
Providing amplification for infants and children is an increasingly complex and challenging endeavor for pediatric audiologists. Rapid innovation in hearing aid signal processing has provided new opportunities for maximizing audibility and minimizing the negative perceptual consequences of noise. At the same time, novel approaches to hearing aid features also create new challenges related to the selection and verification of these features for children. While researchers attempt to keep pace with these developments, clinicians must make decisions about whether or not such features should be used with children. If such features are determined to be appropriate, verification must be completed to ensure that the audibility of speech is maintained and that the recommended maximum output not be exceeded. The purpose of the current review is to provide clinicians with an evidence-based overview of the challenges related to the selection and verification of hearing aid features for infants and young children. An overview of basic selection and verification issues related to pediatric amplification will be highlighted. Additionally, considerations and recommendations for verification related to additional features and signal processing will be presented.
Fundamentals of pediatric hearing aid selection and verification
Although more comprehensive reviews of the process of providing amplification for children are available elsewhere (e.g. Bagatto, Scollie, Hyde & Seewald, 2010; Bagatto & Scollie, 2011), a brief review of the goals and desired outcomes of providing hearing aids for children serves as an important framework for evaluating advanced signal processing options for children. The primary goal of providing amplification for children with hearing loss is to make speech audible to minimize the impact of hearing loss on speech and language development. Therefore, questions about whether or not specific hearing aid features or signal processing strategies are appropriate for children should be based on how those features impact the audibility of speech. Likewise, verification of features should provide clinicians with evidence that audibility is not reduced when such features are activated. Clinicians must also consider the environments, listening behavior, and age of children to help to determine whether or not verification measures provide an accurate estimate of how the feature will be used in realistic environments. For example, while the directional microphone system verification method presented in the current review may indicate that the directional microphones provide a significant advantage for sounds in front of the child, the child's ability to orient towards the talker of interest (Ricketts & Galster, 2008) and the impact of features on incidental learning (Moeller, 2010) could affect the degree of benefit in everyday environments.
For infants who have undergone an electrophysiological assessment of hearing sensitivity with ABR, thresholds must be corrected prior to being used as the basis for hearing aid fitting. Because the dB HL calibration upon which behavioral threshold data are based was collected using relatively long-duration pure tone signals, equivalent ABR thresholds obtained with brief tones should be reduced to account for the elevation in threshold that occurs with brief stimuli due to temporal integration. Two methods exist to account for the difference between the behavioral HL and equivalent brief tone thresholds: 1) measurement of behavioral thresholds for ABR brief tone stimuli can be measured for normal hearing listeners to develop local normative data (Gorga et al., 2006), or 2) frequency-specific correction factors can be applied to ABR thresholds to account for the reduction in threshold for brief-tone stimuli (Bagatto et al., 2005; Stapells, 2000). Regardless of the method used to account for the difference, thresholds that have been corrected should be reported as estimated HL (eHL) and thresholds without correction should be reported as nHL. Failure to accurately report or account for these differences can lead to significant errors in threshold estimation and the subsequent hearing aid fitting.
Prior to assessment of advanced features, verification of the audibility of speech and maximum output should be completed using probe microphone measures and generic prescriptive methods (Bagatto & Scollie, 2011). Most audiologists primarily use the current Desired Sensation Level (DSL v5.0a) method for pediatric patients, although recent series of comparative validation studies have provided support for previous versions of both the National Acoustics Lab (NAL-NL1) and Desired Sensation Level (DSL 4.1) prescriptive methods with children (Ching et al. 2010). Individual ear canal acoustics should be accounted for during verification by either using real-ear probe microphone measurements with the hearing aid in the child's ear or corrected 2cc coupler measurements using the child's measured real-ear-to-coupler-difference (RECD). When probe microphone measures of the child's individual ear canal acoustics cannot be obtained, an average RECD based on the child's age has been found to be more accurate than using manufacturer's proprietary algorithms (Seewald, Mills, Bagatto, Scollie & Moodie, 2008), but less accurate than measuring real-ear or RECD. The measurement of behavioral thresholds using the child's earmold coupled to the tubing of the insert earphones is recommended by the University of Western Ontario (Bagatto & Moodie, 2007). For this reason, the Audioscan Verifit applies the child's earmold RECD to threshold data when auditory brainstem response (ABR), insert+foam or insert+mold are selected as the transducer. For clinics that measure behavioral thresholds with foam insert tips, application of the earmold RECD to behavioral threshold introduces potential for error as acoustic attributes of the earmold are applied to thresholds. Although the magnitude and direction of the error have not been adequately documented, the differences are likely to be largest for earmolds with acoustic tubing or bore modifications that would not occur in foam insert couplings. Clinicians should be aware of these differences and the potential impact on estimates of behavioral threshold and audibility.
Hearing aid verification should be completed using real-ear measurements or coupler measurements based on the patient's RECD. The audibility of speech should be verified over a range of input levels, including soft, average and loud speech. DSL m i/o provides prescriptive targets for multiple input levels to provide clinicians with guidance on how the hearing aid(s) should be set for each level. The maximum output (MPO) of the hearing aid should also be verified using a swept pure-tone signal at 85 or 90 dB, depending on the verification equipment. Importantly, interactions between some manufacturers signal processing and the swept pure tone used for verification of MPO can lead to inaccurate estimates of MPO. The most common solution at this time is to verify MPO with the hearing aid attached to the programming software in a verification mode that disables signal processing features that interact with the verification signals. Therefore, clinicians should follow manufacturer recommendations for verifying MPO accurately until these issues can be resolved. After the audibility of speech has been measured across a range of input levels and the MPO verified for each ear, clinicians must consider which advanced features may be appropriate for the child and how the impact of the selected features on audibility can be quantified.
Feedback management
Acoustic feedback can be a significant challenge in pediatric hearing aid fittings, particularly as infants and young children outgrow their earmolds. The impact of feedback management signal processing on children has not been specifically studied, but studies with adults (Freed & Soli, 2006) suggest that hearing aids with feedback management activated can result in greater high-frequency gain than when the setting is deactivated. Because maximizing the amount of high-frequency gain in pediatric hearing aid fittings is important for supporting speech perception (Stelmachowicz, Pittman, Hoover, Lewis & Moeller, 2004), the use of feedback management for children is recommended as long as the strategy does not result in significant reductions in high-frequency gain. Feedback management strategies should not be used to extend the usefulness of a poorly fitting earmold, as other factors such as physical comfort and reduced low-frequency gain due to slit leaks may occur before feedback becomes problematic. The gain and maximum output of the device should be verified after activation of feedback management to characterize any changes in frequency response that may occur. Because feedback is not realistically simulated in the coupler, real-ear measurements may provide a more accurate estimate of the effect of feedback management on audibility.
Digital noise reduction
Digital noise reduction (DNR) refers to signal processing strategies that reduce gain in response to background noise in an attempt to limit negative perceptual consequences. Although a wide range of strategies are used in different manufacturers' products, DNR algorithms that use modulation-detection to classify the input to the hearing aid as either primarily speech or background noise are commonly used (Kates, 2008). Implementation of DNR systems in hearing aids varies widely across manufacturers and may also vary based on the stimulus input level, activating signal, activation time, frequency range where gain is reduced, and audiogram of the listener (Hoetink, Korossy & Dreschler, 2009). Differences in implementation and the proprietary nature of these algorithms introduce challenges for clinicians who must determine if these algorithms are appropriate for children. Because DNR algorithms use gain reduction and the frequency range of speech and noise signals in realistic environments typically overlap, DNR is unlikely to result in significant changes in the signal-to-noise ratio (SNR) that would be required for improved speech perception. Consistent with this aspect of DNR, studies with adults have consistently reported that speech recognition in noise is similar with and without DNR (Bentler & Chiou, 2006). However, studies with adults have suggested that DNR signal processing can improve listening comfort and ratings of sound quality in noise (Mueller, Weber & Hornsby, 2006). Although the primary goal of providing amplification is to make speech audible, maintaining a comfortable signal for the child across a wide range of realistic environments is also vitally important.
The extent to which DNR can improve sound quality and listener comfort while maintaining speech recognition in children has been evaluated in several recent studies. Stelmachowicz and colleagues (2010) reported that perception for nonsense syllables, monosyllabic words and sentences was not significantly altered by the use of DNR in a group of school-age children with hearing loss. Gustafson and colleagues (2011) also recently reported data that suggest that children with normal hearing showed either stable or slightly improved phoneme recognition with DNR and that DNR reduced verbal response time and improved children's ratings of clarity. Recent work by Pittman (2011a, 2011b) suggests that DNR may result in increased ease of complex listening tasks such as word categorization in children with hearing loss. Collectively, studies with children suggest that as long as the audibility of speech is not compromised, DNR may have benefits for listener comfort, sound quality and cognitive processes. Further studies are needed with younger children and children with greater degrees of hearing loss who may be more susceptible to changes in audibility that may occur with DNR.
If DNR is determined to be appropriate, verification strategies must demonstrate that the audibility of speech is not compromised when speech and noise are presented to the hearing aid. One method that allows simultaneous presentation of speech and steady-state noise is in the Directional Test Mode of the Audioscan Verifit. Although this mode was developed for assessment of directional microphones, clinicians can measure speech and noise simultaneously in the test box using a fixed omnidirectional microphone response to determine how DNR may influence the audibility of speech. With the hearing aid in the test box, the response of the hearing aid with DNR deactivated should be measured with speech and noise in the coupler. The measurement will result in two overlapping lines that represent the response of the hearing aid to speech and noise with DNR off. Using the same parameters, a measurement should be taken with the DNR at use settings. The DNR-off and DNR-on curves are then compared to assess the influence of DNR on hearing aid gain. In most cases, the measurement will be the same, as in Panel B of Figure 1. In some cases, however, the gain of the hearing aid may be reduced with DNR on, as in Panel A of Figure 1. Clinicians must determine if the degree of change is sufficient to negatively impact audibility. In such cases, an alternate DNR setting that has less impact on the audibility of speech should be used. The level of the verification signal can also be changed to evaluate the level-dependencies of specific DNR algorithms.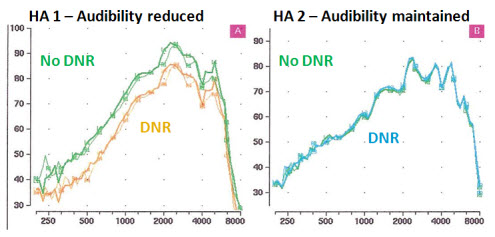
Figure 1. Verification results of digital noise reduction from two different hearing aids. In both panels, the green lines represent the response of the hearing aid with speech and noise (65 dB at a +3 dB SNR) without digital noise reduction (DNR). In Panel A, the orange lines represent the response of the hearing aid with DNR activated and a reduced response. In Panel B, the blue lines represent the response of the hearing aid with DNR activated and no reduction in response. Click Here for larger view (PDF)
Directional Microphones
Hearing aids with directional microphones typically use multiple microphones to minimize amplification of sounds coming from specific directions and maintain amplification for sounds occurring in front of the listener. The use of directional microphones has been shown empirically to improve the SNR and adults' speech understanding, particularly when the talker and noise are spatially separated and the noise is behind the listener (see Amlani, 2001, for review). Given the fact that children are more susceptible to the negative effects of noise than adults, directional microphones may provide a method of improving the SNR that could lead to improvements in speech understanding. Research by Gravel and colleagues (1999) revealed that in a laboratory setting with speech at 0 degrees and noise at 180 degrees, children had improved speech recognition in noise with directional microphones compared to an omnidirectional microphone. Subsequent studies with school-age children in more realistic educational settings have suggested that the benefits of directional microphones are dependent on the location of the talker of interest (Ricketts, Galster & Tharpe, 2007). When the talker of interest is in front of the listener, directional microphones resulted in improved speech recognition in diffuse noise compared to omnidirectional microphones. However, for situations where the talker of interest is beside or behind the listener, speech recognition with directional microphones was either equivalent or degraded. Therefore, the benefits of directional microphones appear to depend on the location of the talker and noise, as well as the ability of the listener to orient towards the speaker of interest. In a follow-up study, looking behavior was measured in school-age children (Ricketts & Galster, 2008), and children in this age were able to accurately allocate visual attention towards the teacher or talker of interest in realistic educational settings. Collectively, these results suggest that directional microphones may be appropriate for school-age children, particularly in situations where use of frequency-modulation (FM) systems may be impractical, such as a classroom discussion with multiple talkers. For infants and younger children, research is less clear about the advantages and limitations of directional microphones. One study of looking behavior in infants and young children with hearing loss suggested that infants and young children with hearing loss orient towards the talker of interest less than half the time in realistic situations (Ching et al., 2009). Research on incidental learning in young children with hearing loss (Moeller, 2010) suggests that children may use overhearing to learn new vocabulary. The impact of directional microphones on incidental learning remains unresolved, but given that incidental learning occurs even when the child is not allocating visual attention towards a talker, the potential negative impact on young children's ability to learn new words should be considered.
If directional microphones are determined to be appropriate, audiologists must verify how directionality may influence the audibility of speech. One method of verifying the function of directional microphones requires hearing aid verification equipment with two speakers, such as the Audioscan Verifit. Using the directional test mode in the Verifit, clinicians can quickly document the directionality of a hearing aid and any changes in the frequency response of the hearing aid that occur when directional microphones are activated. With the hearing aid appropriately oriented towards one speaker and the hearing aid attached to the programming software, recordings of the hearing aid in a fixed omnidirectional and then a fixed directional setting should be completed. In the omnidirectional setting, the response of the front and back speakers should be equivalent, as evidenced by overlapping responses (Green lines - Figure 2). In the directional setting, the response of the front speaker should be maintained, while the response of the back speaker should be reduced, reflecting the directionality (Blue lines - Figure 2). Any changes in the frequency response of the hearing aid and the impact that these changes have on audibility should be carefully appraised. While this method is efficient for documenting directionality, this verification method may not be appropriate for adaptive or auto-switching directional microphone systems.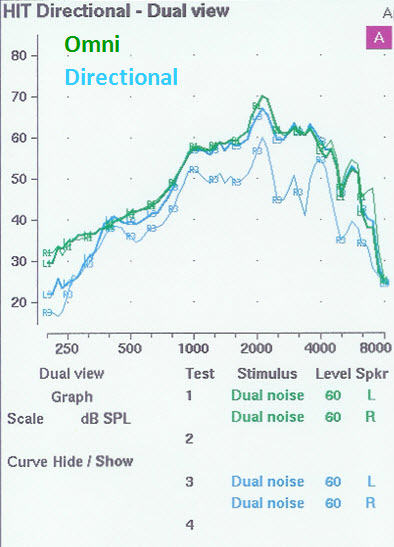
Figure 2. Results from a directional test on the Audioscan Verifit. The green tracing represents the response of the hearing aid in a fixed omnidirectional microphone setting, whereas the blue lines represent the response of the front and back microphones in a fixed directional microphone setting. Click Here for larger view (PDF)
Frequency-lowering signal processing
Multiple research studies over the past decade have highlighted the importance of high-frequency amplification for maximizing speech understanding (Stelmachowicz et al., 2004) and word learning (Pittman, 2008) in children. Studies with adults also suggest that providing a wider bandwidth results in improved ratings of sound quality for music and speech (Moore & Tan, 2003). Attempts to extend the audible bandwidth of hearing aids have been limited by several factors. Because the level of the speech signal decreases significantly at higher frequencies, the ability to extend the bandwidth up to 10 kHz requires a substantial amount of gain and may be achievable for only a portion of listeners with only mild to moderate hearing losses (Moore, Stone, Fullgrabe, Glasberg & Puria, 2008). As an alternative, multiple hearing aid manufacturers have implemented frequency lowering technology to relocate high-frequency speech cues to lower frequencies where the degree of hearing loss is less and hearing aids are able to provide more amplification. One available strategy is Phonak's SoundRecover, which uses nonlinear frequency compression (NLFC) above a specified start frequency to lower high-frequency speech energy into an audible range. NLFC has been evaluated in several studies with children (Glista et al., 2009; Wolfe et al., 2010; Wolfe et al., 2011). While the strategy of maximizing high-frequency audibility for children is justified based on previous research, clinicians must determine the appropriate settings for NLFC to ensure that the audible bandwidth of the signal is maximized, while minimizing potential negative outcomes associated with distortion of the speech spectrum that may occur with frequency lowering.
One method for determining the combination of start frequency and compression ratio that maximizes the audible bandwidth has been proposed by Alexander (2009). This method can be implemented using a free Microsoft Excel spreadsheet known as the SoundRecover Fitting Assistant (email [email protected] to request a copy) that allows a comparison of the frequency range that is audible to the listener with and without NLFC. To estimate the listener's audible bandwidth, an average speech signal is recorded through the hearing aid matched to DSL targets without NLFC. The point where the uncompressed average speech spectrum (middle line on the Audioscan Verifit) crosses the audiogram is the maximum audible frequency (Figure 3).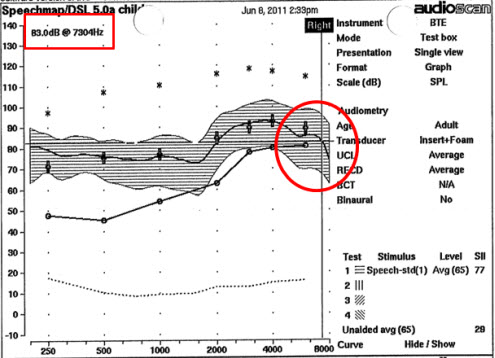
Figure 3. The maximum audible frequency is the highest frequency where the response of the hearing aid to average speech crosses the audiogram. The hearing aid should be matched to DSL targets. Click Here for larger view (PDF)
The maximum audible frequency is entered into the SoundRecover Fitting Assistant and used to select the optimal combination of start frequency and compression ratio, defined as the combination of results in the widest audible bandwidth for the listener (Figure 4).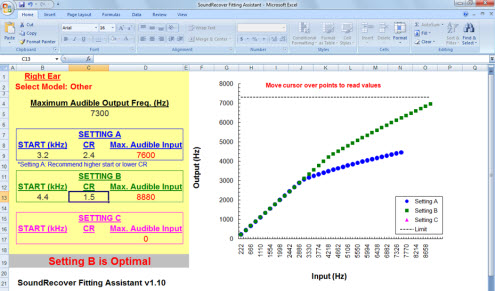
Figure 4. Results from the SoundRecover Fitting Assistant for the manufacturer's default start frequency and compression ratio (blue) and an optimized combination of parameters (green) for the audiogram and maximum audible frequency from Figure 3. Note the difference in the maximum audible input for each setting. Click Here for larger view (PDF)
While the SoundRecover Fitting Assistant does provide a starting point for selecting the parameters that are likely tomaximize audibility for the patient, this process does not constitute verification. An excellent review of the verification process for SoundRecoveris available on AudiologyOnline (Glista & Scollie, 2009). Once an optimal setting is determined, the gain and maximum output of the hearing aid must be verified with the prescribed compression setting activated. The compressed signal should match DSL targets for as much of the audible range as possible. Additionally, the audibility of specific filtered narrow bands available in the Audioscan Verifit may be used to estimate the audibility of specific high-frequency regions, such as 6300 and 4000 Hz. However, because the regions where these narrow bands are compressed contain additional energy outside of these bands, the hearing aid response should not be altered to make these narrow bands match targets. Such efforts may result in overall gain and maximum output that exceed DSL prescriptive targets.
Conclusions
Clinicians who provide amplification for infants and children are faced with significant challenges in determining the appropriate hearing aid features to use with their patients and how to verify the impact of these features on audibility. An appropriate selection and verification protocol for children should take into account the unique listening needs and behaviors of children, while focusing on the fundamental need to maintain speech audibility. Using the proposed protocols will allow clinicians to document that speech audibility is maintained in an efficient manner. On-going developments in hearing aid technology and signal processing may require adaptations of the current protocols, but the recommended measurements can provide a starting point for clinicians who want to document the efficacy of advanced technology with their pediatric patients.
References
Alexander, J. (2009). SoundRecover fitting assistant. Available by emailing [email protected]
Amlani, A. M. (2001). Efficacy of directional microphone hearing aids: a meta-analytic perspective. Journal of the American Academy of Audiology, 12(4), 202-14.
Bagatto, M., Moodie, Sheila, Scollie, S., Seewald, R., Moodie, Shane, Pumford, J., & Liu, K. P. R. (2005). Clinical protocols for hearing instrument fitting in the Desired Sensation Level method. Trends in amplification, 9(4), 199-226.
Bagatto. M. & Moodie, S.T. (2007) Learning the art to applying the science: Common questions related to pediatric hearing instrument fitting. AudiologyOnline Retrieved August 1, 2011 from www.audiologyonline.com/articles/article_detail.asp?article_id=1886.
Bagatto, M., Scollie, S. D., Hyde, M., & Seewald, R. (2010). Protocol for the provision of amplification within the Ontario infant hearing program. International Journal of Audiology, (49) Suppl 1, S70-9. doi:10.3109/14992020903080751
Bagatto, M. & Scollie, S.D. (2011). Current approaches to the fitting of amplification to infants and young children. In R. Seewald & A.M. Tharpe, Comprehensive handbook of pediatric audiology (pp. 527-552). San Diego, CA: Plural Publishing.
Bentler, R., & Chiou, L. K. (2006). Digital noise reduction: An overview. Trends in Amplification, 10(2), 67-82.
Ching, T. Y. C., O'Brien, A., Dillon, H., Chalupper, J., Hartley, L., Hartley, D., et al. (2009). Directional effects on infants and young children in real life: Implications for amplification. Journal of Speech, Language, and Hearing Research, 52(5), 1241-54. doi:10.1044/1092-4388(2009/08-0261)
Ching, T.Y.C., Scollie, S.D., Dillon, H. & Seewald, R. (2010). A cross-over, double-blind comparison of the NAL-NL1 and the DSL v4.1 prescriptions for children with mild to moderately severe hearing loss. International Journal of Audiology,49,S4-S15.
Freed. D.J. & Soli, S.D. (2006) An objective procedure for evaluation of adaptive antifeedback algorithms in hearing aids. Ear and Hearing, 27(4),382-98.
Glista, D. & Scollie, S.(2009). Modified verification approaches for frequency lowering devices. AudiologyOnline Article #2301. Accessed February 21,2012 from: www.audiologyonline.com/Articles/pf_article_detail.asp?article_id=2301
Glista, D., Scollie, S., Bagatto, M., Seewald, R., Parsa, V., & Johnson, A. (2009). Evaluation of nonlinear frequency compression: clinical outcomes. International Journal of Audiology, 48(9), 632-44. doi:10.1080/14992020902971349.
Gorga, M. P., Johnson, T. A, Kaminski, J. R., Beauchaine, K. L., Garner, C. A, & Neely, S. T. (2006). Using a combination of click- and tone burst-evoked auditory brain stem response measurements to estimate pure-tone thresholds. Ear and hearing, 27(1), 60-74. doi:10.1097/01.aud.0000194511.14740.9c
Gravel, J.S., Fausel, N., Liskow, C., & Chobot, J. (1999). Children's speech recognition in noise using omni-directional and dual-microphone hearing aid technology. Ear and Hearing, 20(1), 1-11.
Gustafson, S. J., McCreery, R. W., Hoover, B., Kopun, J. G., & Stelmachowicz, P. G. (2011, March). Ease of listening and speech recognition with digital noise reduction for normal-hearing children. Poster presented at the Scientific meeting of the American Auditory Society. Scottsdale, AZ.
Hoetink, A. E., Körössy, L., & Dreschler, W. A. (2009). Classification of steady state gain reduction produced by amplitude modulation based noise reduction in digital hearing aids. International Journal of Audiology, 48(7), 444-55. doi:10.1080/14992020902725539
Kates, J.M. (2008) Digital hearing aids. San Diego, CA: Plural Publishing.
Moeller, M.P. (2010, April) Optimizing word learning in infants with hearing loss. Marion Downs Lecture: Audiology NOW! San Diego, CA.
Moore, B. C. J., & Tan, C.-T. (2003). Perceived naturalness of spectrally distorted speech and music. The Journal of the Acoustical Society of America, 114(1), 408. doi:10.1121/1.1577552
Moore, B. C. J., Stone, M. A, Füllgrabe, C., Glasberg, B. R., & Puria, S. (2008). Spectro-temporal characteristics of speech at high frequencies, and the potential for restoration of audibility to people with mild-to-moderate hearing loss. Ear and Hearing, 29(6), 907-22. doi:10.1097/AUD.0b013e31818246f6
Mueller, H. G., Weber, J., & Hornsby, B. W. Y. (2006). The effects of digital noise reduction on the acceptance of background noise. Trends in Amplification, 10(2), 83-93. doi:10.1177/1084713806289553
Pittman, A. L. (2008). Short-term word-learning rate in children with normal hearing and children with hearing loss in limited and extended high-frequency bandwidths. Journal of Speech, Language, and Hearing Research, 51, 785-797.
Pittman, A.L. (2011a). Children's performance in complex listening conditions: Effects of hearing loss and digital noise reduction. Journal of Speech, Language, and Hearing Research, 54, 1224-39.
Pittman, A.L. (2011b). Age-related benefits of digital noise reduction for short-term word learning in children with hearing loss. Journal of Speech, Language, and Hearing Research, 54, 1448-63.
Ricketts, T., Galster, J., & Tharpe, A. M. (2007). Directional benefit in simulated classroom environments. American Journal of Audiology, 16(2), 130-44. doi:10.1044/1059-0889(2007/017)
Ricketts, T. A., & Galster, J. (2008). Head angle and elevation in classroom environments: implications for amplification. Journal of Speech, Language, and Hearing Research, 51(2), 516-25. doi:10.1044/1092-4388(2008/037)
Seewald, R., Mills, J., Bagatto, M., Scollie, S., & Moodie, S. (2008). A comparison of manufacturer-specific prescriptive procedures for infants. Hearing Journal, 61(11), 26-34.
Stapells, D.R. (2000). Threshold estimation by the tone-evoked auditory brainstem response: A literature meta-analysis. Journal of Speech-Language Pathology and Audiology, 24,74-83.
Stelmachowicz, P. G., Pittman, A. L., Hoover, B. M., Lewis, D. E., & Moeller, M. P. (2004). The importance of high-frequency audibility in the speech and language development of children with hearing loss. Archives of Otolaryngology-Head & Neck Surgery, 130(5), 556-62. doi:10.1001/archotol.130.5.556
Stelmachowicz, P., Lewis, D., Hoover, B., Nishi, K., McCreery, R., & Woods, W. (2010). Effects of digital noise reduction on speech perception for children with hearing loss. Ear and Hearing, 31(3), 345-55. doi:10.1097/AUD.0b013e3181cda9ce
Wolfe, J., John, A., Schafer, E., Nyffeler, M., Boretzki, M., & Caraway, T. (2010). Evaluation of nonlinear frequency compression for school-age children with moderate to moderately severe hearing loss. Journal of the American Academy of Audiology, 21(10), 618-28. doi:10.3766/jaaa.21.10.2
Wolfe, J., John, A., Schafer, E., Nyffeler, M., Boretzki, M., Caraway, T., & Hudson, M. (2011). Long-term effects of non-linear frequency compression for children with moderate hearing loss. International Journal of Audiology, 50(6), 396-404. doi:10.3109/14992027.2010.551788
Pediatric Hearing Aid Fittings: Selection and Verification of Features
November 14, 2011
Continued and its subsidiaries provide professional education authored by qualified Subject Matter Experts for continuing education purposes. These materials are intended for educational purposes and do not constitute medical advice or a substitute for individual clinical judgment. Continued is not a clinical healthcare provider; the licensed professional is solely responsible for ensuring that the application of any techniques or information presented is within their legal scope of practice and jurisdictional requirements.


Related Courses
1
https://www.audiologyonline.com/audiology-ceus/course/20q-pediatric-amplification-audibility-36815
20Q: Developments in Pediatric Amplification – Audibility, Mild Hearing Loss and More
This course will cover aided audibility in children with hearing aids. A review of key factors such as degree of hearing loss, real-ear verification measures, prescriptive targets, and full-time use of the aid will be discussed.
textual, visual
129
USD
Subscription
Unlimited COURSE Access for $129/year
OnlineOnly
AudiologyOnline
www.audiologyonline.com
20Q: Developments in Pediatric Amplification – Audibility, Mild Hearing Loss and More
This course will cover aided audibility in children with hearing aids. A review of key factors such as degree of hearing loss, real-ear verification measures, prescriptive targets, and full-time use of the aid will be discussed.
36815
Online
PT90M
20Q: Developments in Pediatric Amplification – Audibility, Mild Hearing Loss and More
Presented by Ryan McCreery, PhD
Course: #36815Level: Intermediate1.5 Hours
AAA/0.15 Intermediate; ACAud inc HAASA/1.5; AG Bell - LSLS/1.5 Domain 1, Domain 2; AHIP/1.5; ASHA/0.15 Intermediate, Professional; BAA/1.5; CAA/1.5; Calif. SLPAB/1.5; IACET/0.2; IHS/1.5; Kansas, LTS-S0035/1.5; NZAS/2.0; SAC/1.5
This course will cover aided audibility in children with hearing aids. A review of key factors such as degree of hearing loss, real-ear verification measures, prescriptive targets, and full-time use of the aid will be discussed.
2
https://www.audiologyonline.com/audiology-ceus/course/ethics-in-audiology-presented-partnership-35880
Ethics in Audiology, presented in partnership with Salus University
In this two-part series, a review of unique ethical challenges that can arise will be covered to provide audiologists with a framework for evaluating and resolving ethical quandaries that may occur in pediatric audiology. Discussion of specific elements that will ensure that humanitarian outreach programs reach sustainability and success will be reviewed.
auditory, textual, visual
129
USD
Subscription
Unlimited COURSE Access for $129/year
OnlineOnly
AudiologyOnline
www.audiologyonline.com
Ethics in Audiology, presented in partnership with Salus University
In this two-part series, a review of unique ethical challenges that can arise will be covered to provide audiologists with a framework for evaluating and resolving ethical quandaries that may occur in pediatric audiology. Discussion of specific elements that will ensure that humanitarian outreach programs reach sustainability and success will be reviewed.
35880
Online
PT180M
Ethics in Audiology, presented in partnership with Salus University
Presented by Ryan McCreery, PhD, Jackie Clark, PhD
Course: #35880Level: Intermediate3 Hours
AAA/0.3 Intermediate; ACAud inc HAASA/3.0; BAA/3.0; CAA/3.0; Calif. SLPAB/3.0; IACET/0.3; IHS/3.0; Kansas, LTS-S0035/3.0; NZAS/3.0; SAC/3.0; Tier 1 (ABA Certificants)/0.3
In this two-part series, a review of unique ethical challenges that can arise will be covered to provide audiologists with a framework for evaluating and resolving ethical quandaries that may occur in pediatric audiology. Discussion of specific elements that will ensure that humanitarian outreach programs reach sustainability and success will be reviewed.
3
https://www.audiologyonline.com/audiology-ceus/course/salus-series-practicing-pediatric-ethics-35636
Approaches for Resolving Ethical Dilemmas in Pediatric Audiology, presented in partnership with Salus University
Providing audiological care for children with hearing loss and their families is rewarding, but unique ethical challenges can arise. The goal of this presentation is to provide audiologists with a framework for evaluating and resolving ethical quandaries that may occur in pediatric audiology.
auditory, textual, visual
129
USD
Subscription
Unlimited COURSE Access for $129/year
OnlineOnly
AudiologyOnline
www.audiologyonline.com
Approaches for Resolving Ethical Dilemmas in Pediatric Audiology, presented in partnership with Salus University
Providing audiological care for children with hearing loss and their families is rewarding, but unique ethical challenges can arise. The goal of this presentation is to provide audiologists with a framework for evaluating and resolving ethical quandaries that may occur in pediatric audiology.
35636
Online
PT90M
Approaches for Resolving Ethical Dilemmas in Pediatric Audiology, presented in partnership with Salus University
Presented by Ryan McCreery, PhD
Course: #35636Level: Intermediate1.5 Hours
AAA/0.15 Intermediate; ACAud inc HAASA/1.5; AG Bell - LSLS/1.5 Domain 5; BAA/1.5; CAA/1.5; Calif. SLPAB/1.5; IACET/0.2; IHS/1.5; Kansas, LTS-S0035/1.5; NZAS/2.0; SAC/1.5
Providing audiological care for children with hearing loss and their families is rewarding, but unique ethical challenges can arise. The goal of this presentation is to provide audiologists with a framework for evaluating and resolving ethical quandaries that may occur in pediatric audiology.
4
https://www.audiologyonline.com/audiology-ceus/course/eaudiology-dissecting-evidence-based-practice-40124
eAudiology: Dissecting the "Evidence" in Evidence-Based Practice
Bridging the gap between clinical research and clinical practice can be a difficult task for many practicing clinicians. This course aids clinicians in translating clinical research to everyday practice. Interactive case studies and article critiques are utilized throughout the session to allow participants to develop and improve their understanding of clinical research and its implementation in every practice.
auditory, textual, visual
129
USD
Subscription
Unlimited COURSE Access for $129/year
OnlineOnly
AudiologyOnline
www.audiologyonline.com
eAudiology: Dissecting the "Evidence" in Evidence-Based Practice
Bridging the gap between clinical research and clinical practice can be a difficult task for many practicing clinicians. This course aids clinicians in translating clinical research to everyday practice. Interactive case studies and article critiques are utilized throughout the session to allow participants to develop and improve their understanding of clinical research and its implementation in every practice.
40124
Online
PT30M
eAudiology: Dissecting the "Evidence" in Evidence-Based Practice
Presented by Aaron Roman, AuD, Ryan McCreery, PhD
Course: #40124Level: Introductory0.5 Hours
AAA/0.05 Introductory
Bridging the gap between clinical research and clinical practice can be a difficult task for many practicing clinicians. This course aids clinicians in translating clinical research to everyday practice. Interactive case studies and article critiques are utilized throughout the session to allow participants to develop and improve their understanding of clinical research and its implementation in every practice.
5
https://www.audiologyonline.com/audiology-ceus/course/improving-ehdi-with-caeps-clinical-31492
Improving EHDI with CAEPs: Clinical Assessment of the Cortical Auditory Evoked Potential in Children with Hearing Loss
This course will provide an overview of cortical auditory evoked potentials, current research, benefits and limitations to using CAEPs in a busy clinic, and several case studies.
auditory, textual, visual
129
USD
Subscription
Unlimited COURSE Access for $129/year
OnlineOnly
AudiologyOnline
www.audiologyonline.com
Improving EHDI with CAEPs: Clinical Assessment of the Cortical Auditory Evoked Potential in Children with Hearing Loss
This course will provide an overview of cortical auditory evoked potentials, current research, benefits and limitations to using CAEPs in a busy clinic, and several case studies.
31492
Online
PT60M
Improving EHDI with CAEPs: Clinical Assessment of the Cortical Auditory Evoked Potential in Children with Hearing Loss
Presented by Elizabeth Musgrave, AuD, CCC-A
Course: #31492Level: Intermediate1 Hour
AAA/0.1 Intermediate; ACAud inc HAASA/1.0; BAA/1.0; CAA/1.0; Calif. SLPAB/1.0; IACET/0.1; IHS/1.0; Kansas, LTS-S0035/1.0; NZAS/1.0; SAC/1.0
This course will provide an overview of cortical auditory evoked potentials, current research, benefits and limitations to using CAEPs in a busy clinic, and several case studies.