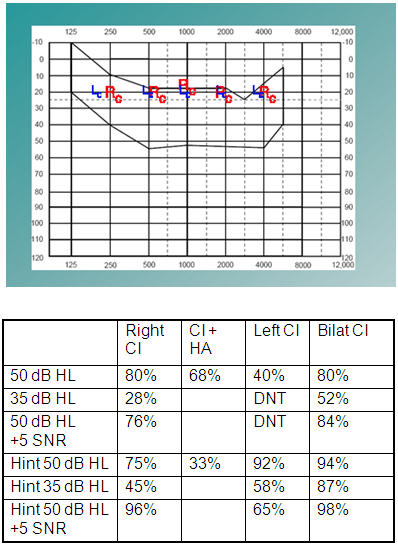
Figure 8. Savy's aided audiogram and speech perception test results post-cochlear implantation.
Although she received her right implant at age 10 ½, most of the testing shown in Figure 8 was done after she received her second implant at age 16. As you can see from the test results with bilateral implants, her test score at a normal conversational level in quiet remained at 80%, the same as using the right cochlear implant alone. Soft speech improved from 28% to 52%, but there was not a significant difference at normal conversation with + 5 SNR. Note the improvement with soft sentences - her score went from 45% using the right cochlear implant alone to 87% with both implants indicating that with limited additional cues she was able to do a much better job of filling in what she did not hear.
Case 5: L., 11 years old to 19 years old
Figure 9 shows test results from child L. when she was 11 years old. She has good aided thresholds with binaural hearing aids and an FM system.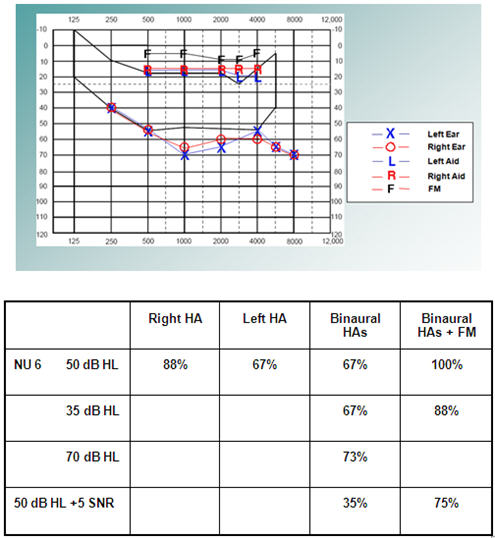
Figure 9. Audiogram including aided results and speech perception results for L, an 11-year-old child.
However, the speech perception score is better in the right ear and the binaural score is also significantly down compared to the right hearing aid alone. That tells us we have to do something to improve the left ear performance, such as listening therapy for the left ear.
I identified this child's hearing loss as a baby and they later moved out of the area and I stopped seeing her. At age 19, she went for a cochlear implant evaluation in another state and was told that she was not a CI candidate because her sentence score was 76%. At that time, she was a freshman at Yale. We know she is evidently very bright to have a profound hearing loss and get into Yale. I evaluated her with monosyllabic words and her scores were 12% in one ear, 14% in another ear, and 14% binaurally. You can see these results in Table 6. She was clearly struggling. She went on to get implanted and is now doing very well.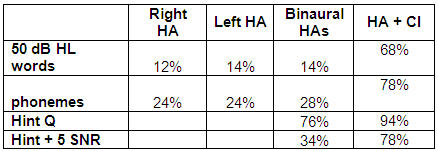
Table 6. Speech perception scores for L. at 19 years old.
Case 6 - D., 18 years old
The next case involves D., an 18-year-old who with a severe hearing loss in the left ear and a profound hearing loss in the right ear. Test results can be seen in Figure 10.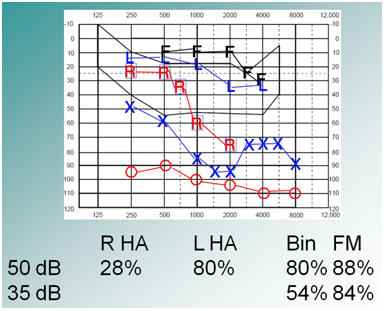
Figure 10. D.'s audiogram and speech perception test results (X = left unaided; O = right unaided; R = right hearing aid; L = left hearing aid; F = FM).
She was using hearing aids, and doing ok with the left aid, but not with the right, as you can see from the scores: 80% left and 28% right. Before she went to college, I decided that 28% word recognition in the right was not going to benefit her enough. I recommended that she consider a cochlear implant on the right side so that she could use two functioning ears in college. She was implanted on the right and her speech perception was significantly better in all conditions because she was now functioning using both ears. Test results post-cochlear implant can be seen in Figure 11.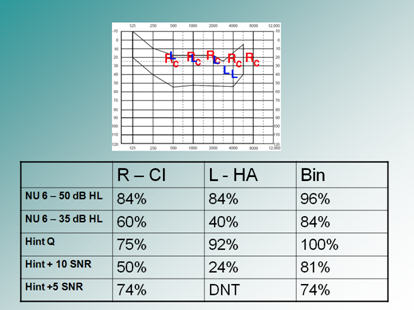
Figure 11. D.'s speech perception scores and aided audiogram post cochlear implantation on the right side (Rc = right cochlear implant; L = left hearing aid).
Using speech reception results: making management decisions
When evaluating test scores we want to look at normal versus soft versus loud presentation levels and consider how the child doing in all of these situations. Are the results comparable at all levels, and if not, what can we do to improve them? If speech perception is good at loud levels, the child has the ability to understand speech using audition. If scores are poorer at normal conversational levels, maybe the signal needs to be louder. If scores are good for a soft presentation level, then the child can hear at a distance of 10 feet.
Look at the results of the right ear versus the left ear - aided thresholds should be similar. If not, you need to determine if the poorer ear's results can be improved by adjusting/changing technology and/or working on auditory tasks with the poorer ear alone. As mentioned earlier, improving the poorer's ear performance will often improve binaural performance.
In addition, consider word versus phoneme scoring. Remember word scoring is a small part of the picture. We need to determine exactly what the child is misperceiving, for example, which frequencies are affected. This information can be used to try and adjust the technology accordingly. It is also important information for the auditory/verbal therapist, who should work on improving perception of the difficult to hear sounds
Speech perception results can be used in making educational decisions. If a child hears normal conversation in quiet he can hear someone 6 feet way. If they hear soft conversation they can hear someone 10 feet away, and if they can hear in noise they will be able to hear in the classroom setting. If they are not hearing well enough, we need to consider interventions in the classroom such as use of an FM system, captioning, an interpreter, a notetaker, and pre-post teaching. We also need to consider how they will manage in social situations. We need to ask ourselves the questions, "How good is good enough?" How does this child compare to children with normal hearing, to other children with hearing aids and to other children with cochlear implants? If children with cochlear implants do better, should a cochlear implant be considered?
Summary
Most children can use audition to learn and to communicate. Speech perception assessments can add significantly to improving performance and outcomes with amplification. Accurate assessment of auditory skills includes conducting speech perception testing and is a critical part of the pediatric audiologist's responsibility.
References
Boothroyd, A. (1968). Developments in speech audiometry. Sound (now British Journal of Audiology), 2,3-10.
Elliott, L.L. & Katz, D. (1980). Development of a new children's test of speech descrimination (Technical Manual). St. Louis, MO: Auditec.
Haskins, H. (1949). A phonetically balanced test of speech discrimination for children. Unpublished Master's thesis. Northwestern University, Evanston, Illinois.
Killion, M.C. & Mueller, H. G. (2010). Twenty years later: A NEW Count-The-Dots method. Hearing Journal,63(1), 10 - 15.
Geers, A.E. & Moog, J.S. (1989). Evaluating speech perception skills: Tools for measuring benefits of cochlear implants, tactile aids, and hearing aids. In E. Owens and D.K. Kessler (Eds.), Cochlear implants in young deaf children. CA: College-Hill Press, pp 227-256.
Madell, J. & Flexer, C.A. (2008). Pediatric audiology: Diagnosis, technology, and management. NY: Thieme.
Ross, M. & Lerman, J. (1970). A picture identification test for hearing-impaired children. Journal of Speech and Hearing Research, 13, 44-53.
Cite this Article as:
Madell, J. (2011, February 7). Pediatric amplification: Using speech perception to acheive best outcomes. AudiologyOnline, Article 841. Retrived from https://www.audiologyonline.com/

