
This study examines the performance of 15 school-aged children with profound hearing loss following an upgrade to an advanced multiple channel non-linear hearing instrument. Significant improvements were found in terms of audibility, speech understanding in quiet and noise as well as in listening preference. This study builds on the increasing evidence that children with profound hearing loss should be given the opportunity to try the latest advanced superpower hearing instruments designed to provide the best possible auditory outcome.
Introduction
In recent years, the benefit of multiple channel non-linear compression for people with severe hearing loss has been demonstrated . However, past attempts to provide non-linear solutions to people with profound hearing loss have met with limited success . One factor accounting for these findings may have been the assumption that all people with profound loss behaved the same way. The lack of a generalized benefit across patients with profound hearing loss may have masked the fact that many of these same individuals may achieve positive results with non-linear amplification. When non-linear solutions are applied to people with profound hearing loss, no single fitting rationale will provide optimum outcome to this population.
Specific Gain and Compression Requirements for Profound Hearing Loss
DigiFocus II SuperPower is based on the Adaptive Speech Alignment (ASA) fitting rationale - a multiple channel, non-linear approach to amplification for people with sensorineural hearing loss. The amount of gain, compression and compression type is chosen to present as much speech information to the individual as possible. Generally, for severe and profound hearing loss, available gain must be increased in relation to the amount of hearing loss but the amount of compression needs to be controlled. We must balance the desire to place the amplified speech within the remaining dynamic range, with the need to provide sufficient temporal cues in the ear with degraded resolution ability . Additionally, due to cochlear dead zones we may not wish to provide amplification across the full frequency range, but restrict amplification to the low or mid frequencies .
Sound Perception Management
Typical multiple-channel, non-linear processing circuits are designed to make most, if not all, of the dynamic range available to the person with hearing loss. As hearing loss increases into the severe and profound ranges, this core assumption requires modification.
The assumption common to fitting lesser hearing losses is that the benefits of providing the full speech range within the remaining dynamic range outweighs any loss of information from compression of the signal. However, given the dramatic cochlear damage in profound sensorineural hearing loss, this assumption may not be true.
The damage pattern in some profound sensorineural hearing loss ears may require a signal that is more linear (Type 1), whereas others may be able to make full use of a compressed signal, in keeping with the ASA approach (Type 2). Ears that are sensitive to too much compression (Type 1) are likely to have extensive damage throughout the inner ear and a minimal amount of remaining, intact inner hair cells. Signal resolution beyond the ability to detect pure-tones is very poor in these cases. These listeners may only make use of the peaks of the speech signal. Conversely, there are other people with profound sensorineural hearing loss who can use signals even more compressed than that which is typically called for by ASA principles (Type 3). These ears probably have extensive outer hair cell loss and some amount of inner hair cell loss (accounting for the profound thresholds), but sufficient residual signal resolution capacity to extract information from a compressed signal.
The variation from patient to patient results in the fact that a generalized fitting approach is unlikely to be appropriate for all patients. The difference in processing abilities are sufficiently different across Types 1, 2 and 3 patients, that simply fine tuning a standard nonlinear fitting will not provide optimum outcomes. Rather, the basic manner in which the hearing instrument processes sound should be matched to the way the patient's ear processes sound.
Children with profound hearing loss
Children with profound hearing loss present unique audiologic challenges. An immature auditory system and the need to learn speech and language drive the importance of providing the best possible amplification. A previous study by Davis and Pogash showed the benefit provided by non-linear amplification for children with severe hearing impairment. 48 children from six countries participated in the Davis and Pogash (2002) study. Results showed a highly significant benefit with non-linear amplification over traditional technology for children with severe hearing loss.
The question of the current study is whether the provision of advanced digital nonlinear hearing aids provide similar benefits for children with profound sensorineural hearing impairment.
Study Method
The study's experimental design was to compare DigiFocus II SuperPower (DFII SP) to the typical technologies currently fitted to children with profound hearing loss. The study consisted of a series of test sessions. Initially, a complete audiologic evaluation was conducted to confirm degree and type of hearing loss. All current hearing aid fittings were evaluated for appropriate fit and function according to the strict test criteria (see below). Once this was completed, aided thresholds were obtained. Speech understanding in quiet and noise was obtained using word recognition tests. In addition, questionnaires about the current hearing aids were completed by the parents or the audiologist .
Following evaluation of the child's current amplification system, the child was fitted with DFII SP using the ASA2sp fitting algorithm. A follow-up appointment was made if any fine tuning adjustments were necessary. After wearing the DFII SP instruments for at least two weeks, speech understanding with the DFII SP instruments was completed in quiet and noise. The last visit was scheduled for eight weeks post fitting. Additional speech testing and questionnaires for the DFII SP fitting were obtained from the child and parents.
Previous Hearing Aid Fittings and Test Criteria
Five children from each of three different hearing centres took part in the study. All children had a pure-tone average (500, 1000 & 2000Hz) worse than 80dB HL with an air/bone gaps of 15dB or less (Figure 1). The children ranged in age from 7 to 16 years old, with an average age of 11 years and 7 months. Current amplification consisted of analogue peak clipping (N=8), analogue AGC (N=6) and digital (N=1).
To be consistent with the design of a 'well-fitted upgrade' style of study, the child's previous aids had to reflect the current acceptable local clinical practice. Minimum standards for appropriate previous fitting were taken from the guidelines developed by Davis and Pogash (2002) and included:
- Devices were fitted within past four years.
- Used on a daily basis for at least 20 hours per week.
- Free from acoustic feedback during normal use.
- Child reports that loud sounds were tolerable.
- Child reports that devices were physically comfortable to wear
- Provides estimates of aided gain of at least 1/3 hearing loss at 500, 1000, & 2000 Hz.
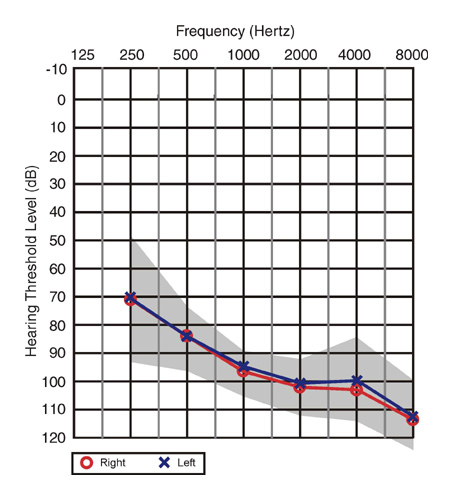
Figure 1. Average hearing threshold levels and one standard deviation for left and right ears.
Results and Discussion
Audibility
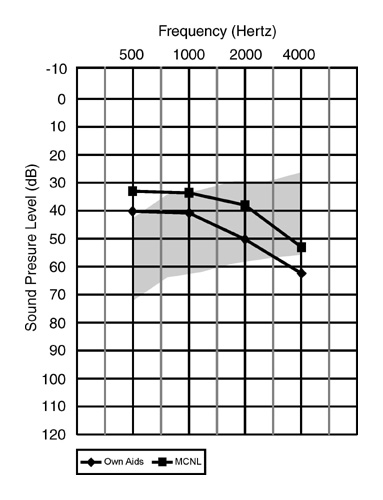
Figure 2. Mean aided thresholds of own aids and the multiple channel non-linear (MCNL) DigiFocus II SuperPower (DFII SP) superimposed on the long-term average speech spectrum.
Aided threshold assessment results found that on average, a substantial increase of audibility was possible with the DigiFocus II SP. This is consistent with previous studies (Davis & Pogash, 2002) and with the basic premise of non-linear amplification, that gain will be increased for softer inputs. While aided thresholds do not necessarily imply intelligibility, it is well established that making previously inaudible sounds audible can often increase speech understanding.
The mean results of aided threshold assessment of their own previous aids and the DigiFocus II SP test instruments are illustrated in Figure 2, where they are superimposed on an audiogram displaying the long term average speech spectrum. This data shows an increase in audibility of speech sounds across all frequencies and importantly for the high frequency sounds. This finding clearly indicates that multiple channel non-linear amplification can lead to improved audibility of speech sounds for children with severe hearing loss.
Speech Understanding
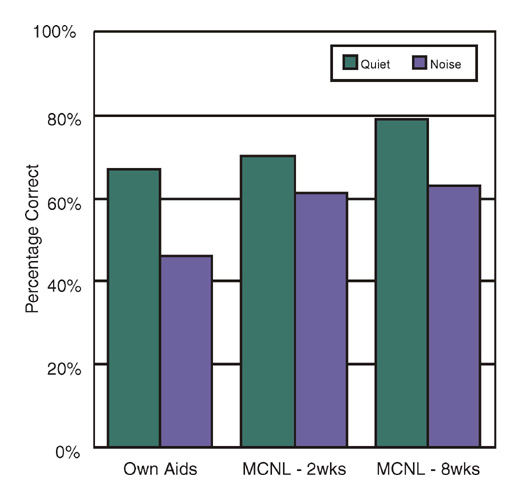
Figure 3. Average results across all the participants for open-set word understanding show the benefit for advanced multiple channel non-linear amplification (DFII SP) over the children's previous hearing aids.
To determine if the increase in audibility obtained through the Digifocus II Super Power did actually lead to an increase in speech understanding, pre-recorded speech intelligibility measures were used (Figure 3).
Results indicated that for speech understanding in quiet there was no discernable immediate difference. However, after a period of eight weeks, performance with the DFII SP increased to become statistically significant. Conversely, speech understanding in noise demonstrated an immediate significant difference in performance with no further improvement over time. Results demonstrate that children with profound hearing loss were able to take advantage of the benefits of DFII SP multiple-channel non-linear amplification.
Of importance is that improved results in quiet conditions were only observed over an extended period of time, whereas the improvement in listening in noise was apparent immediately. Therefore, if the audiologist wished to demonstrate immediate benefits of nonlinear amplification for children with profound hearing loss, testing in noise provided the best test situation.
In addition to statistically significant speech perception scores, verbal reports from the children, parents and teachers, addressing the benefits of the upgraded hearing aids (DFII SP) were impressive
Hearing Instrument Preferences
To further evaluate benefit, children and parents were asked to evaluate the DFII SP hearing aids in a series of listening situations and to make an overall preference evaluation.
The Listening Situations Questionnaire provides both an overall composite score (Figure 4) as well as scores for each listening situation. Both the children (t(15)=5.29, p<.0001 and parents p provided significantly higher composite scores for the dfii sp hearing aids over their previous aids.>
Evaluations of individual listening situations found statistically significant improvements were achieved in adverse listening situations. Interestingly, similar to the speech perception scores, the largest relative improvements were obtained for listening in background noise or at a distance. These situations occur commonly in a child's life such as during school or on the playground.
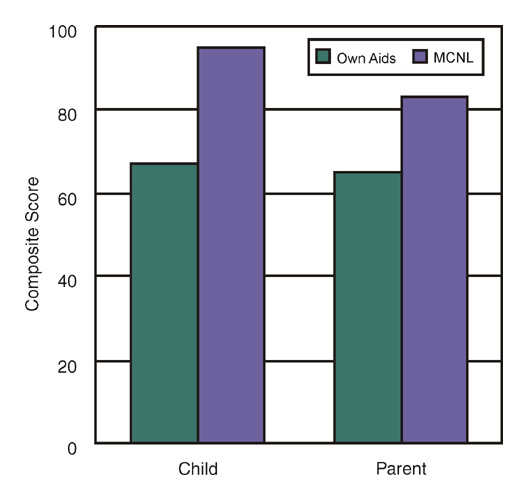
Figure 4. Improvement in composite Listening Situation Questionnaire scores from Previous Aids to DigiFocus II SuperPower (MCNL).
During the final visit, children and parents were asked to make an overall preference as to which hearing aid they would prefer to keep. Significantly, 14/15 children preferred the DFII SP and all 15/15 parents preferred the DFII SP.
Clinical Implications
This study demonstrated the benefit of fitting children with profound hearing loss with advanced nonlinear amplification.
In particular, benefits were seen in the children's ability to listen in adverse listening environments, such as background noise, or listening from a distance. This benefit was confirmed via speech recognition scores, which showed greater and more immediate improvement in noise than in quiet.
It is recommended that when upgrading children to more advanced hearing aids that performance in background noise should be included, as this is where benefit appears to be greatest.
Based on their performance with previous hearing instruments, three of the children in the study were candidates for cochlear implantation. Following their upgrade to more advanced hearing aids, those same children were no longer candidates for cochlear implantation, based on word recognition scores achieved with the DFII SP advanced nonlinear amplification.
Therefore, it is important that all children considering cochlear implantation are evaluated using the best amplification system possible to ensure that appropriate management decisions are made. This is even more important in situations where cochlear implant funding is limited.
When fitting severe and profound hearing loss flexibility is key.
In general, we can conclude that while people with severe to profound hearing loss appreciate more gain and less compression, there is a wide degree of diversity. The fitting rationale and the fitting platform must be able to distinguish between those who prefer a more linear approach and those who prefer more compression to obtain maximal results for each individual.
The present study showed the benefits of upgrading children with profound hearing loss to an advanced multiple channel non-linear platform. For children with residual hearing above 1000Hz, non-linear amplification provides many benefits in terms of increased access to low intensity speech sounds as well a the opportunity to place more speech information within the users restricted dynamic range.
It is imperative that children with residual hearing are provided with the opportunity to benefit from multiple channel non-linear processing.
Acknowledgements
The authors would like to gratefully acknowledge the audiologists of the following clinics for their assistance in the data collection Somerset Hearing Center (Hillsborough, NJ), Fairfax County Public Schools (Fairfax, VA) and Children's Memorial Hospital (Chicago, IL). Additionally, we would like to thank the fifteen children who participated in the study.
References
Bamford, J., McCracken, W., Peers, I., & Grayson, P. (1999). Trial of a two-channel hearing aid (low-frequency compression-high-frequency linear amplification) with school age children. Ear Hear, 20(4), 290-298.
Boothroyd, A., Springer, N., Smith, L., & Schulman, J. (1988). Amplitude compression and profound hearing loss. J Speech Hear Res, 31(3), 362-376.
Byrne, D., Parkinson, A., & Newall, P. (1990). Hearing aid gain and frequency response requirements for the severely/profoundly hearing impaired. Ear and Hearing, 11(1), 40-49.
Ching, T., Dillon, H., & Byrne, D. (1998). Speech recognition of hearing-impaired listeners: predictions from audibility and the limited role of high-frequency amplification. J Acoust Soc Am, 103, 1128-1140.
Davis, P. B., & Pogash, R. (2002). Power for kids. The Hearing Review, 9(3), 52-57.
Flynn, M. C., & Schmidtke, T. E. (2002). Four fitting issues for severe and profound hearing impairment. The Hearing Review, 9(11), 28-33.
Grimshaw, S. (1996). The extraction of listening situations which are relevant to young children, and the perception of normal-hearing subjects of the degree of difficulty experienced by the hearing impaired in different types of listening situations.: MRC Institute of Hearing Research.
Hogan, C., & Turner, C. (1998). High-frequency audibility: benefits for hearing-impaired listeners. Journal of the Acoustical Society of America, 104, 432-441.
Souza, P. E., & Bishop, R. D. (1999). Improving speech audibility with wide dynamic range compression in listeners with severe sensorineural loss. Ear Hear, 20(6), 461-470.
For further information about this study please contact Dr Mark Flynn at [email protected].
For more information on Oticon click here.
Click here to visit the Oticon website.
