
Editor's Note: This is part of a series of six expert seminar presentations and articles on the human side of the fitting process. This series is being presented throughout 2009, and is designed to walk through the hearing aid fitting process from beginning to end with a focus on the human factors that are at play each step along the way. Tools and strategies will be discussed that can assist in ensuring that the patient receives the optimal benefit from modern hearing aid technology. It is designed to be a complement to more typical discussions of hearing aid technology and fitting verification. Please see the accompanying recorded seminar on this topic in the AudiologyOnline eLearning library. Further courses in this series, "Customizing Advanced Technology Fittings" and "Motivating the Older Patient to Take Action" can also be found as recorded and text-based courses in the AudiologyOnline eLearning library. Look for upcoming live courses in this series - Special Fitting Considerations, the Fine Tuning Process, and the Follow-up Process - that will be presented on 9/11/09, 10/30/09 and 12/4/09. Further details can be found in the AudiologyOnline course listings.
Every successful dispensing audiologist, at some time, has heard a variation of the following statement from a patient: "I really didn't want to get hearing aids but now that I have them, I know it was the best thing I ever did." This is a powerful statement that captures two important realities about the dispensing process. First, the typical new patient is hesitant about entering the process of seeking amplification. Second, in most cases, the dispensing process ends with the patient being satisfied with the outcome (Kochkin, 2005). What does it take to bring a patient from an attitude of hesitancy to one of relief and gratitude? There are many factors that must go well throughout the process to obtain a positive end result. The challenge is that many of these variables are out of the audiologist's control. However, one of the keys to the success of this process is ensuring that the patient's expectations are in line with what the audiologist can realistically deliver.
Just because a patient has agreed to enter the hearing aid process, it does not mean that the patient is fully committed to the concept of being a hearing aid user. There are many opportunities throughout the process for the patient to back out. Patients are afforded the reasonable legal right to change their minds. Yet, if the audiologist sincerely believes that the patient will benefit from amplification, then every effort needs to be made to keep the patient moving in a positive direction. All too often, patients enter the process with the expectation of failure. Perhaps they agreed to a trial of amplification only to appease a spouse or other family member, or perhaps they heard negative reports from acquaintances for whom the hearing aid process did not end well.
While no audiologist can guarantee positive results, it is a reasonable assumption that nearly all patients should receive some level of benefit from amplification. The key is to ensure that the amount of benefit received is acceptable to the patient. The best way to ensure satisfaction is to make sure that the patient's expectations are realistic throughout the process, and that the patient allows enough time to experience the benefits of amplification.
This paper addresses two keys essential to managing patient expectations:
- The focus of the process needs to be placed on the professional care provided by the audiologist and not on the hearing aid technology.
- The patient needs to take ownership of the process, with a successful outcome engendering a sense of accomplishment for the patient.
What is Expected?
What is the mindset of the typical patient entering the hearing aid process for the first time? As discussed in a previous paper in this series (Schum, 2009), many first time users are reluctant to seek out audiological care. If they do, they may have many preconceptions about hearing aids and the professionals who dispense them. These preconceived ideas can have a negative effect on the dispensing process. Some patients may be naïve to the complexities of hearing loss and the limits of amplification, leading them to expect a simple solution to a problem that is far from simple. If they have spoken to individuals who have had negative experiences, they may be suspicious of the whole process and even of the audiologist. At the first sign of trouble, these patients may be ready to end the process.
Another more subtle mindset is ambivalence. As discussed by Schum (2009), many older individuals experience increased difficulty making major life decisions. They may have a sense that something needs to be done about their hearing, but they are unsure of how to take action. They may be experiencing a decrease in relevance in their personal and professional lives. They may no longer serve as the family matriarch or patriarch, no longer hold a professional position of authority due to retirement, or have experienced failure in other recent ventures leading to an erosion of self-confidence. If ambivalence is at the core of the patient's mindset, it may be difficult for the patient to make constructive, positive decisions about his or her own care.
Clinicians have known for years that patients typically expect more than what hearing aids can realistically deliver. Sensorineural hearing loss creates distortional changes to sound processing that cannot be completely eliminated by hearing aids. Despite advancements in hearing aid technology, communication in challenging environments is still difficult, even for those with mild and moderate hearing losses.
Schum (1999) assessed the perceived benefit of hearing aids for a group of newly fit patients using the Hearing Aid Performance Inventory (HAPI). He also assessed expected benefit prior to the fittings using a modified version of a subset of the HAPI. Figure 1 provides the expected and actual benefit on the four subscales of the HAPI. Expected benefit was typically found to be greater than actual benefit, even in challenging listening environments such as background noise.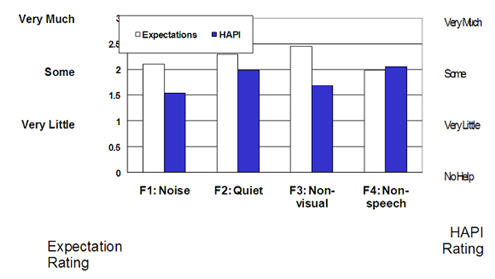
Figure 1. New patient expectation ratings along with subjectively rated benefit after adjustment to amplification (Adapted from Schum, 1999).
Does the fact that new users expect more from hearing aids than can be realistically delivered mean that patients are disappointed? Apparently not. The MarkeTrak data reported by Sergei Kochkin (2005) have shown that the majority of patients fit with hearing aids over a number of years rate themselves as either "Satisfied" or "Very Satisfied". These results suggest that ultimate satisfaction with hearing aid fittings is due to more than whether or not the patient's initial expectations were met.
In a similar study to Schum (1999), Cox and Alexander (2000) compared the results from the SADL, a hearing aid benefit scale, with the ECHO, an expectation scale. As with Schum (1999), over-expectation on the part of patients was documented for the subscale concerning listening performance with hearing aids. However, on the subscale relating to service and costs, there was not a mismatch between expectation and performance. This subscale related to how well the professionals who performed the fittings were able to provide effective care for the patient. The patients in the Cox study had high expectations prior to being fit, and the professionals were able to meet those high expectations. These results speak to the influence that an effective audiologist can have on the patient's perception of the clinical outcome.
Complicating Factors
Patients come to audiologists with a wide range of personalities. One factor that has been identified as affecting the hearing aid process is locus of control (Cox, Alexander & Gray, 1999;Garstecki & Erler, 1998). Locus of Control refers to whether a person feels in control of his or her life (internal locus of control), or that life is under the control of external forces such as other people, fate or a higher power a (external locus of control). Patients with a stronger external locus of control were less likely to follow through on hearing aid recommendations (Garstecki & Erler, 1998). Patients who enter the hearing aid process feeling that they are a victim of external forces may tend to expect hearing aids and the audiologist to fix their problem. They may not view themselves as having a role in the outcome. Although audiologists cannot change a patient's core personality, it is important to impress upon the patient his or her important role in the outcome of the fitting. Patients can do many things to become more effective communicators and to give the newly fit hearing aids the best chance to be of benefit. They can understand that adjustments will be necessary in many new fittings and that experiencing side effects from the start is not unusual. Patients need to clearly communicate back to their audiologists in order to solve initial fitting issues. All of these things will not necessarily come naturally to a person who does not have a strong innate sense of control over the world, especially those who enter the process hesitantly or suspiciously.
Family members, such as spouses or grown children, can be a valuable asset during the fitting of amplification. However, the audiologist should be aware that family members can also exhibit behavior patterns that can complicate the process. In some cases, family members may be the ones with unrealistic expectations. Frustration over years of communication struggle may lead to the classic statement, "I want you to fix my mother's hearing." Although family members are usually the first to notice the benefits of amplification, there are cases where they expect a quick and complete fix to a complex problem.
If a loved one, especially a grown child, tries to direct the care of the patient too assertively, problems with locus of control or ambivalence may be exacerbated. In the health care context, grown children have been observed to prioritize the well-being of their parents over engendering a sense of self-efficacy (Antonucci, 2001). Successful hearing aid use requires active participation on the part of the new user and care must be taken to prevent well-intentioned family members from undermining the process.
Focus on Professional Care
According to Nelson et al. (1997), the principle factor accounting for satisfaction with a health care provider is the patient's perception of personalized attention to the patient's own agenda. Patients want to know that those who care for them are focused on their particular issues, rather than a one-size-fits-all approach. They want to feel that the professional took the time to craft a treatment that reflects their personal issues and concerns.
Kochkin (2000) noted a strong relationship between the estimated time a patient felt that the audiologist spent counseling and the patient's overall satisfaction with hearing aids. Patients do not want to feel rushed and they respond well when they sense that the audiologist has taken time to listen to their problems and concerns. The old words of wisdom seem to apply: patients don't care how much you know until they know how much you care.
While patients expect the audiologist to be the expert in assessing hearing loss and developing a rehabilitation strategy, technical skill alone is not enough. Patients have to choose to try, keep and use amplification, and the audiologist plays a vital role in preparing the patient to be in the best mindset to make those decisions. One of the most effective strategies to motivate and focus the patient to is communicate a sincere desire to mold the rehabilitation package around the specific experiences and goals of the patient. Further, the patient should see that a "rehabilitative package" involves more than the purchase of hearing aids. It includes a complete process of care by the audiologist and support staff (batteries, recall, upgrades, warranty & trial period, connectivity assessment, etc) that will follow the patient over time, providing the assessment, treatment and service that is required whenever the need arises.
The more that the treatment process is focused on the purchase of hearing aids, the greater the likelihood that the limitations of hearing aids will be an issue. The patient must be prepared for the reality that amplification, no matter how helpful, is only be one part of the solution. It is important to stress that the hearing aids were recommended based on a comprehensive and personalized assessment of the patient's needs and are supported by a host of professional aftercare designed to maximize their benefit.
Absolute Expectations and Potential Benefit
As suggested above, the patient may enter the process without understanding what hearing aids are and what they can do. Many audiologists have come across the unfortunate situation in which a patient stopped using hearing aids because of a problem that could have been easily solved by the professional. One approach that may help to avoid this kind of problem and also help crystallize the patient's expectations is to differentiate between Absolute Expectations and Potential Benefit.
Absolute Expectations are those things that the patient should expect to be taken care of by the professional. In a sense, it is a Bill of Rights for the new hearing aid user and is in addition to the normal trial period and warranty assurances. Potential Benefit refers to those goals directly related to the hearing aid fitting that may be attainable, but could prove to be elusive. They would form the basis of the patient's criteria to determine if the hearing aids are truly meeting his or her needs.
Absolute Expectations include:
- The hearing aids should be functional on a daily basis and, if they are not working, repairs will be completed in a timely manner.
- The hearing aids should be free from feedback under normal use conditions. If feedback occurs on a frequent basis, adjustments can be made to minimize these occurrences.
- The hearing aids should be physically comfortable to wear. If discomfort is experienced, especially after the first few days of use, adjustments can be made to the physical shape of hearing aid or earmold to eliminate discomfort.
- Loud sounds in the environment should not be made to be uncomfortable by the hearing aids. If discomfort is experienced, adjustments can be made to control the output of hearing aid.
- The hearing aids should be comfortable to wear in noisier environments.
- The hearing aid should improve the ability to hear soft and conversational levels of speech in quiet environments.
Most of these Absolute Expectations relate to the side effects of the hearing aid fitting. Whereas it is true that advances in feedback cancellation technology have significantly decreased the occurrence of feedback and, through the use of open fittings, the occurrence of occlusion issues has decreased;there are still "bad" things that can happen when a person first starts to wear hearing aids. It is difficult for the patient to focus on the communication benefits provided by new hearing aids when he or she is still struggling with a fitting that is, in some way, uncomfortable or bothersome. Both Kochkin (2000) and Dillon (1999) report a strong relationship between the experience of side effects and overall satisfaction with hearing aid use. The patient needs to be informed that side effects, should they occur, will be promptly addressed. Of course it is true that under certain circumstances a negative experience such as occlusion may be unavoidable. Yet, there are many tools available within hearing aids and the associated fitting software to remedy most side effects. Before the patient can focus on what the hearing aid is doing right, every attempt needs to be made to address what the hearing aid can be perceived to be doing wrong.
Potential Benefits include:
- The hearing aids will allow the patient to better understand speech in complex, noisy situations.
- The hearing aids will improve the patient's ability to separate the various sources of sound in the environment and focus on the sounds the patient is most interested in hearing.
- The hearing aids will improve the patient's ability to understand speech from electronic sources such as telephones, televisions, etc.
- The benefits of amplification may take weeks or months to be fully appreciated as the brain needs time to adjust to new signals.
Although presenting these four points as only Potential Benefits may seem like the audiologist is lowering expectations, this approach is in line with the reality of what hearing aids can do. More importantly, it helps to clarify what the patient should absolutely expect from the hearing aids versus what the patient may hope to gain. The advantages of amplification should be framed in terms of the benefits provided rather than absolute aided performance. It also helps to frame the discussion around the value of advanced features in amplification. The majority of new signal processing approaches that currently define the mid and higher levels of hearing aid technology are focused on bringing improved benefit in the most difficult listening situations. Any good hearing aid should be comfortable, make soft sounds audible, and be free from feedback. The more advanced the technology, the greater the chances of solving the patient's most difficult problems.
What Tools Are Available?
Of course, the best way to ensure that the patient's expectations of amplification are reasonable is for the audiologist to have thorough, constructive discussions with the patient and family members. However, reflecting the comments of Nelson et al. (1997) and many others, different people learn in different ways. There are a variety of excellent tools that can be used by audiologists to supplement the discussions that they have with patients.
- COSI. The emergence of the Client Oriented Scale of Improvement (COSI) in the late 1990s marked a significant change in the use of questionnaires in the hearing aid process. Before the COSI came into use, patients would typically be given a list of specific situations and asked to indicate how much difficulty was encountered. As Dillon and his colleagues (1997) pointed out, although a patient may report difficulties in a given situation, it does not mean that the situation has any relevance or importance to the patient. The COSI requires the patient to list up to five specific situations in which there is a desire for improved communication performance. Since the patient is the one making the list, it puts the emphasis of the rehabilitation process directly on situations that have most relevance to the patient. This is an excellent tool to demonstrate that the entire hearing aid process is centered on the specific and personalized needs of each patient. Audiologists who say they don't use the COSI because they already ask the patient about specific needs may be missing the point. The value of the COSI is not in helping the audiologist keep track of the patient's nominated goals. The true value of the COSI is in what it says to the patient about the audiologist's commitment to a personalized process. There is nothing more powerful than when the audiologist pulls out the COSI form three or four weeks after the fitting and reviews with the patient whether or not his or her specific agenda is being met: "When we first met, you told me how important it was for you to be able to hear your grandchildren when they call you every Sunday on the phone. How well did it go this past Sunday? "
- Multimedia Counseling Tools. Several hearing aid companies now offer computer-based multimedia counseling tools as part of their fitting software. These tools typically use graphical and audio content to help support the education and counseling process. These programs are not designed to replace the counseling provided by the audiologist. Rather, they are designed to help explain important concepts that are easier to understand with supporting media. There is a lot for the new hearing aid user and the family members to learn about hearing aids and the fitting process. Using multiple sources of media to reinforce the same concept has been proven to be an effective teaching approach. These tools can also serve to relate the technology and hearing aids to specific COSI goals. For example, if the patient indicated a desire for better performance during conversations in a restaurant, multimedia software could be used to demonstrate how directionality is designed to work. Figure 2 provides an example of this sort of demonstration from Oticon's eCAPS software.
Figure 2. Screen shot from the eCAPS multimedia software demonstrating the effects of automatic & adaptive directionality from Oticon.
- Hearing Aid Demonstrations. Audiologists differ on their willingness to use live demonstrations when recommending hearing aids. Some are concerned that the response of the hearing aids during a demo may not accurately reflect what the patient will experience once the full fitting process has taken place. Others will attest to the power of demonstrating the significant improvement in audibility that hearing aids offer to a patient who has not heard effectively for many years. Hearing aid demonstrations can be highly motivating for the potential patient as long as the listening situations are well controlled and side effects are avoided or minimized.
- Technology Demonstrations. As a further refinement of the hearing aid demonstration process, some hearing aid fitting software allows the audiologist to demonstrate live hearing aid technology in action. For example, noise can be presented from behind the patient while speech is presented in front. During this demonstration, the software can indicate the real-time activation of directionality. Using such demonstrations requires careful set up of the sound environment. Modern environmentally adaptive circuitry in hearing aids will often be designed to respond to multiple environmental factors. If the audiologist is going to use a real-time demonstration, he or she needs to be well aware of which acoustic factors in the test environment can potentially affect device performance. When these demonstrations are executed effectively, the effect on patient understanding and motivation can be powerful.
- Patient Testimonials. One common observation in healthcare is the power of patients in knowing that they are not the only one experiencing a given condition. To that end, patient testimonials can be an effective way for the prospective hearing aid user to see what real people in the same situation have experienced. Audiologists know the typical problems faced by patients with sensorineural hearing loss and there is a lot of commonality in the situations that cause the most problems. However, the prospective first-time user may not understand that. He or she may not realize that other people who wear hearing aids also have difficulty in restaurants, parties, and other complex listening situations. To see or hear the words of other real patients who had similar issues but felt that amplification was of benefit in those situations, can help raise the confidence of the prospective patient. Patient testimonials will also speak to the comprehensive and caring attitude taken by the audiologist and support staff. That vote of confidence can further help take the focus off of the hearing aids themselves and onto the professional care offered by the audiologist.
When They Leave the Office . . .
Despite the audiologist's best attempts to portray a knowledgeable and caring attitude to patients, once the patient leave the professional's office doubt can creep in. If patients are hesitant or confused about obtaining hearing aids at the initial visit, they will be at risk of changing their minds once they have left the professional's office. Of course, all patients have the right to decide to back out of a hearing a purchase. There are techniques, however, that can be used to help patients maintain a positive attitude between the time they order the instruments and are fit with them, and even during the first several days or weeks after the fitting.
Counseling the patient and family members about new hearing aids is, in many ways, an educational process. Nelson et al. (1997) lay out the important action steps in patient education. They emphasize that different people learn best via different media and that take-home;tangible materials can go a long way to reinforcing messages communicated in counseling sessions with the professional. Tangible items would include hearing aid brochures, literature describing the audiologist's office and services, and other generic materials about hearing loss and hearing aids.
One take-home piece that has proven to be valuable is a consumer guide called Hearing Loss and Hearing Aids: A Bridge to Healing by Dr. Richard Carmen. This 100 page books provides a wealth of information for the new hearing aid user. It provides a positive, yet realistic, view of what it takes to effectively adjust to new amplification. It not only addresses the practicalities of hearing aids, but also the emotional and adjustment issues patients are likely to face.
Patients should be strongly encouraged to contact the audiologist's office with any questions they have. In fact, there is value in having the audiologist or staff member initiate phone contact during that intervening period. Again, the goal is to avoid any misconception on the part of the patient or family that may lessen motivation. Although audiologists deal with hearing aids on a daily basis, the prospect of being fit with amplification for first-time user can be a big deal. The one or two week period between when a patient orders new hearing aids and when the fitting takes place leaves plenty of opportunity for new questions to arise. Audiologists should ensure that they are the ones providing inquisitive patients with the very best information, especially in this age of the Internet. An open invitation to contact the audiologist's office with questions also reinforces the high level of service provided by the professional.
Final Thoughts
Although patients may enter the hearing aid process with hesitancy and perhaps even some suspicion, data over the years indicates that it is reasonable for most patients to expect benefit from amplification and a satisfactory outcome. Both the patient and the professional have important roles to fill in order to achieve these ends. The professional needs to convey a personalized interest in the patient's needs and challenges. Even though hearing aid technology and our clinical processes are designed to create a good generalized solution for the patient with sensorineural hearing loss, there are many steps that the professional can take to personalize this process. The patient needs to recognize that success may very well hinge on his or her willingness to take ownership of the process.
Sensorineural hearing loss is a great challenge for patients. The nature of the disorder is such that amplification, in most cases, cannot provide a complete solution. The audiologist does not need to apologize for this reality. However, empathy is in order and, more importantly, projecting a caring, involved attitude can go a long way to helping patients realize the full benefit of new hearing aids.
References
Antonucci, T. (2001). Social Relations. In J. Birren & Schaie (Eds.), Handbook of the Psychology of Aging. (pp. 427-453). New York: Academic Press.
Carmen, R. (2009). The consumer handbook on hearing loss and hearing aids: A bridge to healing. Sedona, AZ: Auricle Ink.
Cox, R.M. & Alexander, G.C. (2000). Expectations about hearing aids and their relationship to fitting outcome. Journal of the American Academy of Audiology, 11, 368-382.
Cox, R.M., Alexander G.C., & Gray G.A. (1999). Personality and the subjective assessment of hearing aids. Journal of the American Academy of Audiology, 10, 1-13.
Dillon, H. (1999). Measuring the outcomes of a national rehabilitation program: Normative data for the Client Oriented Scale of Improvement (COSI) and the Hearing Aid Users Questionnaire (HAUQ). Journal of the American Academy of Audiology, 10, 67-79.
Dillon H, James A, Ginis J. (1997). Client Oriented Scale of Improvement (COSI) and its relationship to several other measures of benefit and satisfaction provided by hearing aids. Journal of the American Academy of Audiology, 8,27-43.
Kochkin, S. (2005). MarkeTrak VII: Hearing loss population tops 31 million people. Hearing Review, 12(7), 16-29.
Kochkin, S. (2000). MarkeTrak V: Consumer satisfaction revisited. Hearing Journal, 53(1), 38-55.
Garstecki, D. & Erler, S. (1998). Hearing loss, control, and demographic factors influencing hearing aid use among older adults. Journal of Speech, Language, and Hearing Research, 41, 527-537.
Nelson, A., Wood, S., Brown, S., Bronkesh, S. & Gerbarg, Z. (1997). Improving patient satisfaction now. New York: Jones & Bartlett.
Schum, D. (2009, February 10). Motivating the older patient to take action. Audiology Online, Article 12969. Direct URL: /ceus/preview_text_course.asp?class_id=12969
Retrieved April 7, 2009 from the Articles Archive on https://www.audiologyonline.com
Schum, D. (1999). Perceived hearing aid benefit in relation to perceived needs. Journal of the American Academy of Audiology, 10, 40-45.

