
Learning Outcomes
After completing this course, readers will be able to:
- Identify different key features of hearing aid processing that contribute to sound quality.
- Differentiate between sound quality and audibility/speech understanding as contributing factors to initial and long term acceptance.
- Identify speech recognition improvement that can be obtained with the Signia Nx platform.
Introduction
Most of you reading this have normal hearing. And, in your daily life you rarely, if ever, think about “sound quality.” True, if you are serious about your home music listening, sound quality might be something that you indeed think about on occasion—the right delivery system, loudspeakers, headphones and streaming devices. This, however, tends to be more of a recreational concern, not something that impacts your daily activities.
But, what about individuals with hearing loss? For them, inputs of all types, and from all sources, lack optimal sound quality. With acquired hearing loss, the change usually is gradual, but eventually, the person realizes that things simply do not sound as good as they used to. When these individuals are fitted with hearing aids, sound quality is brought to the forefront, as the audibility of most sounds has been altered, and some sounds that may have been forgotten are now audible. The goal, therefore, is that hearing-aid processed signals sound “natural” to the user. If not, hearing aid use may be reduced, or in some cases, the hearing aids are rejected. With this in mind, it is not surprising that when surveys reveal the top ten factors that contribute to “overall hearing aid satisfaction,” five of the top ten factors relate to sound quality: clarity of sound, naturalness, and richness/fidelity, loud sound comfort and sound of own voice (Kochkin, 2010).
Sound quality is also linked to emotion. Different sounds evoke a very quick, distinct and wide range of emotions, ranging from sad to happy, excited to calming. Emotional valence describes the intrinsic attractiveness ("goodness”; positive valence) or averseness ("badness”; negative valence) of a sound. Recent research at Vanderbilt University compared the emotional valence for older adults with normal hearing to an age-matched group of older adults with bilateral, symmetrical, mild to moderate-severe sensorineural hearing loss (Picou, 2016). The authors report that as the degree of hearing loss increases, the range of emotional responses diminishes. Ratings of valence were reduced in response to pleasant sounds and were elevated in response to unpleasant sounds. That is, ratings of all sounds were closer to “neutral” than the ratings of listeners with better hearing. The authors state that these data suggest that listeners with sensorineural hearing loss are less emotionally affected by sounds than their peers with normal hearing, and may not be fully benefiting from activities that their peers with normal hearing find pleasurable. This is yet another reason why the sound quality of hearing aids must be high fidelity, so as to not exacerbate this potentially negative consequence of hearing loss.
Sound Quality and Speech Intelligibility: A Necessary Compromise?
To this point, we have discussed the importance of sound quality in hearing aid design and processing. But, what drives most individuals to seek out amplification is their desire to improve their understanding of speech, particularly speech in background noise. This also must then be heavily weighted when new processing algorithms are designed – also, of course, to ensure a true benefit when the hearing aids are later worn in daily life. In this regard, over the past few years, the Signia hearing aids have been shown, through independent research, to improve speech understanding to the point that in background noise, hearing-impaired listeners out-perform their age-matched peers with normal hearing (Froehlich, Freels, & Powers, 2015). Additionally, research at the University of Western Ontario revealed that this bilateral beamforming technology provided more than 50% improvement in speech recognition, when compared to omnidirectional (Littmann & Hoydal, 2017). Moreover, through the use of Signia narrow directionality, listening effort is significantly reduced, which was documented based on both subjective ratings and objective EEG analysis in multi-site tesing (Littmann, Wu, Froehlich, & Powers, 2017).
The speech recognition findings mentioned above were obtained with the Signia primax platform. To ensure that the bilateral beamforming of the Signia Nx was equal to, or superior to the previous generation, comparative testing between the products was conducted, using both a vented and open fitting arrangement. The results of this are shown in Figure 1.
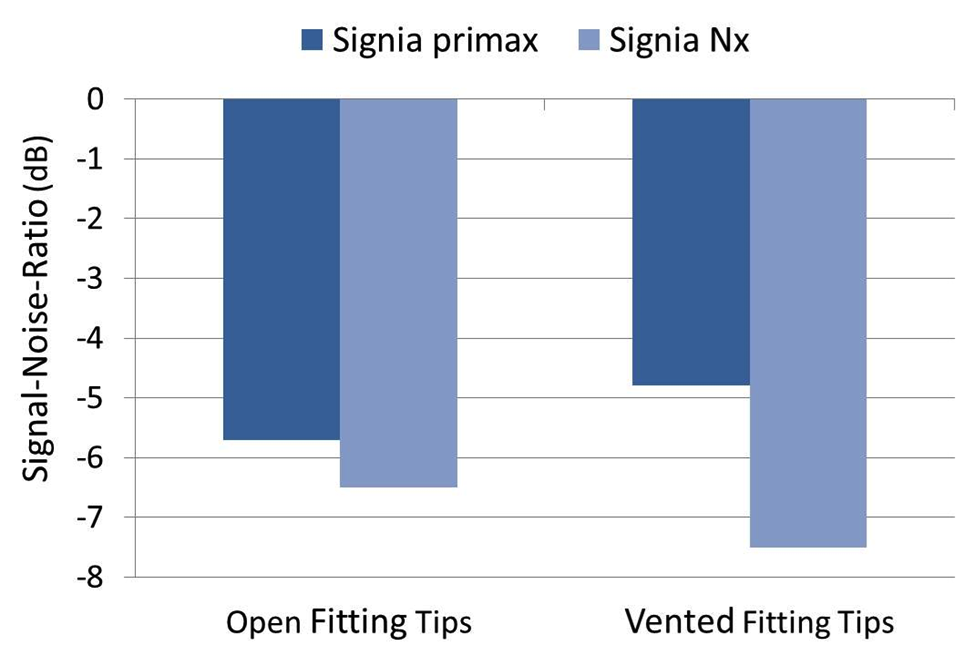
Figure 1. Mean findings for the German Matrix Test (in signal-to-noise ratio [SNR] SRT-80), comparing the binaural beamforming of the Signia primax to the Signia Nx. Testing conducted for both open and vented fitting domes.
Testing was conducted using the German Matrix Test (Oldenburg Sentence Test), and the mean findings shown are expressed in signal-to-noise ratio (SNR) (established using an SRT-80 test procedure). Observe that for open fittings, the improvement with the Nx was about 1 dB as compared to the primax, and with a vented fitting, the improvement was over 2 dB. This SNR improvement can have a significant impact on speech understanding for many listening-in-noise situations—the slope of the psychometric function of the German Matrix test is 17.1%/dB.
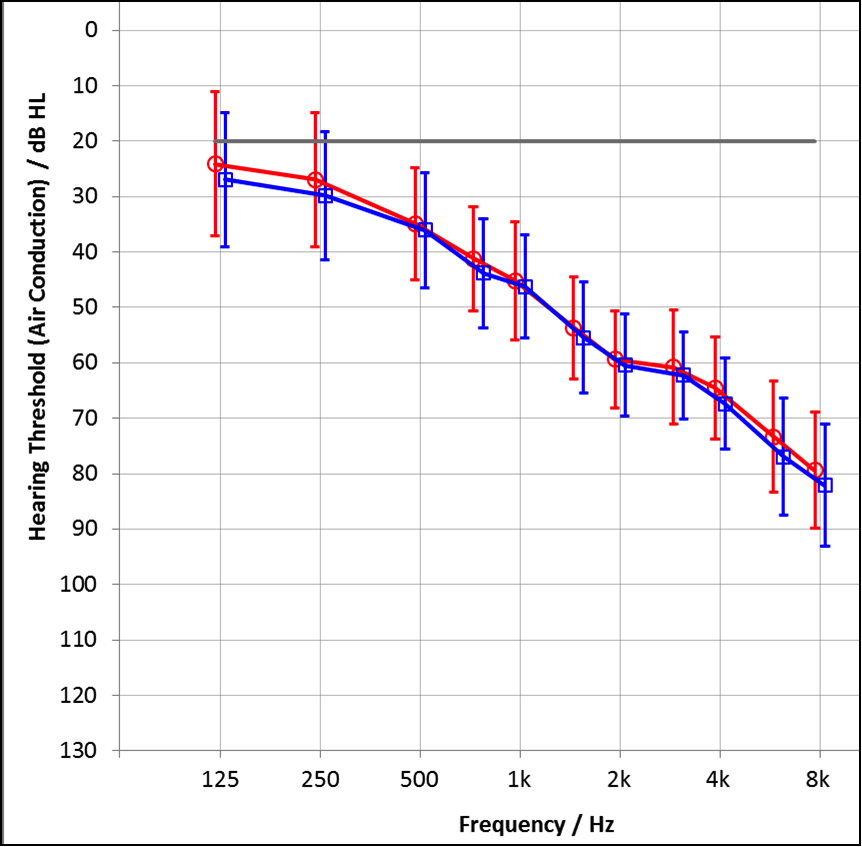
Figure 2. Mean audiogram of the right and left ears of the participants (red=right; blue=left).
While the findings of these research studies are impressive, the obvious question then becomes: “Can sound quality be maintained while at the same time implementing processing that maximizes speech understanding?” With the new Signia Nx, we believe the answer is a resounding “yes.”
User First Acceptance
One of the most important times during the overall hearing aid fitting process is when new users first try their hearing aids. The goal is to make the amplified speech and environmental sounds as natural as possible. If this is not accomplished, the user may decide very quickly that using hearing aids is not a good idea. To examine the first acceptance of the Signia Nx, a study was conducted at the Hörzentrum in Oldenburg, Germany. Individuals with downward sloping hearing losses were fitted bilaterally with the instruments, programmed to the proprietary fitting formula NxFit (see Figure 2 for mean audiogram). Immediately after being fitted, the participants rated their satisfaction for speech perception (both in quiet and in noise) and also rated the dynamics of music and environmental noises. Ratings were obtained on a 4-point satisfaction scale (1=very dissatisfied; 4=very satisfied).
The results of the acceptance study are shown in Figure 3. Observe that for both the perception of speech, and the dynamics, all ratings were near the top of the rating scale, with overall ratings of 3.5 or better. Even the difficult “speech-in-noise” condition was rated “satisfactory.”
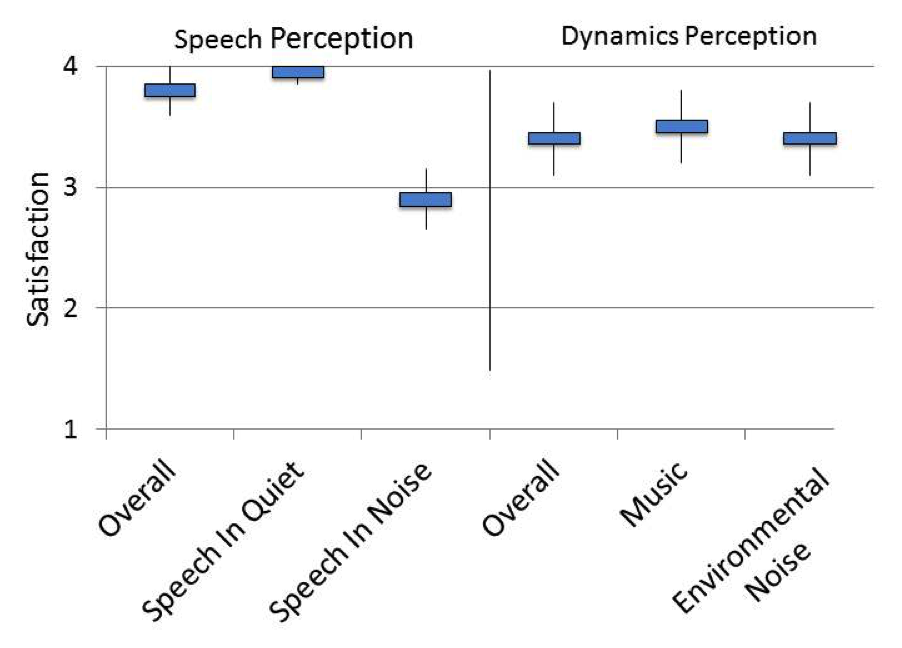
Figure 3. Mean satisfaction rating obtained on a 4-point scale for the Signia Nx, obtained immediately after the first fitting (Nx-Fitting). Judgments obtained for both the perception of speech and for dynamics of music and environmental sounds.
A critical aspect of sound quality in general, and weighted heavily regarding the first acceptance of hearing aids, is the user’s impression of his or her own voice. Does the user perceive his or her own voice as hollow, tinny, sharp, or harsh? If the user’s voice is not acceptable, this alone can prevent routine hearing use, and even lead to hearing aid rejection. In the past, treatment of this issue has been fraught with negative consequences (e.g., simply turning down gain reduces speech understanding). To directly address this problem, the Signia Nx has introduced a new feature, Own Voice Processing (OVP). Using this innovative algorithm, the hearing aid can detect the user’s voice, and then instantaneously alter the gain and output to individualized programmed values. This has no impact on the gain and output of the voices of others. Research studies have shown this feature to be highly successful—see Hoydal (2017) for a complete review.
Regarding the acceptance study mentioned earlier, following the initial fitting and quality judgments, the participants used the Signia Nx hearing aids for several weeks in a home field trial. Following their everyday experiences, they rated sound quality using an abbreviated Speech, Spatial Qualities of Hearing Scale (SSQ; Gatehouse and Noble, 2004). Representative questions from the SSQ used in these ratings were 1, 2, 4, 13, 16, and 18. The rating scale was the standard 11 point, 0-10 scale of the SSQ (0=”Not at all”; 10=“Perfectly”). The mean quality ratings obtained are shown in Figure 4. Also shown are the clinical norms (unaided) reported by Gatehouse and Noble (Gatehouse & Noble, 2004).
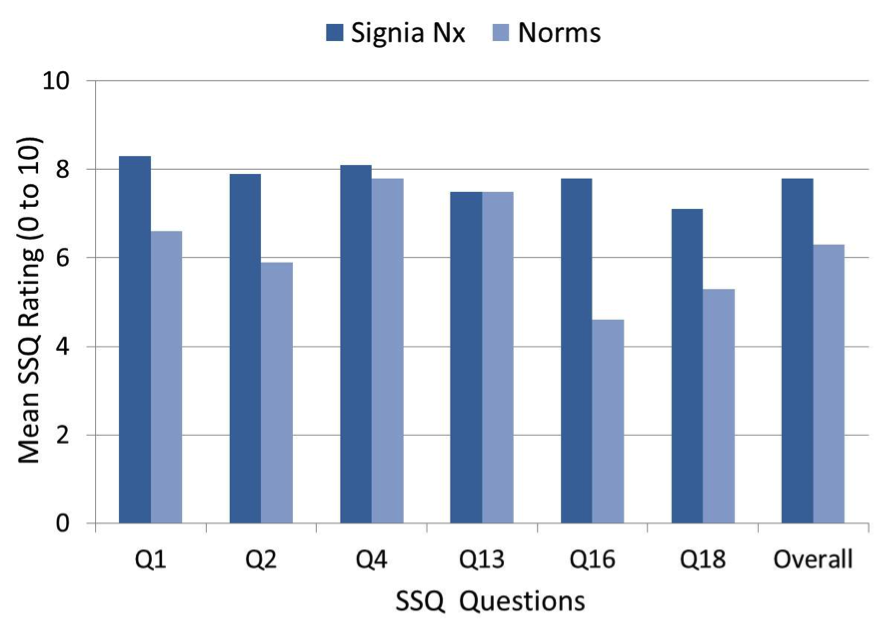
Figure 4. Mean quality ratings for questions from the SSQ, obtained following home trial of Signia Nx. Also included are the normative data for the selected questions from Gatehouse & Noble (2004).
As shown, the SSQ ratings were very positive for sound quality, and in fact, only slightly lower than the norms reported for individuals with normal hearing (Demeester et. al., 2012). For most items, scores were significantly higher than the Gatehouse and Noble norms for individuals with hearing loss. The most notable advantage was for Q16, which relates to listening to others in a car while driving. The one question where the findings were the same as the norms (Q13), concerned judging the mood of someone based on the sound of their voice—not an unexpected findings as this is something that is difficult to do consistently even for individuals with normal hearing.
Localization and Sound Quality
We are able to localize sound primarily because we have two ears that sample signals in two different places, connected to a sophisticated binaural processing system, i.e. the brain. This is made possible through interaural level difference cues, interaural time differences, and monaural filtering effects. Localization of sound is important for safety, and assists in providing a general awareness of our surroundings—knowing where a sound is coming from may help us to identify the sound.
Localization also is an important aspect of sound quality. As reviewed by Byrne and Noble (1998), auditory sensations are essential to aesthetic experience, and auditory localization is a big part of that. For example, the quality of the sound of a bird singing increases if we can identify the general area where the bird is sitting. Also related to localization are the externalization of sounds and the natural feeling of spatial orientation. Again, without this additional quality of the sound, we might feel “out of touch” with the environment, even though the sounds have been made audible.
As mentioned earlier, a very successful method to address the “speech in noise” issue is to utilize binaural beamforming. Although it is inevitable that this processing will disrupt localization to some degree, care is taken to keep this disruption to a minimum, and to maintain localization cues particularly for off-center sounds. To examine the enhanced Nx platform, a laboratory localization study was completed that compared this technology to its predecessor, the Signia primax. Testing was conducted for individuals (n=19) with bilateral symmetrical sensorineural downward-sloping hearing loss (~35-40 dB hearing loss in the low frequencies; ~70-75 dB hearing loss in the high frequencies); binaural beamforming was “Fixed On.” Localization also was assessed for Signia Nx omnidirectional (TruEar) processing.
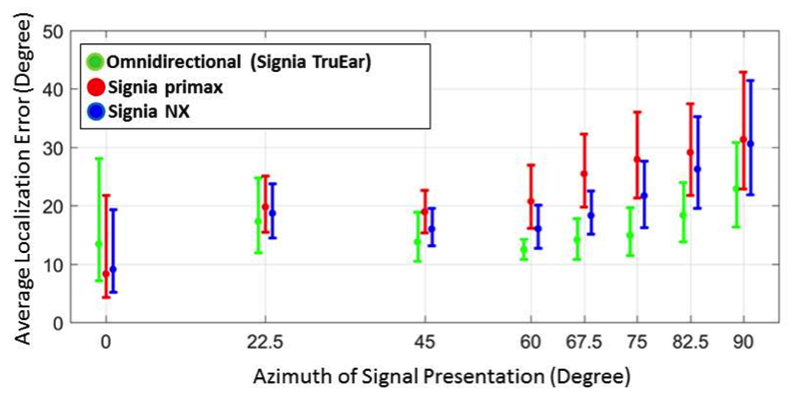
Figure 5. Localization study comparing Signia Nx and Signia primax. Display of average localization error (degree) as a function of the azimuth of the signal presentation. Results shown for Signia primax and Nx with beamforming fixed “on,” and for Nx omnidirectional (TruEar).
The results of this localization testing are shown in Figure 5. As expected, the best results were obtained for the TruEar condition. However, the findings with the new Nx processing revealed that the Nx enhancements were successful, as only slightly poorer localization than TruEar processing was observed, and, an improvement from the previous generation Signia primax was present.
To a large extent, the concern over localization when narrow directionality is activated is a non-issue, for at least three different reasons. First, this feature will only be activated when noise levels are high and there is an adverse signal-to-noise ratio. Secondly, as shown in Figure 5, until the source of interest is greater than +/- 60 degrees, localization with binaural beamforming active is essentially the same as omnidirectional (TruEar). Even in group settings, the talker of interest is nearly always within the +/- 60 degree window. Finally, even when the feature is activated, when visual cues are present, localization is not significantly reduced (Picou et. al., 2014). We assume that most hearing aid users will use visual cues when engaged in group conversations.
Sound Quality for High Inputs
An area that is often overlooked is the sound quality for high inputs. In the fitting and programming of hearing aids, we usually think of the automatic gain control of output (AGCo) as the circuit that determines the maximum power output (MPO)—we program AGCo kneepoints so that loud sounds do not exceed the patient’s loudness discomfort levels (LDLs). We sometimes forget that there also is an input limiter. With early digital hearing aids, this limit was as low as 90 dB SPL or so, and even today this limiting might occur in the mid-90s with some models. Hearing aid users commonly encounter inputs of 100 dB SPL or higher at such places as loud restaurants and sporting events, and listening to music—if the input SPL exceeds the limiter, distortions are likely. There is an advantage, therefore, of having a higher level for the input limiter (the MPO setting will still ensure the signal does not exceed the patient’s LDL).
The input limiter for the Signia Nx is 113 dB SPL. A potential downside of a higher input limiter is increased floor/circuit noise, which can be annoying. For this reason, with Nx, the limiter is adaptively adjusted based on the input signal. That is, the limiter only reaches the higher values when loud sounds are of that same value. If the input is that high, the noise floor of the instrument is no longer an issue. Additionally, this automatic adaptive feature is available in all programs, including the “Universal” program for convenience for the users, as they do not have to switch to a different dedicated program, and no special programming is required by the hearing care provider.
Sound Quality for Streamed Signals
To this point we have talked about sound quality using conventional amplification. The Signia Nx employs direct streaming using 2.4 GHz technology, and therefore, it’s also important to consider sound quality for streamed signals. While it is tempting to assume that a hearing aid that has excellent sound quality in general will also have excellent sound quality for a streamed signal, this is not necessarily true. The processing and algorithms required for incorporating a direct streamed signal involve compromises in the encoding and the subsequent signal processing, which can result in negatively altering the sound quality. This potentially can result in distortions, smearing, artifacts, narrowed-bandwidth, and/or a signal lacking in clarity or richness.
To examine Signia streamed signal quality, research was conducted using eight listeners with normal hearing who were experts at audio quality, and making judgments of audio signals. Comparative judgments were also conducted for the premier hearing aid (mini-BTE RICs) from four other leading manufacturers. The hearing aids were all programmed for a flat 40 dB hearing loss, for an experienced listener, using each manufacturer’s proprietary fitting. Double domes/power domes were used for the fitting. Details of the design can be found at Froehlich, Junius and Branda (2017). The ratings by the expert listeners were conducted blinded using a randomized approach. As a reference, the participants listened to the original sound file, without hearing aid processing or streaming.
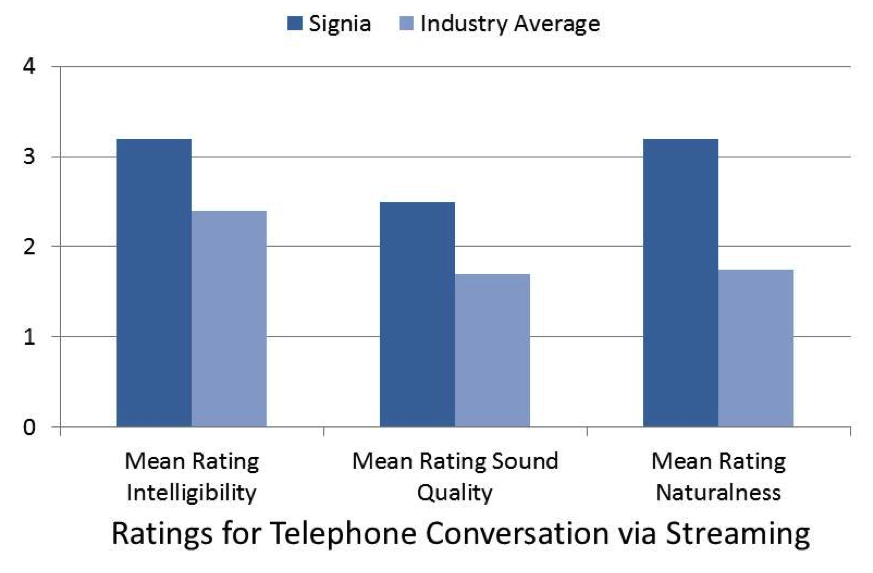
Figure 6. Mean ratings for Signia compared to the mean average of four competitive products. Speech intelligibility ratings for telephone streamed speech were conducted using a 6-point scale—0=Not Good to 5=Very Good. The sound quality ratings of telephone speech were conducted using a 5-point scale—0=Bad to 4=Excellent. The naturalness ratings were obtained using a 6-point scale—0=Not Natural to 5=Very Natural.
Figure 6 shows the mean ratings for intelligibility, overall sound quality and naturalness for the streamed signal of speech via the mobile phone. While the results are plotted on a 5-point scale, the intelligibility and naturalness ratings were obtained on a 6-point scale, so only relative, not absolute differences are meaningful. For all three measures, ratings were significantly higher for the Signia product—for both intelligibility and sound quality the mean for the Signia was nearly 1 point higher than the Industry Average (fair/good versus poor/fair). The biggest advantage for Signia was observed in the “naturalness” domain, where the rating was 3.2 vs. only 1.7 for the Industry Average.
For many patients, steaming music is the most popular benefit of the 2.4 GHz technology. Given the diversity of music itself, and individual preferences for different types of music, we selected five different sample genres for the ratings: classical, instrumental, jazz, piano, and pop. Shown in Figure 7 are the mean ratings from the experts for the five different music samples for Signia and the Industry Average. The average values for the Signia product were substantially above the Industry Average. In general, these mean ratings were at or above “Fair” (#3 Rating). By comparison, the Industry Average was only somewhat above “Poor” (#2 Rating). Interestingly, the superiority of Signia appears to be the greatest for listening to piano music, which could be related to a more artifact-free signal, one of the other findings of the research (see Froehlich, Junius & Branda, 2017).
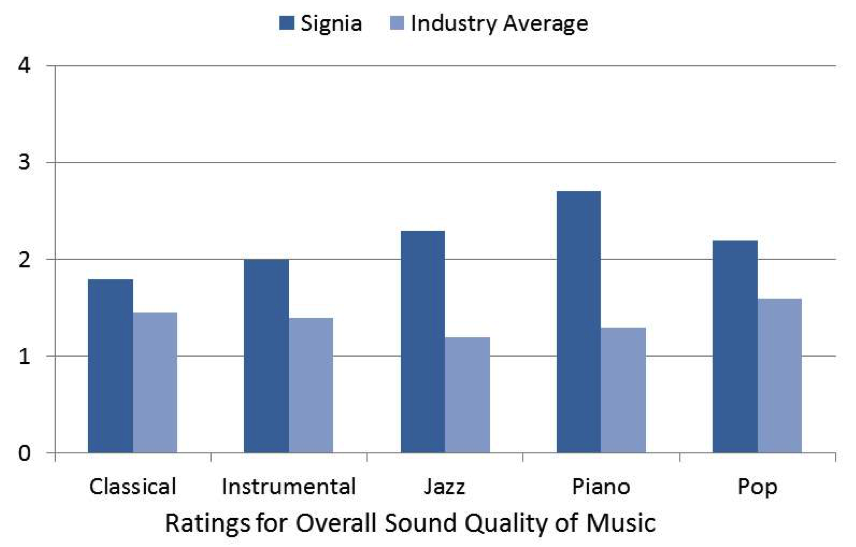
Figure 7. Mean ratings for Signia compared to the mean average of four competitive products for five different genres of music. Ratings conducted using a 5-point scale—0=Bad to 4=Excellent.
Summary
Sound quality is an important and sometimes overlooked aspect of the overall hearing aid fitting process. It might be speech intelligibility issues that initially motivate potential hearing aids users to take action, and guarantee continued benefit in daily life, but it is sound quality that ensures they become regular users of amplification. Certainly the patient’s first impression is one of the most important sound quality areas, but we also are concerned with everyday experiences after the fitting, localization, the quality of high inputs, and streamed signals. In this paper we have reviewed research with the Signia Nx, showing that high marks for this product were obtained for all of these sound quality areas.
References
Byrne, D., & Noble, W. (1998). Optimizing sound localization with hearing aids. Trends Amplif., 3(2), 51-73.
Demeester, K., Topsakal, V., Hendrick, J., Fransen, E., van Laer, L., Van Camp, G.,...van Wieringen, A. (2012). Hearing disability measured by the speech, spatial and qualities of hearing scale in clinically normal-hearing and Hearing impaired middle-aged persons. Ear Hear., 33(5), 615-626.
Froehlich, M., Freels, K., & Powers, T. (2015, May) Speech recognition benefit obtained from binaural beamforming hearing aids: comparison to omnidirectional and individuals with normal hearing. AudiologyOnline, Article 14338. Retrieved from www.audiologyonline.com
Froehlich, M., Junius, D., & Branda, E. (2017). A comparison of signal quality of direct streaming hearing aids. Canadian Audiologist, 4(4). Retrieved from https://www.canadianaudiologist.ca/issue/volume-4-issue-4-2017
Gatehouse, S., & Noble, W. (2004). The speech, spatial, and qualities of hearing scale (SSQ). Int J Audiol., 43(2), 85-99.
Hoydal, E.H. (2017). Communication – the primary goal of audiologic rehabilitation. Hearing Review, 24(11).
Kochkin, S. (2010). MarkeTrak VIII: Consumer satisfaction with hearing aids is slowly increasing. Hearing Journal, 63(1),19-32.
Littmann, V., & Hoydal, E.H. (2017). Comparison study of speech recognition using binaural beamforming narrow directionality. Hearing Review, 24(5), 34-37.
Littmann, V., Wu, Y.H., Froehlich, M., & Powers, T.A. (2017). Multi-center evidence of reduced listening effort using new hearing aid technology. Hearing Review, 24(2), 32-34.
Picou, E.M. (2016). How hearing loss and age affect emotional responses to non-speech sounds. J Speech Lang Hear Res., 59(5),1233-1246.
Picou, E.M., Aspell, E., & Ricketts, T.A. (2014). Potential benefits and limitations of three types of directional processing in hearing aids. Ear Hear., 35(3), 339-352.
Citation
Froehlich, M., & Powers, T.A. (2017, November). Sound quality as the key to user acceptance. AudiologyOnline, Article 21621. Retrieved from www.audiologyonline.com


