
Figure 1. The IMC process is circular and data driven, using database information to link consistent and continuously refined messaging and dialog with target markets in an accountable manner. IMC can use any mix of MC components (center box), depending on the audiology practice
This is the fourth and final article in a series discussing steps in the Integrated Marketing Communications (IMC) process. The steps are shown in Figure 1. Although IMC is a continuous, circular process, without beginning or end, this series began with a discussion of software applications to support IMC, progressed to consider questions of branding to target markets, and then emphasized the importance of identifying and cultivating particular groups within those markets.
This series of articles now ends with a discussion of IMC as a strategic process for integrating software, branding opportunities, and customer relations to spread a controlled, consistent message. Every successful audiology practice must ensure that its message permeates all aspects of its practice, that it is present in all messages sent and received by the practice through all marketing communications channels, and that it is received and understood by targeted markets. IMC requires that everyone in the practice "breathe the brand" to build the brand; otherwise, the brand erodes. Foltner (2006) succinctly summarizes the in-office integration of IMC that builds audiology brands:
In an audiologist's office, every time an employee picks up the phone or greets a patient, the person's attitude and style must be in sync with his or her desired image, who that person is, and what he or she stands for—and behind. The description of who and what the audiologist and practice want to be is represented by every single employee of the practice during every patient encounter.Why is such obsessive, even slavish, attention to message necessary for building successful practices? Consider the facts of Table 1, which show that service providers (including audiologists) are performing and charging for marketing activities associated with service delivery. What we do is not about hearing instruments - that is a parity market in which a few manufacturers are rapidly incorporating each other's innovations and speedily distributing exceedingly similar product lines through a variety of distribution channels. Differentiation in a dispensing practice can only be logistical (efficiency) and by the practice's communications. A good Customer Relationship Management (CRM) set up takes care of the logistics, and all successful practices will take this step, if they haven't already(see Part I of this series, at www.audiologyonline.com/articles/article_detail.asp?article_id=1630). With the logistics solved, the only differentiation between you and everyone else is your message, and "the only real value of [your] brand lies within the consumer's belief system about the brand. What they believe, whether true or not." (italics added, Schultz, Tannenbaum, & Lauterborn, 1993)
- The US is the world's first service economy
- Over half of all US consumer expenditures are for services
- 25-33% of the US civilian labor force is engaged in marketing activities
- $0.50 of each dollar we spend as consumers goes to cover marketing costs
- .....improving design (form utility),
- making services/products readily accessible (place utility place and time),
- informing us about services/products (information utility)
(Etzel, Walker, & Stanton, 2004)
Table 1. US Marketing Facts.
IMC in action means creating a message, delivering the message consistently through all relevant contacts, and continuously measuring the effectiveness of the message in your target markets. "Contacts" covers a lot of ground, including "comments by family, friends, neighbors before and after product purchase; packaging; print and wireless media; signage, merchandising, treatment in the office and over the phone, customer service, return and repair policies, financial transaction handling, etc." (Schultz et al., 1993). The tactics of message delivery and measurement are not addressed in this series; however, there are a number of articles in the audiology literature that address delivery of brand messages through various contacts (c.f. Audiology Online Web Site, News & Information Tab, select "View By Topic", then Articles/Interviews/ATEs/E-Learning. Choose topic of Practice Management/Marketing/Business Issues, or go to www.audiologyonline.com/search/search_archives.asp). A comprehensive discussion of messaging strategies is beyond the scope of this article; consequently, three salient messaging strategies are described as examples of IMC strategic integration.
Strategy #1: Avoid Cognitive Dissonance
The consumer is more than confused by brands. The consumer is bored with brands... because most marketing is a communication hodgepodge. (Schultz et al., 1993)Back in the day, marketing messages were delivered using a "hypodermic approach," on the assumption that shooting information at consumers would replace pre-existing information in their minds. Marketing research disproved that approach, finding instead that consumers integrate new information into their existing knowledge base selectively, rejecting most new information when it does not "match" what they already know, or lumping new and old information into broad categories in which product differentiation is lost. The process is believed to work as follows:
Selective attention occurs when the consumer ...focuses on certain stimuli while excluding others. One study of selective attention estimates the typical consumer is exposed to almost 1,500 ads/day but perceives only 76 of the messages. Other estimates range as high as 3,000 exposures per day. Even if the consumer does notice the advertiser's message there is no guarantee it will be interpreted in the intended manner. Consumers may engage in selective comprehension, interpreting information on the basis of their own attitudes, beliefs, motives, and experiences, interpreting information in a manner that supports their own position. (Paraphrased from Belch & Belch, 2004)Messages are rejected when consumers experience cognitive dissonance: an "uncomfortable tension that comes from holding two conflicting thoughts at the same time" (Wikipedia, n.d.). In marketing, cognitive dissonance arises when brand messages are at odds with the target market's perception of the brand. Rolls Royce advertising to "beat anyone's price" or Dollar Stores announcing "ultimate luxury shopping" are examples of messages that create cognitive dissonance. Going "off message" can be devastating, as Wal-Mart realized when it moved off its low-price message early in 2006 to woo higher-end consumers. Resulting brand confusion has slowed sales and reduced corporate credibility dramatically, even though Wal-Mart quickly retreated to its original message and papered stores with "We sell for less" signs (Hudson & Zimmerman, 2006; Zimmerman, 2006).
IMC states that your message must never confuse the consumer, regardless of context or conditions. An audiology practice with a brand image of "highest quality" cannot position itself as "lowest price" in a sales promotion without creating cognitive dissonance in its market ("If they're the cheapest, how can they be the best quality?"). A practice with a high tech brand image cannot have repeated equipment failures or use a book and pencil to schedule appointments without inducing cognitive dissonance in the minds of its patients.
Use Heuristic Rules
Successful messages take advantage of sometimes-irrational rules, called "heuristics," that govern consumers' decision making and problem solving (in which cognitive dissonance is resolved). A common heuristic is "social proof," in which people emulate the thinking or behaviors of others, assuming that those people know what they are doing! For example, celebrity endorsements and patient testimonials are powerful forms of social proof used in the hearing aid industry and in practices to influence consumers, even though we know from our training that there is little sense in taking hearing aid recommendations from a celebrity. A more logical form of social proof, and possibly as effective as Huey Lewis, is getting primary care physicians to recommend your practice.
In a democracy, word of mouth (WOM) is often the strongest form of social proof. Part III of this series discussed special people who promulgate WOM effectively. Strategic communication with such people is critical. When a practice's message is correctly received by influential consumers and passed on without distortion to others, that practice is effectively using the social proof heuristic to eliminate cognitive dissonance for all concerned. Part III of this series also described a group of influential people known as "persuaders" - likeable, up-beat people that others depend on for social proof to solve problems and resolve cognitive dissonance. Likeability can be measured for messages as well as people*. Before broadcasting a message to brand your practice, it makes sense to test the message by having a sample group of customers score it for likeability.
Advertising and Other MC
Advertising, follow-up, and written information are important post-purchase means of reducing cognitive dissonance. Follow-up is discussed below in Strategy #2; merchandising in Strategy #3. Although audiologists (and others) tend to use advertising to increase awareness and acquire new patients, one of the most important advertising strengths is to reinforce choices and ensure customer retention. Patients who purchase hearing aids from a practice tend to select information that supports their choice and avoid information that raises doubts. As part of that process, they are likely to develop feelings of loyalty toward the practice and may even develop negative attitudes toward other practices. When patients see or hear media advertising for "their" practice, it reinforces their loyalty. Likewise, seeing or hearing media advertising for other practices may have the added benefit of providing a comparison in your patients' minds that is favorable to you and unfavorable to the advertised practice.
Strategy #2: Emphasize Customer Service (CS)
Value is created by consumers balancing product benefits (functional (ease of use), aesthetic (cosmetics), and/or psychological (peace of mind)) versus costs (money, time, learning, habit changes, repair/replacement). (Etzel et al., 2004)Duncan (2002) refers to CS as the "seat belt of brand relationships." Strategic use of CS allows practices to differentiate and create a competitive advantage over other local practices by doing a better job of creating value for their target markets. CS is also a proactive means of ensuring customer retention by anticipating patients' needs so that they do not feel the need to look elsewhere for information and solutions (a form of cognitive dissonance).
Good CS is fast becoming a necessity for practice survival for at least two reasons: the sophistication of digital products means more training for many users; increased competition in the marketplace is causing customers to expect additional, better, and faster CS as requisites for establishing and maintaining relationships. Research shows that consumers in the United States will quit a business if they encounter two negative customer relationship experiences (Two Strikes and You're Out, 2006). There is no strong reason to suspect that audiology practices are exempt from this finding.
In this series of articles, loyal, "high-value" customers have received most of the emphasis. Part III even argues for identifying and minimizing some negative-value customers. However, all customers have value when it comes to designing CS. Strategically implemented CS anticipates complaints from all sources, with patients usually comprising the largest percentage. Positive CS efforts to deal with dissatisfied patients are likely to yield high customer retention rates - as high as 87% in one study (Weiser, 1995). Why anticipate and seek out complaints? A study by the Research Institute of America found that 96.7% of unhappy customers did not complain to the company, but told nine other people about their unsatisfactory experience. In addition, 90% of the unhappy customers did not purchase from the company again (Duncan, 2002). Assuming these findings generalize to audiology, practices must devise strategic IMC recovery processes to actively search out failures, identify and resolve the problems, and retain those customers by converting them from dissatisfied to satisfied. Audiology readers are referred to a series of articles and seminars by Gyl Kasewurm (2006a & b; 2007), a CS expert, who has built her own brand by repeatedly exhorting audiologists to offer exceptional CS. She offers several case-in-point examples in her articles and presentations.
CS activities that focus solely on active patients produce self-congratulatory results of little value, as feedback is heavily skewed toward the "satisfied" end of the scale. Nevertheless, satisfied customers are an important part of good CS, which must look for compliments as well as complaints. IMC directs practices to collect compliments and suggestions to identify their markets' perceptions of the practice's strengths and competitive advantages. Using customer communications data to validate brand efforts gives practices valuable feedback, which can be used as social proof to leverage its brand image in the marketplace.
Avoid the "Fax Effect"
Effective CS programs must be proactive. As an example familiar to most of us, Starbucks uses survey forms at the point-of-service to capture real-time customer feedback. At the same time, CS strategy must avoid the risk of becoming invasive, annoying, or immunizing to consumers. For example, it seems logical from an IMC perspective to collect e-mail addresses and communicate with patients and referral sources via the Internet, given the fact that 62% of Americans are using the Internet to access health information (Silance, 2006). However, e-mailing is fast becoming the new "fax effect" in which the lowest cost channel is used to reach the most people. When consumers are deluged with a low-cost, wide-range channel such as fax or e-mail, they become immunized. They either throw or click it away, and the message is not only lost, but the associated brand loses credibility. Similar effects, although more annoying and invasive than e-mail, occurred with telemarketing, which is 50% less effective in today's market than it was in the 1970s.
Strategy #3: Make all Marketing "Consistently Sticky"
"There is a simple way to package information that ... can make it irresistible. All you have to do is find it." (Gladwell, 2002)As discussed in Part II, Holiday Inn Express (HIE) marketers had to "outsmart instead of outspend" to differentiate themselves from other hotels. They succeeded on a limited budget by developing a consistent brand message that "stuck" in people's minds ("you'll feel smarter"). The HIE campaign used television advertising, which is a low-involvement medium that requires heavy repetition of a simple phrase (e.g., "Where's the Beef?") to get its point across. TV is not a sticky medium unless you have a great phrase and a lot money budgeted (by audiologist's standards) for advertising. Being sticky is more about strategy than it is about big budgets or clever phrases. Sticky messages present simple ideas in ways that show people how your brand "fits" into their lives. Really sticky messages show people how brands can make their lives better. Stickiness is often small and subtle, not always clever like the HIE brand efforts. Here are some sticky ideas:
- Readable maps on referral forms and on yellow page ads
- "Ask an Audiologist": a three-word alliteration that informs consumers we exist, lends credibility, implies trust, makes us seem friendly and accessible, and fits us into consumers' lives by handing them control of when and what they ask us.
- On-site merchandising: displays, brochures, and other information that is readily accessible throughout a practice can help consumers make decisions. For example, incorporating customer service data acquired from satisfied customers (as discussed in the previous section) into practice brochures, slogans, bulletin boards, etc., is a good way to use social proof in your merchandising.
- Using products and merchandising to stimulate problem recognition: hearing aid or cell phone purchases can lead patients to recognize a need for infrared and Bluetooth devices, especially if you have pictures, testimonials, or actual patients in the office using the devices as social proof to influence other patients.
- Southwest Airlines (SWA) "DING": consumers can download this program which sends them a "DING" and a pop-up whenever SWA has a promotion that fits their profile. Customers click the pop-up at their convenience. Besides staying in touch with customers, the "DING" avoids the fax effect and is a consistent, friendly reminder of the SWA brand and how it fits consumers' lives and needs. Audiology practices could use variations on this idea to send "sliver" target emails containing celebratory messages for patients' birthdays, practice events, etc.
- Sticky is not confined only to words. It can be colors or sounds that support and extend a practice's brand image. It is strategic to integrate color consistently into your media messages, your waiting room, and personal presentations. Colors elicit specific emotional and/or physiological reactions, and consumers make split-second decisions based on color (Malone, 2006). As Figure 2 suggests, a practice that brands itself as "high-end, total solution" may create cognitive dissonance if it uses bright yellows and greens (prompting patients to feel the need to get moving and produce something). The same practice may reinforce its brand if it adopts blues, teals, and magentas in its décor (prompting patients to relax, enjoy themselves, and put themselves in your hands).
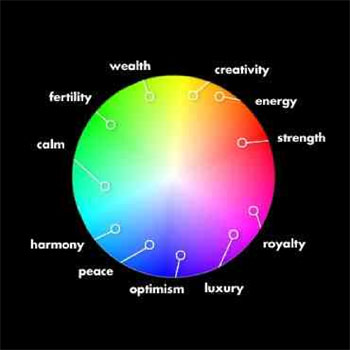
Figure 2. What color is your brand?
- Packaging: Hearing aid manufacturers do an excellent job creating beautiful and functional presentation packaging. Few audiologists have difficulty distinguishing Oticon's sticky packaging from that of other hearing aid brands. But, how many consumers can distinguish your packaging from that of your competitors? Do you even have your own packaging? Packaging is an obvious means of saying "you and only you" in a sticky way. This is especially important because it is the final stage of the financial transaction. When the patients accept your package, they are taking possession of hearing aids and making them their own. Your brand, above all others, should be intimately associated with that important act of acceptance.
- Sponsorships: This form of publicity, discussed in Part II of this series, is mentioned here because of the stickiness of "cause marketing" for audiologists and other hearing-health professionals. Careful selection and wholehearted support of a worthy health cause is a natural and sticky message to consumers that your practice is dedicated to supporting health-related issues and those in need.
- "Give Good Store." This is Paco Underhill's (1999) way of saying "make the entire personal selling experience great for the customer." The phrase is a form of POP (Purposeful, Original, Pithy) language which uses catchy, imaginative phrases and metaphors to communicate messages that stick. For example, an audiologist might describe listening to music with digital hearing aids as "sitting front row and center at the symphony."
- Your place of business: You know your IMC has gone deeply awry when a patient writes you a large check for high-end digital hearing aids but leaves the payee line blank because they don't know the name your "hearing aid place." Besides POP, Underhill's message in the previous bullet is sticky because it points out the obvious; our offices are our best vehicle for getting our branding message across (including our name!), if we take advantage of it. What does your office look like to an outside observer walking or driving past? What message does it send to the postman, the FedEx delivery person, the retirement-center bus driver, or the personal assistant accompanying your patient? Does the outside and inside of your office send a positive, sticky message that cements your brand in their minds? Or, do any of these people leave without remembering your name or your office?
Lest it is lost in the integration, it is important to recall that the ultimate purpose of all IMC activities is to achieve stated objectives, chief among which is profitability. No matter what strategies and tactics are adopted for marketing a practice, IMC requires that marketing efforts must be accountable and open to change, especially for companies who now find themselves in a competitive market. That means that they must be measured and those measurements must demonstrate a Marketing Return on Investment (MROI) that meets pre-set business objectives. If the MROI does not meet objectives, it has failed and needs to be discarded or revisited. Cost effective measurements that have relevance to audiology practices include surveys and questionnaires directed at consumers, patients and referral sources that measure brand awareness, brand knowledge, and satisfaction.
Conclusion
A long-time patient recently asked me how people know where to go for hearing help, since "there's a hearing aid store on every corner." We are in the midst of a rapid revolution in the marketplace, where traditional supply-driven markets are giving way to markets of abundance in which consumers have choices galore and exercise their power to choose (Anderson, 2006).
Consumers today acquire information on demand, and only when they need or want it. They skip elaborate marketing campaigns rolled out in traditional media, and instead point and click or check their cell phones to find what they want, ignoring scads of information and offers that are outside their targets. It is intriguing that our target markets have turned it around and made our messages and brands their targets. In such a scenario, social proof has high value, and WOM is powerful. We no longer control our message distribution, but we can control the likelihood that our messages will be processed and adopted by consumers. We can do this by using IMC to deliver a consistent, comprehensive, and likeable message. The present article has discussed controlling the message with a few IMC strategies to eliminate cognitive dissonance, capitalize on social proof, concentrate on customer-centric solutions, and bond practices with their target markets.
Editor's Note
This article, focusing on strategic messaging to build brand, is the forth in a series of four papers examining Integrated Marketing Communications (IMC). The series was written by Dr. Holly Hosford-Dunn, an Audiology Online Contributing Editor in the area of Practice Management. The first article in this series, focused on Customer Relationship Management (CRM), was published in July, 2006 on Audiology Online and can be accessed via the Articles Archive or directly by the following URL:
www.audiologyonline.com/articles/article_detail.asp?article_id=1630
The second article was published in December, 2006 on Audiology Online on the topic of strategic messaging to build brand, can be accessed via the Articles Archive or directly by the following URL:
www.audiologyonline.com/articles/article_detail.asp?article_id=1732
The third article was published in March, 2007 on Audiology Online on the topic of acquiring and retaining customers. It can accessed via the Articles Archive, or directly at
/articles/integrated-marketing-communications-imc-part-952-952
Footnote
* Here's an example of a "Likeability Questionnaire" from Jones & Ince (2001) in which subjects use a scale of 1 (strongly disagree) to 5 (strongly agree) to rate aspects of likeability as well as overall likeability of a person.
If I were to give this person a grade it would be a(n)_____
- I would be interested in getting to know this person better.
- I believe this person is probably mean.
- This person seems like someone that I would hang out with.
- This person seems like they would be good to go to with a problem.
- This person seems really nice.
- I don't think this person can be trusted.
- I think this person is very intelligent.
Anderson, C. (2006). The Long Tail. New York: Hyperion.
Belch, G.E., & Belch, M.A. (2003). Advertising and promotion. An integrated marketing communications perspective (6th Ed). New York: McGraw-Hill/Irwin.
Duncan, T. (2002). IMC: Using advertising and promotion to build brand. New York: McGraw-Hill Irwin.
Etzel, M.J., Walker, B.J., & Stanton, B.J. (2004). Marketing (13th Ed). New York: McGraw-Hill/Irwin.
Foltner, K. & Mansfield, B. (2006). Branding audiology: It's a budding opportunity. The Hearing Journal, 59(5), 41-44.
Hudson, K. & Zimmermann, A. (2006). Wal-Mart demotes price-slashing 'smiley' in new ads. Wall Street Journal Online. Retrieved February 8, 2007, from brandkeys.com
Jones, D.N. & Ince, E. (2001). The effects of cognitive dissonance on interpersonal perception and reassertion. Current Research in Social Psychology, 7(4). Retrieved January 14, 2007, from uiowa.edu
Kasewurm, G. (2006a). Being outrageous! Audiology Today, 18(5), 43.
Kasewurm, G. (2006b). It's all about relationships. Audiology Today, 18(4), 35.
Kasewurm, G. (2007, January 18). Improving Patient Retention in Your Practice. Audiology Online, Recorded Course 7786. Retrieved February 7, 2007, from audiologyonline.com
Malone, T. (2006, February). Marketing color to the young and the restless. Symposium conducted at the American Gem Trade Association, Tucson, Arizona.
Schultz, D.E., Tannenbaum, S.I., & Lauterborn, R.F. (1993). The New Marketing Paradigm. Integrated marketing communications. Chicago: NTC Business Books.
Silance, T. (2006). Embracing the internet age. The Hearing Review. April, 32.
Two Strikes and You're Out. (2004). Marketing Management, 13(5), 5.
Underhill, P. (1999). Why we buy: The science of shopping. New York: Simon & Schuster.
Weiser, C. (1995). Championing the customer. Harvard Business Review, Nov-Dec, 113-116.
Wikipedia (n.d.). Cognitive dissonance. Retrieved January 14, 2007, from en.wikipedia.org
Zimmerman, A. (2006). To Boost Sales, Wal-Mart Drops One-Size-Fits-All Approach. Wall Sreet Journal Online, Retrieved February 8, 2007, from wsj.com

