
Donna Sorkin: I am Donna Sorkin from Cochlear America's HOPE Program. I am delighted to welcome a large group from around the globe to our session today. Today's topic is an important topic and I would like to share some information with you about it. A recent study that was published in Laryngoscope by Dr. Bob Peters and others in May of 2010 (Peters, Wyss, & Manrique, 2010) gave us some statistics about the numbers of bilateral surgeries around the globe. The authors surveyed a number of cochlear implant clinics around the world. They found that 70% of all bilateral cochlear implant surgeries have occurred in children. The largest group of those being children that are in the 3 to 10 year old grouping with 33% followed by adults, 30% followed by children under 3 years, and 26% followed by children 11 to 18 years. This interesting study looked at the demographics, candidacy and treatment approaches for bilaterals, but interestingly we still do not have much information out there about the therapy for bilateral recipients.
We are delighted to have MaryKay Therres with us today to focus on that particular topic. MaryKay Therres is a speech language pathologist and Auditory Verbal Therapist at the Children's Hospital at Philadelphia (CHOP). She is part of their cochlear implant team. Previously, she was at Children's Hospital Oakland also with their cochlear implant team. She is the co-author of AuSpLan which she has referenced before in other HOPE Online sessions for us, and she is also very involved in the professional preparation and cochlear implant program at CHOP. She is the co-developer and co-instructor in that program and has well over 15 years of experience with children who are deaf and hard of hearing. MaryKay is a regular HOPE Online speaker and we are really delighted to welcome her back for this important topic.
MaryKay Therres: Thanks, Donna and thank you, Cochlear Americas, for inviting me to give another presentation online. What I would like to do today before I jump into talking about therapy for children who have a bilateral cochlear implant is give a little bit of background information about why we would want to go ahead and consider bilateral implantation. Then I will get into what is the therapy that we want to do. I will be covering today some definitions or general terms that you may have heard with regard to bilateral cochlear implantation and some of the rationale as to why we might want to go ahead and do this implantation. Then I will discuss what the current research and implications are for candidacy (because as with unilateral cochlear implants not all children are going to have the same benefits), what we look at when we see a child to determine what benefit we think that child would get from the bilateral, and then I will get into the meat and potatoes of what the therapy would be for these children or individuals.
I would like to say thank you to two of my best friend audiologists, because some of the front part of this talk is more Audiology and I do not proclaim to be an audiologist at all. I am a speech language pathologist. I needed some help getting some of this information. Michael Jackson, who is the audiologist at the implant center here at CHOP, and Adeline McClatchie, who is a dear friend and mentor I worked with in the cochlear implant program out in California, were both helpful in putting some of this beginning information together.
Some of the terminology we might hear around bilateral cochlear implantation are "binaural hearing" and "bimodal devices". "Binaural hearing" is the coordination of sound in the central auditory pathway from hearing occurring in both ears, and that is really hearing in two normally-hearing ears. We might also hear the term "bimodal device", which means a cochlear implant in one ear which is electric signal and a hearing aid in the other ear which is an acoustic signal.
Bimodal Pros and Cons
What would be the pros and cons of having a cochlear implant in one ear and a hearing aid in the other, and being bimodal? One pro could be, depending upon the residual hearing, you may get great benefit from the other ear with the hearing aid, and get more of the natural acoustic sound versus the electric trick sound. You may have improved or enhanced music appreciation. You may keep that nerve stimulated which could minimize auditory deprivation. Some people will ask "should we keep the nerve stimulated and wait for nerve regeneration or research down the road?" I think, across the board, the answer to that is "no." That is not going to happen in the timely manner we would like to see it to preserve that ear for later technology or research. Those children are learning speech and language now and they need the best access to sound as it is now. Although it is important to keep the nerve stimulated, if that ear is not providing enough access to sound, we would probably be better off going to bilateral cochlear implantation rather than waiting for a nerve regeneration to come along. Another possible pro would be it providing some binaural hearing benefits.
What would the cons be? Often there is a lack of useable residual hearing. If there is more of a profound loss, even with amplification, they are not getting a lot of access to sound in that ear. That is a differing benefit between the ears as you may get a lot of access to sound with a cochlear implant and minimal access to sound with the hearing aid. You are managing more equipment. You have your cochlear implant equipment and your hearing aid equipment. That makes it a little more complicated. You can have feedback issues with the ear molds, and we need to look at what the benefit is versus the hassle. Is it worth considering trying to keep a hearing aid in the other ear or do we think that a cochlear implant might be the better option for that second ear?
Bilateral Cochlear implants
A bilateral cochlear implant refers to one cochlear implant in one ear (electric stimulation) and one cochlear implant in the other ear which is also electric stimulation. "Simultaneous bilateral cochlear implant" means you are receiving both implants in one surgery. "Sequential" is where you receive one cochlear implant in one surgery, and after a period of time, you then receive the other cochlear implant in a second surgery. These surgery options depend sometimes upon the preference of the surgeon or the cochlear implant team that you are on. Here at CHOP the surgeon preference is to do sequential. For various reasons we might do simultaneous, but in general, we are doing sequential which is the surgeon preference. This may vary from center to center.
Some other terminology that you might find when talking about the bilateral cochlear implant are "right ear" versus the "left ear", "old implant" versus "new implant", "old ear" versus "new ear", "first implant" versus "second implant", "first ear" versus "the second ear", "original implant" versus "bilateral implant", or as families may say "this is his big boy ear" versus "his baby ear". People come up with different terminology so you may hear different things. We do have children that get re-implanted, and so the water can get muddied when you are talking about the second implant. Are you talking about the new implant in the same ear or talking about a new implant in the bilateral ear? You can see how confusing it can be. I will use, in this talk, a lot of "bilateral implant" or "the new bilateral implant", meaning the implant in the other ear.
Why would we want to consider implanting a child with a second cochlear implant in the other ear? For this, I was looking into some of the research, and I found that Dr. Peters has a White Paper (2006) on Cochlear America's website. He did an article reviewing a lot of the data that was available in scientific literature, presentations, and what he himself had found at his center, the Dallas Otolaryngology Cochlear Implant Program, and why we may want to provide binaural to cochlear implant recipients.
Why do we want two ears? The human brain is organized to receive and process sound from binaural sources so the brain can sample and compare the spatial, temporal and amplitude characters of an acoustic signal, and merge the incoming signals from two ears together. Normal-hearing brains use this rapid, real time analysis to hear from the normal ear. This is binaural hearing in normal-hearing ears and this binaural hearing is made possible by at least these three things: the head shadow effect, binaural redundancy and summation, and binaural squelch. These give us that binaural advantage which results in improved speech, understanding in quiet and in noise as well as sound localization ability. You may ask, "What is head shadow effect?" As a speech language pathologist, that was my question. In general terminology trying to keep this simple for me, a speech pathologist and teacher who may not get into all the very technical audiology terms as audiologists might do, the head shadow affect is how the head acts as an attenuator of sound so that the ear that is farther from the sound sources does not hear the sound as loudly or as quickly as the other ear that is closer to the sound source. This intensity and timing difference can assist in localizing sound. Also when noise is present, the ear that is furthest from the noise will have a more advantageous signal to noise ratio. I hope that makes sense to everybody.
Another binaural affect would be binaural redundancy and summation. This results in signals being louder and providing more access to softer sounds when you listen with both ears rather than one ear. With this bilateral signal presentation in normal-hearing ears, there is a redundancy with the information that results in an enhanced sensitivity to small changes and intensity in frequency. This can assist in understanding of speech in quiet.
Binaural squelch effect is the process from which our ears and brain receive both speech and environmental noise, and then focus on what you want to hear and tune out what you do not want to hear. In therapy if you have ever worked with children, we try to teach this skill, which I think to typically normal-hearing individuals comes automatically. We try to teach the skill of listening to the speech or to the person who is talking to them, and try to tune out the background noise. This binaural squelch effect helps with that. It reflects a central auditory system analysis that compares the interaural level and differences between two ears, and this can contribute to sound localization.
Why bilateral cochlear implants?
We want to give the individual the best access to sound and the possibility of developing some binaural skills which can assist in improving understanding and noise, localization of sound and greater ease of listening. Again the literature reports many potential benefits of bilateral cochlear implantation. It states that it can help in improved understanding in quiet or noise, improved localization ability, patient satisfaction and perceived benefit.
Let's go back to some of the research that was done on unilateral cochlear implants. A lot of this research comes from Sharma, Dorman and Spahr (2002) and what they really looked at was the auditory evoked cortical potentials, which is not a speech pathology term that we use very often. Sharma looked at auditory evoked cortical potentials, or the brain waves of children who had unilateral cochlear implants, and based on the speed of the response, this is an indicator of the maturity of the auditory system. She measured P1 latency. This is an indicator of the maturation of the central auditory pathways, and it correlates to those pathways that are more mature seeming to have better discrimination of speech. In some studies that they did, they looked at the P1 latencies of normal hearing children. This measure would be considered the typical. They also looked at children from under 3.5 to over 7 years of age who had received cochlear implants, and unilateral cochlear implants in less than 3.5 years of age. Most of those children's P1 latencies are within the normal range compared to typically hearing children of that same age. This tells us that the P1 latency is an indicator of the maturation of their central auditory pathways. In children who were age 3.5 to 6.5 years of age and received a unilateral cochlear implant, about 50% showed P1 latencies comparable to normal hearing children and about 50% fell outside of the norm. In children who were implanted with a unilateral cochlear implant over 7 years of age, these children generally did not have P1 latencies that were comparable to normal hearing children. It was concluded that the central auditory system requires sound input in the first few years of life if effective central auditory development is to take place to get maturation of the auditory pathways. There is a sensitive period of about 3.5 years during which cochlear implantation can occur in a highly plastic central auditory system and that implantation after 7 years occurs into a reorganized central auditory system. Sharma concluded that the P1 data suggested that for most optimal central auditory development occurs during the first 3.5 years of life. There is some variability in the data to 3.5 to 7 years, and that in all likelihood the sensitive period ends at age 7.
These findings also correspond to the practical application that Kirk et al. (2002) found; in that children with congenital deafness younger than 4 receiving an implant, developed significantly better speech and language compared to those children who received their implant after 6 or 7 years of age. If clinically you are working with children and have worked with children getting their implants under 3 versus a child over 6, we can mostly agree that we see those same results with children with severe to profound losses. It is going to be different if the child had some access to sound before.
P1 Latency and Bilateral Cochlear Implants
Now we have all this information about the P1 latency and unilateral implants, what does it have to do with bilateral cochlear implants? In terms of candidacy, is there some kind of sensitive period or window of opportunity like there is with unilateral implants for the bilateral cochlear implant, or can we implant at any age and expect the same kind of outcomes? Dr. Peters, in review of the literature and continued research from Sharma (2002), says the conclusion is that the same sensitive period in time course for normalization of the central auditory evoked potential is known to exist for the second implanted ear. He also says that early implantation and longer term cochlear implant use in 1 year was inadequate in preserving the plasticity of the auditory pathway that serve the opposite ear and almost seems to be kind of ear specific. He went on to say they did some research on the children tested at their center and were able to find that the trajectory of P1 latency change, for children with the second implant ear, was similar to the trajectory of children who received their first implant at the same age, as those who received their second implant. This meant for children who received their first implant less than 3.5 years of age, their P1 latency was found to be more comparable to normal hearing children. Also if you received your bilateral implant under 3.5 years of age, the P1 latency was also within that normal range with normal hearing children versus if you got your first implant after 7 or bilateral cochlear implant after 7 as they did not fall into that normal P1 latency compared to normal hearing children. This was strong evidence that there is a sensitive period or a window of opportunity to acquire effective binaural integration from that second ear.
The conclusion was that window of opportunity for children to maximally develop central bilateral mechanisms from that second ear would seem to be highest under 3.5 years of age, intermediate potential up to 7 years of age, and minimal potential over 12 years of age despite being high performers with their first implant.
This is not all dependent upon the age. Another big factor is auditory stimulation in the other ear. Dr. Peters' conclusions were that, in the absence of consistent contralateral hearing aid use, children less than 8 years of age were more ideal candidates. They were reluctant to implant the children over 12 who did not use a hearing aid in the second ear until at least 6 years of age, and that with continued hearing aid use, children of any age could be considered a good candidate. This goes back to if there is auditory stimulation in that other ear and there is some residual hearing, they are getting some benefit from it, and the age factor becomes less important. Again the two factors are age and the amount of auditory stimulation in the other ear, or if the child is post-lingually deafened make a big difference. The age of the second implant has significant benefit factored in with their willingness to use the second device. Younger age is better, and we also have to take into consideration how much auditory stimulation was in that other ear.
To review, some of the bilateral candidacy factors are age and cochlear anatomy, keeping in mind that sometimes the first ear was implanted for reason, and that reason may have been because it had the better anatomy which is something that we have to consider if we are going to be implanting that second ear. Hearing aid use is a factor. However if they have not been wearing a hearing aid, have not been stimulating that side, and they are older, it is not as likely to have benefits versus a child who has been wearing a hearing aid in that side and getting some benefit from it. Then we have a little more leeway with the age factor there.
Previous implant and performance and language comprehension is another factor. We need to be careful when we are talking about children who have multiple issues or significant language issues in thinking that if give them a bilateral cochlear implant, that will help them. That is not always the case. We need to determine if they have an access to sound issue, language processing, or a cognitive issue. The bilateral implant can give them the access to sound, but the bilateral is not going to change language processing disorders. It is not going to change cognitive issues. What are the expectations and why would you want to give bilateral cochlear implantation with that? Looking at the patient and family motivation, especially if this is an older child who had their first implant at 2 or 3 and now they are 10, 11, or 14 years of age, motivation is going to be very important, and pre versus post lingually deafened. As I already mentioned when post lingually deafened, they will most likely have a better benefit than prelingually deafened.
One more time to reiterate, those who can expect better outcomes would be children who:
- are younger and are not having other issues going on;
- have utilized a hearing aid in the other ear and are demonstrating some benefit;
- may have had progressive loss as we know that they would have been stimulated in that ear and have had some access to sound for meaningful period of time;
- have normal anatomy;
- showed significant benefit with the first cochlear implant;
- were post-lingually deafened at any age.
I would like to spend the rest of this talk addressing what we are going to do in the therapy setting.
Focus of Goals - Simultaneous
When I am working with a child, whether they are getting hearing aids or a unilateral cochlear implant, bilateral simultaneous or bilateral sequential, I think of three main areas that I want to work with this child to develop their listening and spoken language skills.
The first area is auditory skills and the auditory skills pyramid. In my mind, I break that down into two separate auditory skills. The first part is auditory discrimination or speech perception skills, and the second part being the processing comprehension, the receptive auditory skills that are coming in with that. The second area is the hierarchy of speech intelligibility which is developing speech language production. The last area is language levels which is developing the verbal expressive language skills. For a child who has received a simultaneous bilateral cochlear implant, it will be the same as if they are getting a unilateral cochlear implant. They are now on the track so let's develop their listening and spoken language skills.
We are going to focus on the auditory hierarchies with perception, receptive language, speech production, and verbal expressive language. Basically we will have the children wearing both implants at the same time and will be working on all three of those different hierarchies. There may be some times when we might work with one ear versus the other ear to monitor or get a sense of how they are doing with speech perception. You might want to start a session with doing the ling sounds for each side to see if they are "on the air" with both cochlear implants. In general, however, when you are trying to develop the language, the listening and spoken language, you are going to be working with both ears together. That is why I say that therapy will be the same as what you would do with the child who has a unilateral cochlear implant. There are many, many talks on HOPE Online. I know I have done a few. Ashley Garber has done many, and quite a few other people have presented about therapy for developing listening and spoken language skills with a child with unilateral cochlear implant. They would be applicable for a child who has received a simultaneous cochlear implant, bilateral cochlear implants.
Focus of Goals - Sequential
The sequential cochlear implant is two separate surgeries. Those children who received that second surgery within three to six months of the first surgery, I lump them into the category of simultaneous cochlear implant. Because 3 months post, 6 months post of that first cochlear implantation, they have not developed high level speech and language skills at that point. They are still learning those skills. We do not see as much of a difference between the ears. I spend most of my time with those children working on speech and language development with both ears, working with the ears together, and treating them as a simultaneous cochlear implant child. When I am talking about a child with sequential implants and how we might treat it differently, this is a child who has developed some level of listening and spoken language skills with the first implant and then with the second bilateral implant. We need to work on those skills to get them to meet the level of the first ear. What we work on with these children is different. Going back to the hierarchies, we are definitely going to focus on auditory, but more of that speech perception, auditory discrimination, and auditory memory, not necessarily all of the receptive auditory language goals.
When it comes to speech production and expressive language goals, they should always be utilizing both cochlear implants. We do not want to penalize a child and make them work extra hard at learning how to do speech sound production with the new implant alone when they have better access to sound with the old implant. Our primary goal is speech sound production, so let's give them the best access to sound possible. This is where the therapy is going to be a little different. When we are looking at the therapy, we always want to be monitoring the skills. Our long term goal is to develop the auditory skills of the new bilateral cochlear implant to the level of the first ear. We start with closed set and progress to open sets. We start with structured activities moving to more unstructured activities and start with simple concepts, vocabulary, and then advance to more complex.
Auditory Skills Pyramid
Figure 1 shows my auditory skills hierarchy. We will move up through the hierarchy, starting at the beginning as we would with a unilateral. Because these children have not really learned to listen with the implant in that ear, we have to start at the bottom building those basic listening skills and giving them confidence that they are hearing something and can possibly attach meaning to it. We will do a lot of emphasis at level 3, and some parts of level 4 and 5.
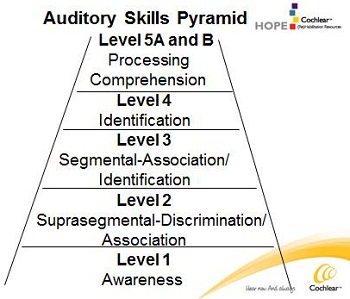
Figure 1.
Sequential Bilateral Habilitation: Auditory
Our sequential bilateral habilitation is going to focus on the auditory aspect through awareness to pattern perception, to focusing on speech discrimination, to identification, to processing comprehension and then localization and background noise as some of our goals. These are going to be your general goals. As I previously said, the two main goals under auditory are going to be speech discrimination/auditory perception and the auditory comprehension of longer chunks of information. If you are working on developing receptive language skills such as teaching vocabulary and newspaper concepts, try to do that work with both cochlear implants. We do not want to make it harder for them to learn language than it already is. Give them the best access to sound when teaching new information. What we are trying to accomplish with the bilateral is improving the listening skills which is that speech discrimination and auditory memory of longer chunks of information.
Auditory goals - Awareness and suprasegmental-pattern perception. We start with level 1, which is awareness. This is the same as what we do with the unilateral. We want to make sure they can respond to all of the Ling sounds for the same reasons. Can they hear the high, mid, low frequency sounds with that? Then we move to suprasegmental-pattern perception. We definitely want to work on this level a little, because I feel this is where we start to give children some confidence in their listening skills. If we start with more of a closed set and they are not at the segmental aspect yet of picking out different words but they can hear patterns, it makes them feel kind of confident that they are hearing something with this ear and can attach some meaning to something with this ear. You have to remember some of these children have very well-developed listening and spoken language skills or highly developed listening skills with the old ear, and now they have to start over with this new ear. We are going all the way back to the "baby steps" again and that can be a little daunting for them or scary. We want to make sure we build confidence in increasing the size of the sets.
Auditory goal - Discrimination. We have awareness, and then move to the pattern perception. Then we get into the area I think we really need to be focusing on which is what I consider my level 3, and this is auditory discrimination. This is speech perception, really fine tuning the listening skills. What is the clarity of sound that they are getting from that cochlear implant on the new side? Are they really able to hear sounds as being different or do a lot of the high frequency sounds like S and SH sound very similar to them? It is hard for them to discriminate that. We go through speech sound differences and isolation to segmental differences. Then I have added in tracking, as in my mind, I think of it as a discrimination task.
Discrimination auditory activities. Can they hear the Ling sounds as being different? We are taking the rhythm or difference away, and are listening for the segmental vowel consonant differences. Can they hear the finer differences? We start with words that are further apart and smaller sets such as "shoe", "ball", "cup", "book". When we bring the words closer together like "book" vs. "boat" or "horse vs. "house", can they start to hear those kinds of differences? You want to increase the size of the set. This is the fine tuning of listening. If they can kind of do it, and get placement and voicing differences, can they then listen to sets of words, vowel-only differences like "kite", "cat", "coat"," cut", "cute"? Then to make it a little bit harder, let's go into the consonants. Can they hear it by manner, which is the easiest to hear, like "shoe" vs. "boo" vs."moo", or by voicing, which is the next harder to hear like "coat"vs."goat" or "sad" vs. "sat"?
The final position seems to be a little harder. Can they hear it by place of production, if the manner and the voicing are the same? Can they hear the difference between place of production as in "Kate" vs."cape" vs. "cake"? With speech acoustics, there are different lists available or tools that you can go to like the SPICE or the CAST. I will have a reference at the end of the presentation to help you with that. I also like to make it a little more challenging. You are doing this at the word level and really listening. Can they hear the sound difference in the words too, at the sentence level? If they are a little bit older and you are working on Kate-cape-cake, you might say to them "Draw a circle around Kate and underline cape". If they are younger, one of the things that I like to do is have younger children manipulate objects with this. There is a company called Discovery Toys and the objects are called Mini Motors. You can get a little rubber box of vehicles with airplanes, boats, trains, and cars, and they are in different colors. I might put out a blue airplane, blue car, blue train, purple airplane, purple car and purple train if I am doing a voicing difference with "coat" vs. "goat". If they are working at the world level, I might put out an airplane, a car and a train with two orange, two blue, and two purple. Then I would say "Put the purple plane on the coat and put the blue train on the goat." With this, there is even more discrimination. Not only are you working on auditory memory, but you are having them do discrimination at a more difficult level than just the word itself. We are really working on whether they can hear those fine sound differences and hang on to them.The last discrimination task that I wanted to talk about was tracking. There are different types of tracking that can be done. I use it as the definition of repeating verbatim. To me it is really working on pure auditory discrimination and kind of auditory memory. If I say "The boy is sleeping," I expect the child to come back with "the boy is sleeping", not "the boy sleeping" which tells me they have missed the word "is". If I say 'My friends and I played baseball", and they say "my friend and I played baseball," I feel like they missed the plural "s". Is that an auditory discrimination and they did not hear the s at the end? This is what I am really looking for when I do the tracking.
For younger children you can certainly use some familiar phrases. I have done this with children 3.5 and 4 years of age. Frank Schaffer's Easy Action Picture flash cards are nice. I do not show them the picture first, but I might say repeat after me, with a familiar routine phrase, like "Open the door." Can they come back with that? Examples are, "Be careful", "It's hot" "Tie my shoe." They might say to me "oe" which means they have got the rhythm and intonation, but maybe they missed the "sh" in there or did not quite get that. This is what I am looking for in the tracking. For older children, start with simple sentences and then making it a little more complex. It gets a bit more challenging when we are working on some of these activities; because we have to keep in mind some of these older children have good language skills and good language strategies. Even if they did not quite hear a word in a sentence, they might be able to use the sentence to figure out what the word was. We do not want to necessarily be working on the language. We should try to work on their listening, set these goals up carefully, and be challenging. I might use the example, "Dad worked hard and was very fatigued." They were probably thinking I was going to say "tired", but I said a different word. I really want them to listen for that. What did they hear? Can they say that back to me?
Things that you can use for the older kids are their textbooks and currently assigned reading. Why not give them a review of their homework to begin with? Another activity for this auditory tracking, particularly with older kids is what I call iPod® therapy and having them listen to music. They can have the lyrics printed out. As they are listening along, they can see what the words are to help with that discrimination and did they hear the ending on that sound, and so forth. They can listen to books on tape and follow with or without the book in front of them. If they are still in the early stages, you might want to have the book in front of them. Watching and listening with closed caption off to a familiar movie is another activity they can do. Even with younger children, you can do this, especially if that child has watched 101 Dalmatians 30 different times, which they tend to like to do. Then go ahead and take the old implant off. Keep the new bilateral cochlear implant on and have the child watch the movie they are familiar with. They may know certain lines at certain points, and can listen and be able to pick that out a little bit.
Auditory Goal - Identification. We are now up to level 4 of our goals which is identification, picking out key words in a sentence. This level for me is all about the auditory memory. We are working on listening to shorter and longer sentences, picking out more key words and listening, moving from more of a close set of choices to more open set. At this level, keep in mind that listening and auditory memory is not teaching new vocabulary, and not teaching new concepts. You want to use information that the child is already familiar with. Eventually you might want to make it a more challenging goal, but initially I keep separate in my mind that I am working on trying to develop their listening skills or working on developing their language skills. If I am working on language, I am using both cochlear implants. If I am working on listening, I am doing it with the new bilateral cochlear implant alone.
Auditory Goal - Processing/Comprehension. The last level up at the top of the hierarchy is the auditory goal of processing/comprehension. So again are you working on listening alone or are you working on new concepts and working on language? Some of the goals you can work on with the new bilateral cochlear implant alone are working on paragraphs by listening to a larger chunk of information trying to see if they can discriminate with this larger chunk, and maintain that information that is familiar information, and also listening in a conversation. If you are working on developing new vocabulary, working on more challenging questions, cognitive language skills, inferencing, learning how to define and explain things, you should be using both cochlear implants, and this is how this differs in the therapy.
Processing/Comprehension auditory activities. When working with paragraphs, you want to start off with simple paragraphs and move to paragraphs with more complex information. I already talked about why we would want to use familiar information. You start with shorter and move to longer kinds of paragraphs. For older children, you can use news, current events, and magazine articles. For younger children, you can show them a picture and tell them a short little story. You should use what is age appropriate for that child.
Then there is conversation. This is kind of the high level. You want to work on whether they can follow a conversation if they know the topic, to a conversation where they do not know the topic. If you want you can set up situations where you might say these are three things that we are going to talk about such as baseball, the snowstorm we had last week, and Christmas. They will then have a sense of what the vocabulary might be and then transition this to be open ended, particularly for older children. Adding in participants to the conversation is next, and be done with better opportunity in the classroom. Not only do they have to follow along, but they will have localization and background noise as well. Practice comes into play with this because if it is a small group in which you are having a discussion and someone adds to the discussion, are they able to localize where that question or comment came from?Something else we would add in, but would not necessarily put primary emphasis on with the unilateral implant, but with both implants is working on localization. I will admit this is a challenging area for me in therapy as it is very hard to set up situations for the child to localize to a sound. I can hide a noise, like an alarm clock that goes off 10 minutes into the session and see if the child can determine where the noise came from, not just in a general sense, but even more specific, tuning into exactly where it was to actually finding a ringing cell phone. You can have two or more people in a room making noise in different parts of the room to see if the child can localize where it is coming from, or just having someone make a comment and see if they can localize.
The one thing you need to be careful about is discrimination versus localization. If you have a male speaker and female speaker, they might know a male voice versus a female voice. This was not necessarily localization, but it was a discrimination task. All these things should be kept in mind as it becomes more challenging. This is the same with using different noisemakers. If they know that the drum is to the right of them and the tambourine or the ringing bell is to the left, they can discriminate the different sounds. They heard the drum and know which direction to look without to having use a localization skill. Trying to keep the sounds or the speakers such as two female voices that are somewhat similar is what I find to be a challenging one. Real life in-classroom situations are great in that you want to maximize all the natural opportunities that come along, and again in that natural environment, you can point out localization with "Did you hear that? Where did it come from?
There is also background noise. I do work on this sometimes with children who have a unilateral cochlear implant, but certainly with the bilateral cochlear implants, we want to push this a little bit more. This is not scientific. In my therapy room, I usually have a radio. Not measuring the decibels on it, I start with it on kind of low with doing simple tasks like following directions. The radio would be the background noise. This is where we try to teach them to do a binaural squelch, where they tune out what is not important and tune in the speaker, which is what is important. Then as they are getting better with this, you can increase the noise. You do not want to make the background noise louder than what you are presenting your directions at. This gives them a chance to learn how to tune out the noise and tune into what is important.
Auditory Habilitation
In the classroom, if you are learning new information, or you are in a learning environment, then I would like that child to be wearing both cochlear implants. I do not want to make them work harder than they already are. In therapy, your frequency and the intensity, and how much you are going to work on developing the listening skills in the new cochlear implant ear will depend upon the child's overall listening, spoken language, and academic skills. When I think about bilateral cochlear implants, in my mind as a speech language pathologist, my primary goals are listening, spoken language and academic development. I do not want to sacrifice that to try and develop listening skills in that second cochlear implant. If they have speech and language disorder or delays going on in academic issues, I would not devote all of my time to just the new listening skills. I will devote some of my time to hone up and develop those listening skills, but primary importance is developing the speech and language skills. This is going to depend upon the child. Usually I say to take 10 minutes out of a therapy session in the school and work on some of these different skills such as awareness, the pattern perception to some of the speech perception, to then working on following directions, auditory memory tasks, to paragraphs of information with some conversation. Then at home have them work on conversation with the parents.
When the child gets a new, second cochlear implant, we do not say take the old one off and spend the whole weekend with the new one alone. If they have developed language with that first implant and very minimal skills with the new implant, you will have a very frustrated and unmotivated child. You have to ease them into it. This may be just 20 minutes right before bedtime. Pull out a very familiar book that this child knows. Take the old implant off. Sit down. Read the story with the new implant on. Let them learn to get some confidence in their listening skills with this new implant and then we can up the time. You can do activities of playing a familiar game such as Go Fish with very common vocabulary or as I said before watching the 101 Dalmatians movie for the 39th time. As they develop skills, it can be transitioned to a few hours. We really want to strengthen the auditory pathways on that side by giving them some time, but it is not an all or nothing. We do not want to throw them in there and take the old implant off.
It is my experience or the experience that we have had at CHOP, in those children that have been deemed to be appropriate candidates, auditory skill development in the second ear generally becomes similar to the auditory skills acquired in the first ear by 12 months of that bilateral use. It is really amazing to see. I had a patient who had a cochlear implant in one ear, and received a second cochlear implant for one month. What she was doing with the second ear by one month post implant took her 6 months post implant with her first ear. We sometimes see those rapid gains, and by 12 months they can be equal with their ears, but it is not the same for every child. Again it is all about the candidacy, how much stimulation they had on the other side, what age did they receive the implant at, and all of these other factors that I have talked about previously. We have to keep monitoring, following along, and setting appropriate expectations with that.
I have added some resources for you at the end of this presentation. I talked about the SPICE and the CAST for speech acoustics with word lists for voice, manner or place, or vowel differences. I use some of my favorite books for following directions, listening to a paragraph of information, etc. Other resources are from Jean Gilliam DeGaetano and Marilyn Toomey, with SuperDuper. I am not the most creative person in the world so I look to other things, and with these resources, you do not have to create it yourself. You can look to those sources for some of the auditory following directions. Cochlear Americas has Sound and WAY Beyond ™ that really goes through hierarchy of the listening skills. They also have additional papers and guidance on their website with regard to bilateral cochlear implantation. I could not put all of that information into this talk.
Know the research. Understand what bilateral cochlear implants are about and how to set realistic expectations. Certainly children can benefit from this. Benefits are going to vary just as they do with unilateral cochlear implantation. Know the different types of outcomes and how they affect our therapy. If the surgery is simultaneous, it really does not affect our therapy. We want to focus on developing the auditory skills, speech production and expressive language skills. If it is sequential, it does affect our therapy approaches and we will come at it from a different angle. Focus on developing auditory skills with the newer implant. The, auditory memory skills, receptive language, speech production and expressive language are going to be done while they are wearing both cochlear implants with that.
Donna: Great talk, MaryKay. MaryKay has shared her contact information if you have additional questions you want to send those to her. Always contact me if you have questions about HOPE. MaryKay will address the questions.
How do you differentiate between a power struggle and rejection in a child who does not want to wear a second cochlear implant?
MaryKay: First you need to look at the candidacy and try to get a sense if this is going to be something that might be a struggle for this child. For example, if they are 14 years old and they have never worn a hearing aid in that ear. There has not been auditory stimulation. You should ask what we are going to set as our expectations for them versus the three-year-old who has been wearing a hearing aid in the other ear and does very well with the first cochlear implant. One of the first things I look at is what would I expect, and again this is not an all or nothing. You do not just take the other implant off. You try to ease them into it. We have had those situations where kids really just do not want to take that first implant off, which is not a bad thing. It tells us they bonded to that first cochlear implant. We can try to ease the new implant in for maybe 10 minutes, and we do a few activities, while letting the coil hang. We do not take the whole implant off so they know it is there and that it can be put back on right away. This builds confidence and is the big thing we try to work through in making it positive for them. This is most likely the best way to start to work through some of those issues.
I have heard about some children who rejected the first implant after receiving the second implant.
I will admit, in very rare cases, I have seen that. The only reason I can think of behind this is that maybe we did not implant the better ear, and they actually get better benefit from the new bilateral cochlear implant than they did from that first ear. Unfortunately we do not have the technology to be able to test all the neural integrity to say this is the better ear. For whatever reason if that child is feeling like they have better access to sound and better discrimination abilities from the new bilateral versus the old, I say go for it, depending upon the age of the child. We would like them to wear the other one because it can give them some of these other benefits. However if they want to use that new bilateral as the stronger ear, and it has a stronger performance for them, there is nothing wrong with that. Again I can only say maybe it captured the better ear that second time around which is another benefit of bilateral cochlear implant with that.
Do you have any experience with single sided deafness in children, cochlear implant recipients?
No. I personally do not have experience with any children who have received a unilateral Cochlear implant, but actually have typical hearing or significant hearing in the other ear. They have to meet FDA approval which is severe to profound loss, and they have to have significant hearing loss in both ears.
Would you go bimodal with a three-year-old with neuromyopathy or what is also referred to as auditory neuropathy?
This might be more of a question for an audiologist and I am a speech language pathologist coming from the therapy aspect. I would probably say that you provide therapy and monitor the progress. If you do not see progress being made, you may want to consider it. That is my best response to that question. You know it is easier to try the bimodal because it is not as invasive, not a surgery. I have no problem with saying it is all right if they are using a unilateral cochlear implant. This is what they are doing, why not do a trial period with a hearing aid in the other ear to see if there is any benefit from it or not. It is not an invasive procedure. Then you monitor the progress. Set very specific goals, monitor the progress, and look at what the outcomes are.
Do you always wire an FM to the CI side if the child is wearing a CI and a hearing aid?
I am not an audiologist, but I will give you my speech pathology thoughts. Some of these are questions you ask the audiologist. You would want to provide the access to the side that has the most sound. If the better access to sound is the cochlear implant, then you are going to want to put the FM to that side versus giving it to the hearing aid which may not have as much access to sound.
What is the frequency of speech therapy sessions post simultaneous implant for a child?
This is another one that is very child specific. Individualized family education, service planner individualized educational plan. There is also the difference between 0 to 3, 3 to 5, and 5 and over. This is really dependent upon the child's needs. I have in the past talked about how you want to front load services for these children. Give them all the services up front with that. There is no set response that I can give with a specific formula such as "if this is what they are doing, this is what the services are." You have to look at the child specifically and individually to determine what the frequency and the intensity of the service will be that they will need.
What is the rationale for a surgeon to want to do a sequential approach?
It is the length of surgery and the amount of time the child is under anesthesia. They also take a look at what they are doing with that first implant a little bit. This surgery can give the parents a chance to get used to all of the equipment. I think really the big surgical part of it is the length of surgery, and then we want to look at how they are doing with it and how the family is handling the equipment.
Will this information be applicable to a child that has the second Cochlear implant surgery four years after initial implant?
This depends upon age of the initial implant. If the child were 2 at the time of the first implant, and the child is now 6, it might be better for them, versus if the child were 6 at the time of the first implant and now they are 10 getting the second bilateral. I would think they are not going to have as good of outcome.
What would you recommend regarding implants for older students who have experienced progressive hearing loss and their aids no longer give them speech understanding?
If they had stimulation, had more of that progressive, and were post lingually deafened even though they are older, they are more likely to get better benefit with that. You have to look at each child specifically, but have the audiologist look at it. Certainly it may be an option for that child.
Would I apply the same candidacy groupings from the AuSpLan plan and cochlear implantation?
I have not done it quite that cut and dried. I will admit at CHOP we have talked about doing a bilateral candidacy protocol looking at children for the bilateral cochlear implant. We have not quite applied "Do we think if they are familiar with AuSpLan they are more of an A candidate, B candidate or C candidate," but we have done general narratives. Throughout this talk you should have gotten a sense of who might be a better candidate or who might be able to get some better binaural affects. I have not done specific to that.
What is the urgency of giving a cochlear implant to a child who is 6 years old that was hearing up to 4000 hertz and is now losing the hearing, but still has some reasonable benefit up to 2000 Hz?
I think you really need to look at the speech. That is an audiology question, but you need to look at what the child's listening and spoken language skills are. Are you seeing a regression in skills? If you are, this tells you they are not getting enough access to sound to continue to develop or maintain those skills, and then you may want to consider cochlear implantation. This is something you should be working with and talking to the audiologist about. It might be time to start looking at cochlear implantation.
With the 10 minutes focused therapy, was that for 30 minute session or 60 minute session?
This would be for a 30 minute session, but it depends really on what the overall speech and language or listening and spoken language skills are of the child. What is the primary focus? If you have a 30 minute session with a child who is behind in their skills, you want to give a little bit of time (maybe not 10 minutes, but six minutes), but keep your primary focus on developing the listening and spoken language skills.
For a child that uses an FM in the older cochlear implant ear, would you want to put an FM in the newer Cochlear implant ear?
I am definitely going to refer that to the audiologist. I think again that is going to be very specific as to all the different benefits they are getting from each ear and can you integrate the systems together.
Donna: We will research that question and send an email out. I agree with MaryKay that is an audiology question and probably something that there is some difference of opinion on. This has been a terrific session, MaryKay. We all thank you. It has been very interactive. You had terrific questions. So please join us again at HOPE Online. Send your feedback form back to the address on the form.
MaryKay: I wanted to add if I was not able to answer someone's questions, please email me. If it is an audiology question, I will send it off to our mapping audiologist at this center and they can maybe help you with that. Again, thank you everyone for sitting through this presentation.
- SPICE (Speech Perception Instructional Curriculum & Evaluation) - www.cid.edu/home.aspx
- CAST (Contrasts for Auditory & Speech Training) - www.linguisystems.com
- Jean Gilliam DeGaetano - www.Greatideasforteaching.com
- Marilyn Toomey - www.childrenspublishing.com and www.superduperinc.com
- Sound and WAY Beyond™ - www.CochlearAmericas.com/HOPE
Brown, K, & Balkany, T. (2007). Benefits of bilateral cochlear implantation: A review. Current Opinion Otolaryngology & Head Neck Surgery, 15, 315-318.
Ching, T. (2005). The evidence calls for making binaural-bimodal fittings routine. The Hearing Journal, 58(11), 32-41.
El Fata, F, James, C, Laborde, M, & Fraysse B. (2009). How much residual hearing is 'useful' for music appreciation with cochlear implants? Audiology and Neurotology, 14(S1), 14-21.
Kirk, K, Miyamoto, R, Lento, C, Ying, E, O'Neill, T, & Fears, B. (2002). Effects of age of implantation in young children. Annals of Otology, Rhinology, and Laryngology-Supplement, 189, 69-73.
Litovsky, R, Parkinson, A, Arcaroli, J, & Carol Sammeth (2006). Simultaneous bilateral cochlear implantation in adults: A multicenter clinical study. Ear and Hearing, 27(6), 714-731.
Peters, B R. (2006) Rationale for bilateral cochlear implantation in children and adults. 2006. Cochlear Americas White Paper. Available at: www.cochlearamericas.com/PDFs/bilateral_white_paper.pdf
Peters, B.R., Wyss, J., & Manrique, M. (2010). Worldwide trends in bilateral cochlear implantation. Laryngoscope, 120 Suppl. 2, S17 - 44.
Sharma A., Dorman M., & Spahr A. (2002) A sensitive period for the development of the central auditory system in children with cochlear implants: Implications for age of implantation. Ear and Hearing, 23, 532-539.
Sharma, A. & Nash, A. (2009). Brain maturation in children with cochlear implants. The ASHA Leader, April 14, 14-17.
Sucher, C, & McDermott, H. (2009). Bimodal stimulation: benefits for music perception and sound quality. Cochlear Implants International, 10(S1), 96-99.
